Archform
The basic principle of arch form in orthodontic treatment is that within reason, the patient’s original arch form should be preserved. These variations in arch form however, are not reflected in the preformed arch wires presently available and it is important to keep in mind during orthodontic treatment that if they are used, their shape should be considered a starting point for the adjustments necessary for proper individualization. Today, however, many normal variations are emphasized more than the specific type of arch forms. Recent studies nullify the existence of a single ideal arch-form template, indicating that dental arch forms are highly individual, and defining a single generalized shape and using variations of it should be avoided.
Abbreviations
CBCT: Cone Beam Computed Tomography; CCD: Charged Couple Device.
Introduction
The basic principle of arch form in orthodontic treatment is that within reason, the patients original arch form should be preserved. Arch form at start is established by the configuration of the bony ridge and then by tooth eruption, perioral muscles, and intraoral functional forces to diminish some of these factors, specialists have explored the most effective approach for the proper repositioning of teeth to provide esthetics, function, and stability, and to define the size and configuration of the dental arch. It is well defined that increase in dental arch length and width during orthodontic treatment tend to return toward preliminary values after retention. This lack of stability of the post treatment dental arches is a difficult problem for the orthodontist. Relapse has long been recognized as being partly due to neglect in maintenance of arch form during orthodontic treatment [1].
Importance of Archform
Arch form is important mainly to obtain proper:
- Esthetics
- Function
- Stability
Esthetics
Esthetics is the driving force for the patient to seek orthodontic treatment. It is one thing, which attracts patients for the treatment. The teeth are arranged in proper arch form, for esthetic smile will no doubt improve the value.
Function
Function cannot be obtained until the teeth occlude properly. Proper occlusion can only be possible when both upper and lower teeth are aligned.
Stability
Stability of arch form is one of the most desirable but least understood goals of orthodontic treatment. The arch form obtained after alignment of teeth should be placed such that equilibrium is not affected In today’s culture a “broader smile” achieved through expansion of the dental arches is in direct conflict with the fact that expansion of the lower inter-canine width has an adverse effect on stability. Therefore, if stability is of utmost importance treatment should be directed towards maintaining the arch form presented by the malocclusion as much as possible. The resolution of the conflict between desired esthetic change and stability ultimately depends on the decision made by the orthodontist with the patient.
Stability of the arch form changes with greater relative stability of premolar than canine expansion. The greater the arch form change, the greater the risk post retention changes. The patient’s pre-treatment arch form appeared to be the best guide to future arch form stability. Patients should be appraised of treatment limitations before treatment in terms of stability. Meta-analysis on maxillary expansion tells that stability is very less. Most of the expansion lasts during post retention period. Stability is more in maxillary arch in comparison with mandibular arch.
MBT Archform
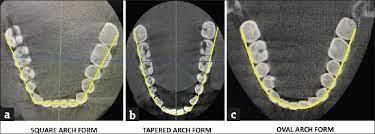
Mclaughlin RP, et al. [2] have classified arch forms as tapered, square and ovoid when enveloped, the three Arch forms mainly in inter-canine and inter-first premolar width, giving a range of approximately 6 mm in this area [3].
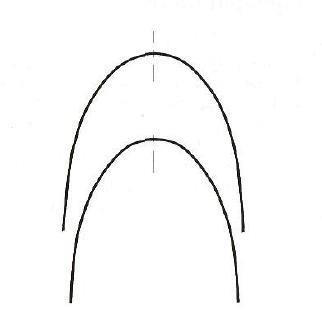
Tapered Archform
This arch form has the smallest inter-canine width and is useful in patients with narrow, tapered arch forms. It is particularly to use this form for patients with narrow arches, and especially in cases with gingival recession in the canine and premolar regions (mostly seen in adult cases). Cases undergoing single arch treatment often require the use of the tapered arch form. In this way, no expansion of the treated arch occurs, relative to e untreated arch. The posterior part of this arch form can easily be modified to the match the inter- molar width of the patient (Figure 1).
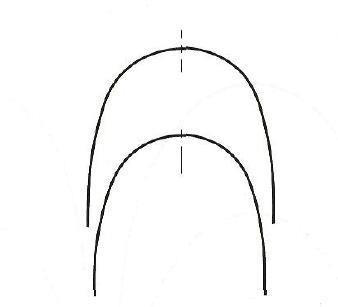
Square Archform
This arch form has the broadest inter-canine width and seen in patients with broad arch forms. It is also helpful, at least in the first part of treatment, for cases that require buccal uprighting of the lower posterior segments and expansion of the upper arch. The square arch form is useful to era overexpansion has been achieved, it may be beneficial to change to the ovoid after maintain expansion in upper arches after rapid maxillary expansion (Figure 2).
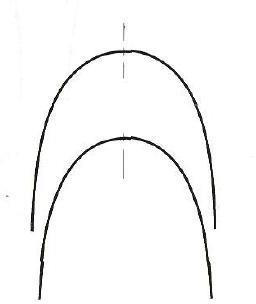
Ovoid Archform
Advisable to stock wires in ovoid arch form (Figure 3) wires, which then can be changed depending on the case. The combined uses of this arch form with appropriate finishing, settling, and retention procedures has resulted in a majority of cases with good stability, and minimal amounts of post-treatment relapse. The square arch form is used for maintenance of expansion in upper-arch after rapid expansion [2].
Recent Developments
The era of 3D radiographic imaging with Cone Beam Computed Tomography (CBCT) has led to aggregation of clinical application across all dental disciplines. Frontal views of dental arches aid in the assessment of vertical and transverse dimensions to evaluate inter arch discrepancies (Figure 4).
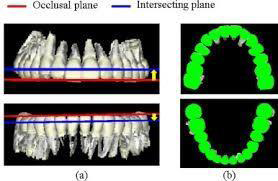
Occlusal views of arches reveal relative tooth positions and shape of alveolar bone support. Arch form tracings are made at the height of the alveolus. The arch forms can then be posed to reveal the similarities (Figure 5).
Arch Form in Lingual Orthodontics
Due to the lingual morphology of the teeth, a straight wire cannot be engaged lingually. The arch form is altered accordingly. The wires used here are “Mushroom Shaped”, with an offset present between canine and premolar. The arch forms are derived from the skeletal and dental anatomy and are therefore designed to be closer to an anatomic ideal than a mathematical ideal. Previous arch wire shapes had their in the concept of an ideal arch form; anatomy probably was not given enough consideration in design [4].
Laser P Mapping
Another interesting concept being developed by Syrinx Technologies, Texas (1976) is to place brackets on teeth, followed by laser mapping to establish the arch form. and transfer those 3 dimensional data to a computer for storage and usage. After the clinician decides the direction the teeth are to go on “arch wire bending robot” can fabricate an individually designed arch wire to achieve the desired movements [5].
Wire Bending Robots
If the effort to fabricate a complex archwire were eliminated, “plain vanilla” brackets without all the straight wire compensations could be used instead of going to the trouble of producing custom brackets with elaborate prescriptions.
In lingual orthodontics, the laser-scanned casts needed for fabrication of custom bracket pads also can provide the data needed to generate computer-fabricated archwires. For labial archwires the data can be accomplished via an intraoral scan that is done using a charged couple device (CCD) video camera connected to a projector [6].
Variation in Arch Form
Over the years the great majority of authors on the subject of arch form have recognized that there is variability in the size and shape of human arch form.
Racial Differences in Arch Form
- Mary lynnmerz (1991), the dental arches of the black patients as compared to whites was significantly wider and deeper with significantly larger mesio-distal diameters of the canine, premolar and molar [7].
- Prasad K, et al. [8] was evaluated whether pont’s index could be used on Indians and Chinese and to establish the norms. They found that there was highly significant difference between two sample groups regarding pre molar and molar arch widths. Significant correlation was found existing between combined maxillary incisor widths and premolar and molar widths in both samples [8].
- The Caucasian population had a significant decreased arch width and increased arch depth compared with the Japanese population [9].
Gender Differences in Arch Form
- Did a study to compare the dental arch dimensions between dentoalveolar classes I, II & III, and between male and female subjects as measured on virtual 3D models.
- In men, a statistically significant difference in upper dental arch was found only in the incisor region and in the lower dental arch, differences were found in intercanine and intermolar region.
- Noticeable differences were seen between the male groups in upper molar depth dimension and in lower molar and canine depth dimension. The class I group had the largest upper and lower dental arches and the class III group the shortest. Similarly noticeable variation was found in lower molar width/depth ratio, lower canine width/depth ratio, and lower canine depth/ molar depth ratio [10].
Arch Form Differences Based on Facial Type
Kageyama T, et al. [11] in their study to evaluate dental arch forms associated with various facial types in adolescence with class II div. 1 malocclusion came to the conclusion that dental arch depth of the brachyfacial subjects was significantly greater than that of the mesofacial subjects in the maxillary arch [11].
Even Williams PM [12] recommended that the shape of the head and the face should be considered in order to determine the shape of dental arch. Grabber describes dolichocephalic individuals have long, narrow face and relatively narrow dental arches. Brachycephalic facial type individuals have very broad and relatively short faces and broad round dental arches. Mesocephalic individuals fit somewhere in between these two [12].
Narrow arch forms with V shaped arches and vaulted palates result in many of the intra oral occlusal signs of wear, facets, crowding of teeth, lingual inclination of lower teeth, teeth chipping and cusp breakage with accompanying dry mouth syndrome and a asymmetric faces. These problems if unrecognized and untreated will lead to unstable bites and lack of long term retention after orthodontic therapy. Thus orthodontic or orthopaedic concepts are changing with the dental profession due to numerous clinical results and long term treatment outcomes that many general orthodontic practitioners and orthodontic specialist are experiencing in their clinical care.
Conclusion
The search for a universal ideal arch form has been one of the most persistent but elusive tasks that orthodontic researchers have pursued. Current literature illustrates many divergent views on the shape of arch form it is now generally believed that the arch shape is determined by an interplay between genetic and many varied environmental factors such as pressure from soft tissues; shape and position of jaws; alteration in eruptive mechanism and morphology of teeth.
The basic principle of arch form in orthodontic treatment is that within reason, the patients original arch from should be preserved. These variations in arch form, however, are not reflected in the preformed arch wires presently available and it is important to keep in mind during orthodontic treatment that if they are used, their shape should be considered a starting point for the adjustments necessary for proper individualization Clinicians should therefore be cautious when treating Individuals to a mathematically derived ideal.
The common consensus though seems to be that individualization and coordination of arch forms for each patient is a must to obtain optimum long term stability. A study of any aspect of orthodontics immediately involves the problem of variation in the size of structure variation in the form of parts and variation in function and dental arch from is no exception to this. The form and size of dental arches is Influence by at least 4 factors. Firstly, skeletal parts may not be harmonious or in proportion and this will mean appropriate compromises are indicated from otherwise ideal relations. Secondly, functional problems may alter the oral environment when muscle structure itself may be Inadequate Thirdly psychologic factors may be present causing prolonged habits and fourthly, discrepancies in tooth size and tooth form may alter an otherwise harmonious situation. Because of these complex problems and relatively low knowledge of dental arches as of today. There is no universally accepted ideal arch form. The irony of wisdom is that the more we know about a particular subject, the more our ignorance unfolds and the goal seems far ahead.
Hence, we know that presently there is no generalized, universal, ideal arch form and It is great challenge for an orthodontist to treat the patient we should follow what Dr. Angle suggested nearly a century ago, and which still holds true, that is, “The best the orthodontist can do is to secure normal relations of the teeth and correct general form of arch leaving the finer adjustments to individual type and form to be worked out by Nature through her forces, which must in any event, finally triumph”.
References
-
Singh D (2021) Arch form: A Review. International Journal of Health Sciences 5(S1): 358-367.
-
Mclaughlin RP, Bennett JC, Trevisi HJ (2001) Systemized Orthodontic Treatment Mechanics. Mosby, Edinburgh.
-
Mclaughlin (1997) MBT™M Arch form and Archwire Sequencing. The MBT Versatile+Appliance system.
-
Andreiko C (1994) The Elan and Orthos Systems. J Clin Orthod 28(8): 459-468.
-
Ronay V, Miner RM, Will LA, Arai K (2008) Mandibular Arch form: The Relationship between Dental and Basal Anatomy. Am J Orthod Dentofacial Orthop 134(3): 430- 438.
-
Jiang J, Ma X, Zhang Y, Huo B, Liu Y (2018) Study on Three- Dimensional Digital Expression and Robot Bending Method of Orthodontic Archwire. Appl Bionics Biomech.
-
Merz ML, Isaacson RJ, Germane N, Rubenstein LK (1991) Tooth Diameters and Arch Perimeters in a Black and a White Population. Am J Orthod Dentofacial Orthop 100(1): 53-58.
-
Prasad K (1995) Model Analysis- Comparison of Norms for Indians and Chinese using Pont’s Index. J Ind Orthod So 26(1): 1-5.
-
Nojima K, McLaughlin RP, Isshiki Y, Sinclair PM (2001) A Comparative Study of Caucasians and Japanese Mandibular Clinical Arch Forms. Angle Orthod 71(3): 195-200.
-
Slaj M, Spalj S, Pavlin D, Illes D, Slaj M (2010) Dental Archforms in Dentoalveolar Class I, II, III. Angle Orthod 80(5): 919-924.
-
Kageyama T, Rodriguez GC, Vigorito JW, Deguchi T (2006) A Morphological Study of the Relationship between Arch Dimensions and Craniofacial Structures in Adolescents with Class II Division I Malocclusions and Various Facial Types. Am J Orthod Dentofacial Orthop 129(3): 368-375.
-
Williams PM (1917) Determining the Shape of the Normal Arch. Dent cosmos 59: 695-708.
- Diagnosis and Management of Mental Nerve Paresthesia Secondary to Apical Periodontitis of Mandibular Second Premolar: A CBCT Based Case Report
- A Randomized, Double Blinded Clinical Trial to Compare the Effect of Oral Premedication (Diclofenac Potassium or Dexamethasone) on Post-Operative Pain Following Pulpectomy
- Modified Lip Repositioning Technique for the Management of Excessive Gingival Display
- Integral Role of Non-Dental Providers and Fluoride Dissemination
- Root Canal Treatment Rate in Deciduous Teeth Among 6-Year- Olds in the Era of Discontinuing Water Fluoridation - Historical Cohort Study
- The Impact of the Notch1 on the Migratory Capacity and the Expression of E-Cadherin and CyclinD1 in Ameloblastoma Cells