Diabetic Pain
Editorial
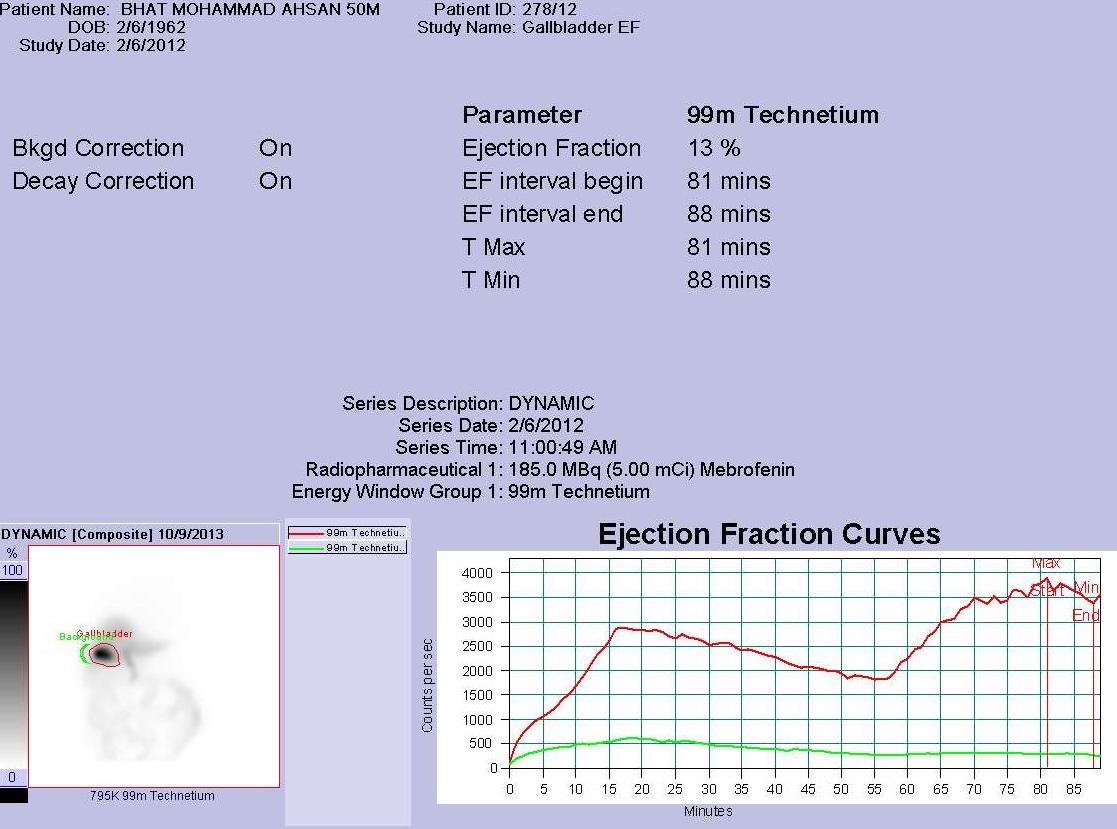
The common form of diabetes mellitus, type 2 diabetes mellitus, is projected to affect an estimated 366 million people worldwide by 2030 [1]. Involvement of the peripheral and autonomic nervous systems is the most common complication of diabetes. Incidence of neuropathy being approximately 45% for patients with type 2 diabetes mellitus and 54% to 59% for patients with type 1 diabetes mellitus. Nerve conduction tests performed at the time of diagnosis demonstrate that neuropathy is already present in patients when it is still subclinical, and these tests show improvement with intensive control of glycemia. Significant peripheral neuropathic pain occurs in 7.5% to 24% of all patients with diabetes mellitus [2]. Peripheral neuropathic pain is also one of the most common presentations in impaired glucose tolerance and impaired fasting glucose compared to autonomic pain. The symptoms of diabetic autonomic neuropathy depend on which specific component of the autonomic nervous system is affected. These include cardiac autonomic system, peripheral autonomic dysfunction, genitourinary autonomic neuropathy and last but not the least and most troublesome neuropathy, the gastrointestinal autonomic neuropathy which often goes unrecognised being attributed to drug or other cause. It is important to recognise this pain as it has an impact on morbidity and mortality in people with diabetes. Studies assessing the prevalence of gastrointestinal symptoms in patients with diabetes mellitus have shown that people with diabetes are more likely to experience gastrointestinal symptoms compared with controls [3, 4, 5]. These patients can present with esophageal motility disorders like dysphagia, retrosternal pain and heartburn [6]. This has been attributed to reduced amplitude and decreased wave speed of the tubular esophageal contractions in people with diabetes and gastrointestinal neuropathy [7, 8]. Patients with delayed gastric emptying may be asymptomatic [9] or present with anorexia, nausea, vomiting, early satiety, and postprandial fullness. Diabetic enteropathy reflects widespread gastrointestinal autonomic neuropathy. Less is known about gall bladder emptying in people with diabetes which can be delayed due to uncontrolled hyperglycemia [10] and can be symptomatic in form of severe pain in epigastric region associated with nausea and vomiting simulating pain in cholelithiasis or gastritis. Some of patients in our previous study [10] developed severe intractable pain in epigastrium without a definite cause after full evaluation. Measuring gall bladder ejection fraction can be helpful in symptomatic patients with diabetes. Two of our symptomatic patients with diabetes were also noted to have reduced gall bladder ejection fraction 13 % (also known as dyskinesia) as shown in the graph (figure 1). These patients were subjected to cholescystectomy for relief of severe refractory pain and had a significant relief as shown by studies that gall bladder dyskinesia can predict the success of cholecystectomy in symptomatic patients [11]. Exact mechanism of gall bladder dyskinesia in people with diabetes is not known. Acalculous cholecystitis or diabetic cholecystoparesis has been proposed as the probable etiology. Thus diabetic autonomic neuropathy secondary to chronic hyperglycemia as well as acute hyperglycemia affects motor function of biliary system which can cause refractory pain and should always be considered while evaluating the patient for same so that management can be given at appropriate time.
References
-
Wild S, Roglic G, Green A, Sicree R, King H (2004) Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27(5): 1047-1053.
-
Zilliox L, Russell JW (2011) Treatment of diabetic sensory polyneuropathy. Curr Treat Options Neurol 13(2): 143-159.
-
Spångéus A, El-Salhy M, Suhr O, Eriksson J, Lithner F (1999) Prevalence of gastrointestinal symptoms in young and middle-aged diabetic patients. Scand J Gastroenterol 34(12): 1196-202.
-
Ricci JA, Siddique R, Stewart WF, Sandler RS, Sloan S, et al. (2000) Upper gastrointestinal symptoms in a U.S. national sample of adults with diabetes. Scand J Gastroenterol 35(2): 152-159.
-
Ko GT, Chan WB, Chan JC, Tsang LW, Cockram CS (1999) Gastrointestinal symptoms in Chinese patients with Type 2 diabetes mellitus. Diabet Med 16(8): 670- 674.
-
Rayner CK, Samsom M, Jones KL, Horowitz M (2001) Relationships of upper gastrointestinal motor and sensory function with glycemic control. Diabetes Care 24(2): 371-381.
-
Stewart IM, Hosking DJ, Preston BJ, Atkinson M (1976) Oesophageal motor changes in diabetes mellitus. Thorax 31(3): 278-281.
-
Hollis JB, Castell DO, Braddom RL (1977) Esophageal function in diabetes mellitus and its relation to peripheral neuropathy. Gastroenterology 73(5): 1098-1102.
-
Laway BA, Malik TS, Khan SH, Rather TA (2013) Prevalence of abnormal gastric emptying in symptomatic women with newly detected diabetes and its reversibility after glycemic control-a prospective case control study. J Diabetes Complications 27(1): 78-81.
-
Arshad F, Laway BA, Rather TA, Kuchay MS, Khan SH (2015) Impaired Gallbladder Motility in Adults with Newly Detected Type 2 -Diabetes and Lack of Reversibility after Achieving Euglycemia. Can J Diabetes 39(2): 101-104.
-
Sorenson MK, Fancher S, Lang NP, Eidt JF, Broadwater JR (1993) Abnormal gallbladder nuclear ejection fraction predicts success of cholecystectomy in patients with biliary dyskinesia. Am J Surg 166(6): 672-674.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty