The Prevalence and Correlation of Bruxism with Stress and Aggression
Aim and Objectives: This study aims to investigate the relationship between bruxism, stress, and aggression in forensic settings and its psychosocial impact on people’s psychological health. It also seeks to examine the potential benefits of raising awareness about bruxism for a more thorough forensic evaluation and its relationship with gender, age, occupational stress, and high-performance sports. Background: Bruxism is a dental condition that often goes unnoticed. It can cause tooth fractures, joint issues, and tooth sensitivity. Bruxism is linked to personality traits like aggression, emotional suppression, and stress. Stress sensitivity can lead to forceful muscle contractions, affecting one’s quality of life and ability to keep up with responsibilities. Materials and Method: A study was conducted in three phases at Parul University. First, 150 individuals were screened based on psychological status and bruxism history. Second, 60 out of 150 participants underwent an extraoral examination, and finally, an intraoral examination was conducted. The study used a Google form for screening, a modified Likert scale questionnaire to measure stress, and a staging chart by Li and Ji to analyze molars. Result and Conclusion: This study collected quantitative data and analyzed it using descriptive statistical methods and Spearman correlation. The aim was to investigate the relationship between attrition levels and stress-related factors such as aggression, bruxism, age, and gender. The results showed a complex interplay among stress, aggression, and bruxism, but no strong correlation. Age was found to be significantly correlated with attrition, while gender had no significant relationship with high-performance sports.
Introduction
Bruxism is a parafunctional behaviour characterized by non-functional tooth grinding or gnashing. It is influenced by various factors, including anatomical characteristics like dental occlusion and the structure of the stomatognathic system’s bony structures. Other etiologic factors include illnesses, trauma, heredity, alcohol and/or tobacco use, caffeine consumption, illegal drug use, and prescription drugs. Psychosocial factors, central factors, unique neurotransmitters, sleep disorders, and dopaminergic system involvement also contribute to bruxism. No one treatment works for everyone, and the cause, diagnosis, and treatment of bruxism are not fully understood due to the potential overlap between abnormal and normal clenching.
According to the American Academy of Orofacial Pain, bruxism is defined as: Bruxism is a parafunctional behaviour that can occur during the day or night and manifests as teeth clenching, bracing, gnashing, and grinding [1]. In 1907, Marie and Pietkiewicz created the term “bruxism” or a term similar to it, calling it “bruxomania”[2].
Several things can lead to attrition, such as habitual teeth clenching and grinding (bruxism) and regular chewing and grinding. The degree of tooth attrition varies from person to person and is influenced by things like personal habits, dental hygiene, and diet. Excessive attrition can occasionally result in issues like tooth sensitivity, altered bite patterns, or even structural damage to the teeth. Chronically being around dust and dirt can also make humans more worn down [3].
People who experience ongoing stress may forget to practice good dental hygiene, like brushing and flossing regularly. This may result from an increased risk of cavities, gum disease, and other dental problems. The emergence of mouth sores and ulcers can be attributed to stress.
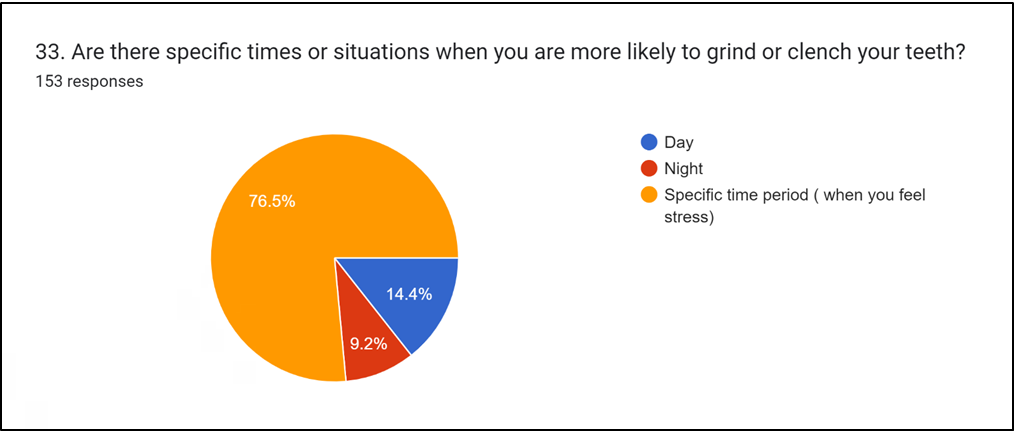
Bruxism is a common condition characterized by an outward manifestation of stress, often triggered by personality traits such as aggression, emotional suppressions, and stress. People with bruxism often exhibit anxiety and neuroticism, which can lead to a range of physiological reactions. The most common cause of seeking medical attention is pain, which occurs when muscles and temporomandibular joint structures cannot adjust to the environment. Excessive stress sensitivity is a significant difference between individuals with bruxism and the control group. Anxiety and a mindset towards success are key factors in the development of bruxism. Prolonged stress can overstimulate muscle receptors, causing masseter muscles to contract more forcefully and uncontrollably [4]. Studies have shown a link between stress and bruxism, particularly in university students. Students may either learn to manage stress in their university setting or remain oblivious to its harmful effects. Stress is increasingly considered a trigger, risk factor, and sustaining factor for bruxism, though it remains unclear how these factors are implicitly related. Painful temporomandibular disorder (TMD) is associated with bruxism, and the type of traumatic event can affect the likelihood of developing these conditions. Most people believe stress plays a role in bruxism, including sleep bruxism, based on an early case series that showed a connection between increased nocturnal masseter muscle activity and stressful everyday events [5, 6, 7, 8].
Rationale
Based on the literature review done so far, it can be inferred that the research gap is between the correlation between bruxism and the psychological status of an individual. Thus, the formulated research question is whether bruxism is used to determine the psychological status of an individual as compared to stress and aggression.
Based on the formulated research question, the null hypothesis will be that Bruxism does not correlate with stress and aggression, and cannot be used as a method to assess a person’s psychological status. Whereas, the alternative hypothesis will be that Bruxism has some correlation with stress and aggression and can be used as a method to assess a person’s psychological status. The main aim of this study is to verify and establish the correlation between bruxism with stress and aggression.
Materials and Methods
A study was conducted at Parul Institute of Applied Sciences, Parul University in Waghodia, Vadodara and Gujarat from September 2023 to March 2024. The study aimed to investigate the prevalence of bruxism in adults aged 18 to 40 and its correlation with stress and aggression-the research aimed to understand bruxism in different professions and its relationship with psychological variables and dental health.
Sample Collection
Approximately 150 samples have been taken which include 32 female and 28 male individuals and people indulging in high-performance sports and other professions which can create stress as a possible cause for bruxism. The method of stratified random sampling has been employed to select the participants, guaranteeing representation of various demographics such as age, gender, and socioeconomic status.
Materials used for the examination purposes were-an occlusal mirror and a mouth mirror.
Procedure
Screening
At the outset, participants were required to fill out a series of questionnaires to determine their eligibility to progress to the next stage. They were then asked to complete a Google form detailing their recent observations over the past 1-3 months. The questionnaire utilized a modified version of the Likert scale, specifically the Perceived Stress Scale, and was divided into four distinct sections [9, 10].
- The Google form begins by asking for the person’s name, gender, and age, followed by questions related to their behaviour. These questions include (Table 1).
- Do people often think you get angry easily?
- Do you feel like hitting a person if they annoy you?
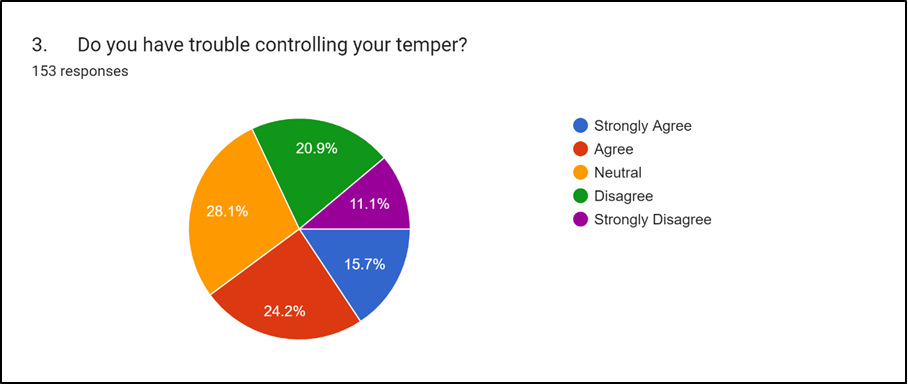
- Do you have trouble controlling your temper?
- Do you get angry frequently?
- Do you get angry quickly but get over it quickly?
- Do people say you are argumentative most of the time?
- Do you get annoyed if things are not in favor of you or not getting enough?
- Do you like overly friendly strangers?
- Do you get angry for no reason?
- Do you disagree with people frequently?
- Do you not like if a person is bossy?
- Do you often get anxious about thinking people are talking behind you?
- Do you feel relaxed if you show your irritation?
Table 1: Behavioral Questions.
- These questions helped us understand how participants deal with stress and anger. We had asked them to see how they react to unfavorable situations that can cause these emotions. The second section of the Google form was designed to collect more detailed information about the
- In the last month, how often have you been upset because of something that happened unexpectedly?
- In the last month, how often have you felt that you were unable to control the important things in your life?
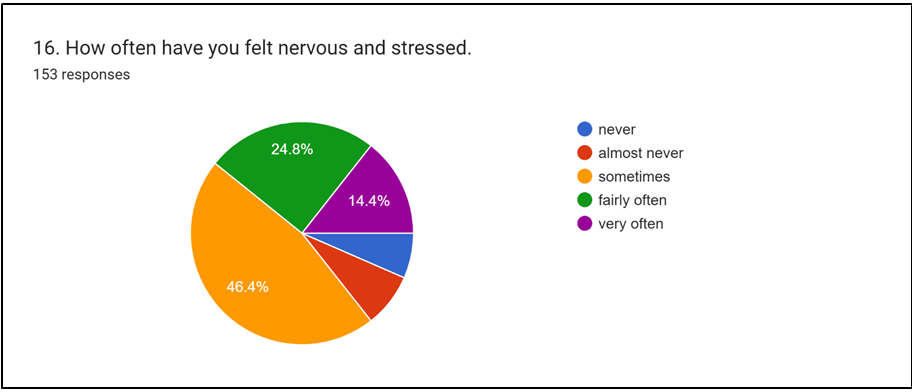
- How often have you felt nervous and stressed?
- How often have you been angered because of things that happened that were outside of your control?
- How often have you felt difficulties were piling up so that you could not overcome them?
- Have you felt ongoing academic pressure is causing stress?
Table 2: Questions to asses stress level.
12. Do you often get anxious about thinking people are talking behind you?
14. In the last month, how often have you been upset because of something that happened unexpectedly?
attrition level
15. In the last month, how often have you felt that you were unable to control the important things in your life?
17. How often have you been angered because of things that happened that were outside of your control?
18. How often have you felt difficulties were piling up so that you could not overcome them?
16. How often have you felt nervous and stressed?
attrition level 1
12. Do you often get anxious about thinking people are talking behind you?
-0.07611 1
14. In the last month, how often have you been upset because of something that happened unexpectedly?
-0.2456 -0.21968 1
| 15. In the last month , how often have you felt that you were unable to control the important things in your life? | -0.16314 | -0.16211 | 0.315955 | 1 | |||
|---|---|---|---|---|---|---|---|
| 16. How often have you felt nervous and stressed. | 0.004202 | -0.3173 | 0.187571 | 0.307314 | 1 | ||
| 17. How often have you been angered because of things that happened that were outside of your control? | -0.04431 | -0.19729 | 0.170235 | 0.545572 | 0.490377 | 1 | |
| 18. How often have you felt difficulties were piling up so that you could not overcome them? | -0.03607 | -0.38218 | 0.266412 | 0.385167 | 0.412248 | 0.351206 | 1 |
Table 3: 1: Coefficient value of Spearman’s correlation between attrition level and questions related to stress.
The following questions were designed to evaluate how an individual expressed their aggression in the past: (Tables 3 & 3.1).
Do you tend to break things when you are angry? Does Showing off the aggression help you to cool your temper?
After hitting others, do you feel better? Do you often slam the door when leaving because you are angry?
| attrition level | social status | social factors | anger management | impulsive behavior | short temperedness | defiant behaviour | vexed nature | cautious | irritability | disability | rebellious nature | cooling down | sabotaging nature | aggressiveness | physical aggression | passive aggressiveness | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| attrition level | 1 | ||||||||||||||||
| social status | -0.11 | 1 | |||||||||||||||
| social factors | 0.08 | 0.23 | 1 | ||||||||||||||
| anger management | -0.05 | 0.43 | 0.11 | 1 | |||||||||||||
| impulsive behavior | 0.08 | 0.39 | 0.22 | 0.43 | 1 | ||||||||||||
| short temperedness | -0.01 | 0.34 | 0.12 | 0.19 | 0.35 | 1 | |||||||||||
| defiant behaviour | -0.03 | 0.29 | 0.27 | 0.31 | 0.3 | 0.35 | 1 | ||||||||||
| vexed nature | 0 | 0.13 | 0.43 | 0.11 | 0.4 | 0.36 | 0.5 | 1 |
Table 4: 1: Coefficient value of Spearman’s correlation between attrition level and questions related to bruxism.
- cautious
- -0.17 -0.11 -0.05
- 0.15
- 0.1
- 0.19
- 0.12 -0.06
- 1 irritability
- 0.12 0.26 0.12
- 0.26
- 0.59
- 0.21
- 0.1
- 0.29 0.12
- 1 disagreebility 0.29 0.01 0.12
- 0.1
- 0.32
- 0.09
- 0.08
- 0.13 -0.09 0.45
- 1 rebellious nature
- -0.24 -0.05 0.23
- 0.09
- 0.3
- 0.09
- 0.22
- 0.29
- 0.1
- 0.12 0.08
- 1 cooling nature 0.03 0.16 0.07
- 0.12
- 0.33
- 0.08
- 0.27
- 0.26 -0.01 0.3
- 0.17 0.02
- 1 sabotaging nature
- 0.16 0.08 0.21
- 0.27
- 0.33
- 0.11
- 0.04
- 0.19 -0.1 0.32 0.23 0.11 0.05
- 1 aggressiveness 0.05 0.18 0.21
- 0.23
- 0.39
- 0.07
- 0.04
- 0.19 -0.21 0.2
- 0.26 0.24 0.35 0.47
- 1 physical aggression
- 0.13 0.12 0.49
- 0.13
- 0.3
- -0.05
- 0.1
- 0.17 0.09 0.25 0.36
- 0.1 0.47 0.24
- 0.37
- 1 passive aggression
- 0.24 0.19 0.08
- 0.27
- 0.39
- 0.16
- 0.12
- 0.25 -0.12 0.34
- 0.4
- 0.15 0.3
- 0.53
- 0.35
- 0.44
- 1
Table 5: 1: Coefficient value of Spearman’s correlation between attrition level and questions related to aggression.
- Finally, the person would have been asked about any previous instances where they knowingly or unknowingly experienced symptoms of bruxism. The following questions would have been asked: (Tables 4 & 4.1).
- 1. Do you experience frequent jaw pain?
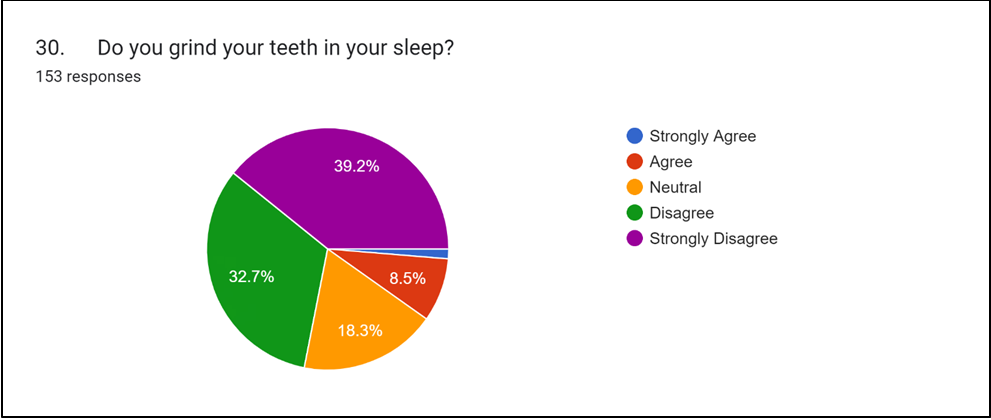
- 2. Do your partner, friend, or family members complain about you grinding your teeth in your sleep?
- 3. Do you clench your teeth when you are angry?
- 4. Do you feel jaw pain while asleep when you are feeling depressed?
Table 6: Questions about occurrence and frequency of bruxism.
| 0 | attrition level | sleep bruxism | sleep discomfort | jaw discomfort | teeth chipping | dental healthcare | peer response | unusual jaw sounds | anger | mental status | aggressive clenching | sleep disturbance |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| attrition level | 1 | |||||||||||
| sleep bruxism | 0.122 | 1 | ||||||||||
| sleep discomfort | 0 | 0.546 | 1 | |||||||||
| jaw discomfort | 0.032 | 0.371 | 0.665 | 1 | ||||||||
| teeth chipping | 0.029 | 0.219 | 0.16 | 0.298 | 1 | |||||||
| dental healthcare | 0.013 | 0.351 | 0.166 | 0.209 | 0.155 | 1 | ||||||
| peer response | -0.125 | 0.587 | 0.36 | 0.363 | 0.212 | 0.324 | 1 | |||||
| unusual jaw sound | 0.054 | 0.388 | 0.529 | 0.405 | 0.01 | 0.192 | 0.414 | 1 | ||||
| anger | 0 | 0.128 | 0.31 | 0.319 | 0.218 | 0.017 | 0.279 | 0.203 | 1 | |||
| mental status | -0.031 | 0.491 | 0.542 | 0.698 | 0.349 | 0.166 | 0.437 | 0.344 | 0.35 | 1 | ||
| aggressive clenching | 0.164 | 0.382 | 0.164 | 0.29 | 0.233 | 0.366 | 0.479 | 0.302 | 0.321 | 0.558 | 1 | |
| sleep disturbance | 0.141 | 0.405 | 0.374 | 0.31 | 0.338 | 0.183 | 0.407 | 0.284 | 0.42 | 0.326 | 0.316 | 1 |
Table 7: 1: Coefficient value of Spearman’s correlation between attrition level and questions related to bruxism.
Phase-1
Extraoral Examination
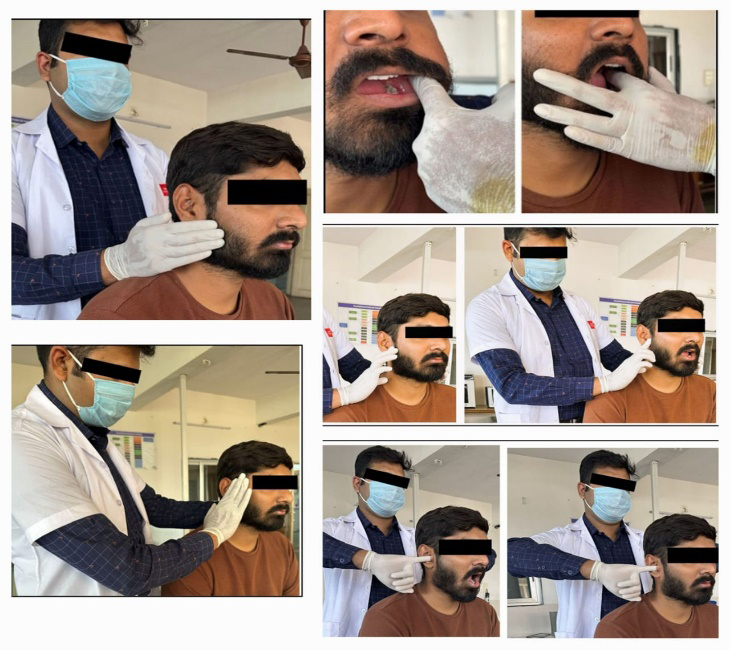
After the screening phase 60 out of 150 were asked for phases 2 and 3 based on their responses. During the examination, the facial asymmetry, masseter, and temporalis muscles were inspected. The range of mandibular movement, including maximum mouth opening and lateral movement, was also assessed. Participants were asked to open their mouths as wide as possible and report any pain during the task. A non-clinical person was trained for 15 days under the guidance of a doctor for muscle examination and sample collection.
Palpation of Temporomandibular Joint
The examination of the TMJ involves palpation of the pre- tragus area, allowing the participant to open their mouth, feel the mandible joint, and assess condylar movement. Palpation can also be done through the anterior wall of the external auditory meatus. The presence of tenderness during this process can be alarming and a sign of articular inflammation. Participants were asked about any pain they were feeling during this process. It was also designed to examine whether the pain elevated or not during the whole process [11].
2 types of joint sound should be looked for during this examination. Those are: Clicking Sound: single explosive noise of short duration. The timing of the click is also important. It should be noted whether the clicking sound is heard while opening their jaw. Crepitus: continuous grating noise. This type of noise can only be felt with the stethoscope. The main cause of this is the articular surfaces of the joint being worn.
Examination of Muscles
The most frequent complaint of TMD patients is likely related to functional disorders of the masticatory muscles. The broad category known as “masticatory muscle disorder” is typically where they are categorized. Like in any pathologic condition, there are two main signs to look out for those are pain and dysfunction.
Temporalis muscle
The anterior, middle, and posterior regions of the temporalis muscle were palpated by firmly clenching the teeth, as recommended.
Multiple Masseter Muscle
The temporalis muscle was observed when the person forcefully closed their jaw. The masseter muscle was palpated by pressing the thumb and index finger against it.
The Medial Pterygoid
The insertion of a muscle was palpated by placing one finger externally and orally in the lingual vestibule, palpating the anterior part with a 45-degree angle, and palpating the inferior and posterior parts extra orally.
The Lateral Pterygoid
Muscle was palpated. The little or index finger was placed medially to the coronoid process and lateral to the maxillary tuberosity to palpate the muscle. It is possible to detect pain when the finger presses upward and inward. The examining finger can reach the lateral pterygoid intraorally. Through this process, any type of muscle spasm and tenderness can be examined for presence in those areas [12].
The extraoral examination was done under the guidance and supervision of a certified dentist (Figure 1).
Phase-2
Intraoral Examination
The intra-oral examination was done to check teeth attrition using the modified Li and Ji method for ASA (Average Surface Attrition) with the help of an occlusal mirror and mouth mirrors. Clear photographs were taken to check the level of attrition. Using the Average Stage of Attrition (ASA) chart (stages 0–9), the attrition values of each molar cusp are noted, and an average is then computed. We used the average attrition levels of all mandibular and maxillary first [13] and second molar cusps (Figure 2).

The intraoral examination was also done under the guidance and supervision of a certified dentist.
Results
The Google form was distributed among 150 people for the screening phase. After screening, 60 individuals with symptoms of bruxism were selected for clinical examination and personal interview. The collected data was tabulated into an Excel sheet and then subjected to statistical analysis. For the statistical analysis, Microsoft Excel (version 2210) was used.
Descriptive Statistics
The datasheet comprises a total of 28 males and 32 females. The mean age of the selected 60 individuals is between 21.21 years. The youngest individual is 18 years old, while the oldest is 30. Furthermore, the mean attrition level of the selected individuals is 2.
Spearman Correlation Analysis
Spearman correlation is a statistical method used to assess the strength and direction of association between two non-parametric variables. It is particularly useful when dealing with ordinal data, as it does not require the variables to follow a specific distribution. This method calculates the relationship between the variables by ranking the data and then assessing the degree to which the ranks correspond between the two variables. It was applied to determine the correlation between attrition and various factors such as age, stress, aggression, and bruxism an additional analysis is being performed to establish a correlation between stress and aggression in this study.
Correlation between Stress and Attrition Level
The correlation coefficient measures the relationship between stress and attrition levels. Negative values indicate a negative correlation. In this case, most questions negatively correlate with the attrition level. Since the coefficient values were mostly below 0.2 it suggests that attrition level is weakly correlated with stress level. it was found that attrition level was somewhat negatively related to the stress as a result of unexpected events. This implies that in case an individual is undergoing stress as a result of any unexpected event, is less likely to clench his/or her teeth or resultant degree of wear and tear.
Correlation between Aggression and Attrition Level
The correlation coefficient between aggression and attrition exhibits a positive correlation with the question about disagreements with individuals, which possesses a value of 0.293. Based on that, we can conclude that individuals showing a higher rate of disagreement with others are likely to show more degree of attrition in teeth, suggestive of teeth clenching.
Correlation between Bruxism and Attrition Level
The observed correlation between attrition and bruxism indicates a positive association with only two specific questions, namely “sleep difficulty” and “aggressive clenching”. Based on this finding, it can be suggested that anger and sleep disturbances may contribute to the development of attrition.
Spearman’s Correlation between Attrition Level and Age
There is a positive correlation between attrition level and age with a value of 0.22 implying the fact that level of attrition or wear and tear of teeth is a marker of increasing age. Independent t-test revealed that there is a significant difference in the attrition level concerning sex change (<0.05) (Figures 3-7).
Discussion
This is a cross-sectional survey aimed at diagnosing the frequency of bruxism in adults between the ages of 18 and 40. The study also explores the relationship between bruxism, stress, and aggression while shedding light on the connection between psychological factors and dental health.
A 2021 study by Fluerasu MI, et al. [14] examined the frequency of sleep or awake bruxism in young students aged 19-30. The study involved 308 participants from Transylvania, Romania, and France. The researchers found no significant correlation between age, sex, or nationality and bruxism. However, European subjects, except Romanians and French people, experienced high levels of stress and frustration due to cultural and language adjustments. Females were more likely to experience stress, duty-related depression, and anxiety. The study used the Mann- Whitney test and Spearman rho coefficient for continuous variables [14].
Serra-Negra JM, et al. [15] study on dental students in Brazil revealed that 36.5% of them had awake bruxism and 21.5% had sleep bruxism, using descriptive analysis, Kruskal-Wallis, Mann-Whitney, and Poisson regression for statistical analysis [15].
Molina OF, et al. [16] divided bruxers into four distinct categories. Using chi-square and Fisher’s exact tests, they discovered that the percentages of people who engaged in mild, moderate, severe, and extreme bruxing behavior were 16.1%, 29.6%, 31.5%, and 22.8%, respectively [16].
A 2016 study by Cavallo P, et al. [17] found that university students in Italy experienced an average perceived stress score of 32.2, with gender differences. Women were more likely to experience awake bruxism, while men had an average score of 31.2. Sleep bruxism was prevalent at 31.8%, with no significant gender difference. A significant positive correlation was found between stress levels and awake bruxism, but only among males [17].
Nakata A, et al. [18] study found a weak association between sleep bruxism and job stress in men, based on questionnaires from 1944 males and 736 females in Japan. However, the results may be partially accurate due to higher male participation [18]. Muzalev K, et al. [19] found psychological stress to outperform sleep bruxism as a pain predictor for temporomandibular disorders [19].
The study explores the link between bruxism, stress, and aggression, focusing on attrition levels caused by stress and aggression. It suggests that stress may not always cause bruxism and differentiates between sleep and awake bruxism, despite scientific studies only partially supporting this link [20]. Sleep bruxism, a common condition triggered by stress, can only be definitively identified through polysomnographic recordings, but this method is restricted due to high costs and limited lab facilities [21]. The data is based on the self- report approaches. Studies have shown that self-reported bruxism by patients is not a reliable diagnostic tool, as it can be influenced by the patient’s and clinician’s beliefs [22]. Bruxism, whether clinically or self-diagnosed, has been linked to emotional stress, psychosomatic disorders, hostility, aggression, apprehension, and a tendency to worry [23]. It is important to note that this study only covers a specific number of students and therefore cannot be generalized to represent the entire Indian population. India is a diverse country, and the findings of this study may not accurately reflect the attitudes and behaviours towards bruxism in other regions. Nevertheless, this study can serve as a useful reference for raising awareness about bruxism in other parts of the country. Attrition can also be caused by the other factors other than bruxism such as food habits, age, or any other dental treatments. There is bias in the numerous studies that show a positive relationship between the degree of wear and self-reported bruxism [24]. A similar conclusion was drawn in a large epidemiological study, which found that self-reported bruxism contributed no more than 3% to the existence of tooth wear [25]. In a study, individuals with moderate to severe sleep bruxism (as determined by Polysomnography) exhibited minimal tooth wear, while those with minimal muscle activity displayed greater tooth wear [26].
Forensic Significances
Research on forensic bruxism is important for several reasons, including its ability to provide insight into a subject’s behaviour, mental state, and potential involvement in legal matters. The specific arguments that follow highlight how important it is to look into bruxism from a forensic perspective:
Effects on the Force of the Bite
Bruxism has the potential to impact bite force, particularly in the anterior regions of the oral cavity. A comparison of incisor bite force values indicates that individuals afflicted with bruxism exhibit higher values than their non-bruxing counterparts [27]. The variations in bite force induced by an individual’s biting behavior and the resultant impressions that they leave on objects or other persons are factors of significance in forensic inquiries.
Damages to the Dental Tissues
Tooth attrition, chipping, and cracking are only a few of the severe dental implications resulting from bruxism. Recognizing significant wear enables the identification of individuals affected by bruxism. In forensic dentistry, the analysis of wear patterns and tooth morphology allows for the determination of bruxism presence and potential association with a crime scene.
Dental and Psychological Experts
Forensic psychologists and dentists are capable of providing expert testimony in legal proceedings. Their expertise extends to offering insights into an individual’s mental health and discussing potential links between psychological stress, bruxism (teeth grinding), and aggressive tendencies. An intriguing theory posits that wake-clenching is distinctly associated with depression or possibly serves as a symptom of this condition; a concept substantiated by psychiatric literature. Additionally, this body of literature posits that individuals with bipolar disorder may experience disruptions in their central neurotransmitter systems, which could contribute to the onset of bruxism [28]. Stress and bruxism are often linked to poor sleep. Forensic investigators can analyze a person’s stress levels and sleep habits to determine if they suffer from bruxism. This information can help gain insight into the motives and actions of a criminal.
Helps in Investigation of Dental Malpractice
In a malpractice case, expert testimony is frequently needed to determine the relevant standard of care and show how the defendant violated it. Often bruxism misconceptions are perceived as medical malpractices, and in those cases, expert testimony is crucial. Expert testimony is often required in malpractice cases to determine the applicable standard of care and demonstrate how the defendant’s actions breached it. However, there are exceptions to this rule, such as in cases where the lack of professional care is so evident that a non- expert could recognize it. Bruxism, such as the type induced by the antidepressant sertraline, can also be associated with specific medications [29, 30]. This emphasizes how important it is for medical personnel to be informed about possible drug side effects and to keep an eye out for them in their patients.
Recommendation
If we consider the limitations the present study can help generate the awareness of bruxism. this helps to have a preliminary idea about bruxism stress and aggression. The participants should be observed for more than 2 years for the progression of stress along with bruxism for observing bruxism other methods can be applied for more in-depth understanding. More samples will help us better understand the seriousness of the topic. A large number of samples can enhance the accuracy of statistical analysis resulting in establishing the variations between different populations. By applying different methods for psychological screening, the data can be more specific about the stress and aggression level. Perceived stress scale, scales for anxiety, and aggression will be more effective for the assessment.
Limitations
This study includes intraoral photographs of the subjects. As it involves human participants, questions related to their psychological health are designed moderately. No direct questions were asked, which can be a limitation of this study.
The research project was assigned six months; however, it was discovered that a longer period is required to observe the manifestation of bruxism following the participants’ lifestyle. Due to the time constraints, the study was conducted solely based on the current situation of the participants, and a more comprehensive investigation was unfeasible.
Initially, many participants were unaware of the concept of bruxism. As a result, only 60 out of the 150 samples were taken, as they were unable to identify if they had the problem or not. Due to the constricted sample size the desired result was not obtained.
The history was gathered using a Google Form. While it is a commonly used tool for research studies, it has some limitations. The design customization options available are limited and may not be sufficient for researchers who require more advanced customization. Additionally, while it offers various question formats, it may not be able to generate a large number of different forms. The tool is only accessible with an internet connection, which may restrict its usability in areas with poor internet connectivity. Its file upload limitations, which include file size and format restrictions, may restrict the kinds of data that can be gathered. Finally, the complexity of the research may be restricted by the number of sections that can be included in a form often, students feel reluctant when filling out Google forms, which can lead to inaccurate data being collected. It is important to encourage students to provide honest and thoughtful responses to ensure that the data collected is reliable and useful.
The attrition can be affected by the other factors other than bruxism such as age, food habits, and previous dental procedures. The staging of attrition has been done through the chart proposed by Li and Gi. The staging from the chart can cause unreliable and unrealistic data sometimes.
To obtain a precise analysis of sleep bruxism, it is crucial to fulfil adequate laboratory requirements. However, in this particular situation, such requirements were not met, which made it impractical to accurately diagnose the condition. Before the sample collection, a dental practitioner has trained a nonclinical individual which can lead to a lack of proficiency. Sample collection was done under the supervision of a dental practitioner. This study was conducted on a diverse Indian population and is not limited to any specific region. This study was conducted on a diverse Indian population and is not limited to any specific region.
Conclusion
This cross-sectional study investigates the prevalence of bruxism among young and adult individuals in India and the connection between stress and aggression. It found that awake bruxism is often linked to aggression, while stress and anxiety are primarily linked to sleep bruxism. However, due to limited laboratory facilities, an in-depth examination of sleep bruxism was not possible. The study aims to gain a preliminary understanding of bruxism and increase student awareness. Participants from different age groups and professions, such as teachers, doctors, and administrative workers, exhibited high levels of attrition due to their bruxism habit. No significant correlation was found between bruxism and high-performance sports. Stress and aggression can be attributed to bruxism, with obsessive, domineering, or violent personalities more likely to develop the condition. Work stress and erratic schedules can worsen bruxism. The study aims to understand the dynamicity of bruxism in determining personality traits, anxiety, and psychological health.
Declaration
Author 1 has participated in the conception and design, analysis, and interpretation of the data, author 2 has participated in drafting the article or revising it critically for important intellectual content; and has approved the final version. This manuscript has not been submitted to, nor is it under review at, another journal or other publishing venue. The authors have no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the manuscript. The following authors have affiliations with organizations with direct or indirect financial interest in the subject matter discussed in the manuscript.
Ethics Approval and Consent to Participate
The given manuscript is a research article. Therefore, there is no requirement for ethical approval or participation consent.
Consent for Publication
Since the given article manuscript is a review article, there is no requirement for consent for publication. The author gives full consent for the publication of the article on approval.
Availability of Data and Material
All required data about the manuscript has been already provided. There is no supplemental data.
Competing Interests
The author(s) declare that there are no competing interests in the article.
Authors’ Contributions
Both authors have participated in the conception and design, analysis and interpretation of the data, drafting the article or revising it critically for important intellectual content, and approval of the final version.
References
-
Okeson JP (1996) Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management. European Journal of Orthodontics 19(1): 103-104.
-
Reddy SV, Kumar MP, Sravanthi D, Mohsin AHB, Anuhya V (2014) Bruxism: A Lliterature Review. J Int Oral Health 6(6): 105-109.
-
Goldstein RE, Curtis JW, Farley BA, Siranli S, Clark WA (2018) Abfraction, Abrasion, Attrition and Erosion. Ronald E. Goldstein’s Esthetics in Dentistry, pp: 692-719.
-
Rao SK, Bhat M, David J (2011) Work, Stress and Diurnal Bruxism: A Pilot Study among Information Technology Professionals in Bangalore City, India. International Journal of Dentistry.
-
Rugh JD, Solberg WK (1975) Electromyographic Studies of Bruxist Behavior before and during Treatment. J Calif Dent Assoc 3(9): 56-59.
-
Clark GT, Rugh JD, Handelman SL (1980) Nocturnal Masseter Muscle Activity and Urinary Catecholamine Levels in Bruxers. Journal of Dental Research 59(10): 1571-1576.
-
Rugh JD (1981) Psychological Stress in Orofacial Neuromuscular Problems. International Dental Journal 31(3): 202-205.
-
Rugh JD, Harlan J (1988) Nocturnal Bruxism and Temporomandibular Disorders. Advances in Neurology 49: 329-341.
-
Royeen CB (1985) Adaptation of Likert Scaling for Use with Children. The Occupational Therapy Journal of Research 5(1): 59-69.
-
Scale PS (1983) Perceived Stress Scale.
-
Meyer RA (1990) The Temporomandibular Joint Examination. In: Kenneth W, et al. (Eds.), Clinical Methods: The History, Physical and Laboratory Examinations. 3rd (Edn.), Boston: Butterworths. Chapter 163.
-
Widmalm SE, Lillie JH, Ash MM (1987) Anatomical and Electromyographic Studies of the Lateral Pterygoid Muscle. Journal of Oral Rehabilitation 14(5): 429-446.
-
Miles AE (1962) Assessment of the Ages of a Population of Anglo-Saxons from their Dentitions. Proc R Soc Med 55(10): 881-886.
-
Fluerasu MI, Bocsan IC, Andrei TI, Iacob SM, Popa D (2022) The Epidemiology of Bruxism in Relation to Psychological Factors. International Journal of Environmental Research and Public Health 19(2): 691.
-
Negra JM, Scarpelli AC, Costa D, Guimaraes FH, Pordeus IA (2014) Sleep Bruxism, awake Bruxism and Sleep Quality among Brazilian Dental Students: A Cross- Sectional Study. Brazilian Dental Journal 25(3): 241-247.
-
Molina OF, Santos ZC, Simiao BRH, Marchezan RF, Silva NDPE, et al. (2013) A Comprehensive Method to Classify Subgroups of Bruxers in Temporomandibular Disorders (TMDs) Individuals: Frequency, Clinical and Psychological Implications. Revista Sul-Brasileira de Odontologia 10(1): 11-19.
-
Cavallo P, Carpinelli L, Savarese G (2016) Perceived Stress and Bruxism in University Students. BMC Research Notes 9(1): 514.
-
Nakata A, Takahashi M, Ikeda T, Hojou M, Araki S (2008) Perceived Psychosocial Job Stress and Sleep Bruxism among Male and Female Workers. Community Dentistry and Oral Epidemiology 36(3): 201-209.
-
Muzalev K, Visscher CM, Koutris M, Lobbezoo F (2018) Long‐Term Variability of Sleep Bruxism and Psychological Stress in Patients with Jaw‐Muscle Pain: Report of Two Longitudinal Clinical Cases. Journal of Oral Rehabilitation 45(2): 104-109.
-
Kato T, Thie NM, Huynh N, Miyawaki S, Lavigne GJ (2003) Topical Review: Sleep Bruxism and the Role of Peripheral Sensory Influences. Journal of Orofacial Pain 17(3): 191- 213.
-
Pierce CJ, Chrisman K, Bennett ME, Close JM (1995) Stress, Anticipatory Stress, and Psychologic Measures Related to Sleep Bruxism. Journal of Orofacial Pain 9(1): 51-56.
-
Olkinuora M (1972) Psychosocial Aspects in a Series of Bruxists Compared with a Group of Non-Bruxists. Proceedings of the Finnish Dental Society 68(4): 200- 208.
-
Nagarale R, Todkar M, Shaikh Q, Shaikh S, Shaikh S, et al. (2022) Knowledge, Attitude and Practices Regarding Bruxism and its Management in General Population of Western India: A Questionnaire Study. International Journal of applied Dental Sciences 8(1): 94-98.
-
Seligman DA, Pullinger AG, Solberg WK (1988) The Prevalence of Dental Attrition and its Association with Factors of Age, Gender, Occlusion, and TMJ Symptomatology. Journal of Dental Research 67(10): 1323-1333.
-
Lavigne GJ, Khoury S, Abe S, Yamaguchi T, Raphael K (2008) Bruxism Physiology and Pathology: an Overview for Clinicians. Journal of Oral Rehabilitation 35(7): 476- 494.
-
Montero J, Polo C (2017) Personality Traits and Dental Anxiety in Self-Reported Bruxism: A Cross-Sectional Study. Journal of Dentistry 65: 45-50.
-
Calderon PDS, Kogawa EM, Lauris JRP, Conti PCR (2006) The Influence of Gender and Bruxism on the Human Maximum Bite Force. Journal of Applied Oral Science 14(6): 448-453.
-
Lobbezoo F, Soucy JP, Montplaisir JY, Lavigne GJ (1996) Striatal D2 Receptor Binding in Sleep Bruxism: A Controlled Study with Iodine-123-Iodobenzamide and Single-Photon-Emission Computed Tomography. Journal of Dental Research 75(10): 1804-1810.
-
Sullivan MF, Durham NC (1983) 417 Mich. 398, 338 N.W.2d 181.
-
Albrahim S, Albobali Y, Elzain M (2020) A Challenging Case of Sertraline-Induced Bruxism. Journal of Medical Case Reports And Case Series 1(2).
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells