Agranulocytosis: A Rare Complication and Management Paradox
<p>Introduction: Thyroid disorders are common disorders seen around the globe. The prevalence of thyroid disorders in India is approximately 5-10%, more common in females and hypothyroidism being more common than hypothyroidism followed by hyperthyroidism. Anti-thyroid drugs are commonly used for the medical management of hyperthyroidism. A rare and notoriously dangerous complication of these drugs is agranulocytosis, seen in 0.3-0.5% of treated patients. Case: A 50 year old female presented in the emergency department with high grade fever associated with rigors and severe throat paint associated with difficult and painful swallowing since 5 days. She was a known case of hyperthyroidism on carbimazole 30 mg once daily since 1 year. Patient was vitally stable and throat examination showed severely enlarged and inflamed tonsils with inflamed posterior pharyngeal. ENT opinion was taken which advised for conservative management and elective tonsillectomy later. The entire fever profile was negative. Her total leucocyte count was 650 cells/mm3. Carbimazole induced agranulocytosis was suspected and the drug was withheld. Gradually the WBC count started to rise and patient recovered symptomatically. Conclusion: Agranulocytosis is a potentially lethal side effect but if diagnosed early is treatable. High index of suspicion and timely drug withdrawal is the key to reduce morbidity and mortality.</p>
Introduction
Thyroid diseases are one of the most common endocrine disorder worldwide having higher prevalence in females [1]. As shown in several epidemiological studies the prevalence of hyperthyroidism was either subclinical or overt hyperthyroidism and was present in 1.6% and 1.3% of the population [2]. Thionamide group of drugs were discovered way back in 1943 to treat hyperthyroidism which inhibits thyroid hormone synthesis. They are actively transported into the thyroid gland by Na+ - I- symporter, where they inhibit both the organification of iodine to tyrosine residues in thyroglobulin and the coupling of iodothyronines [3]. Propylthiouracil, carbimazole and methimazole are the thionamide drugs available and commonly used. These drugs act like a double edged sword as they treat hyperthyroidism a life threatening condition and may increase mortality and morbidity with its dangerous side effects like agranulocytosis. Hereby we report a case of 50 year old female who presented in neutropenic sepsis probably secondary to carbimazole induced agranulocytosis.
Case Report
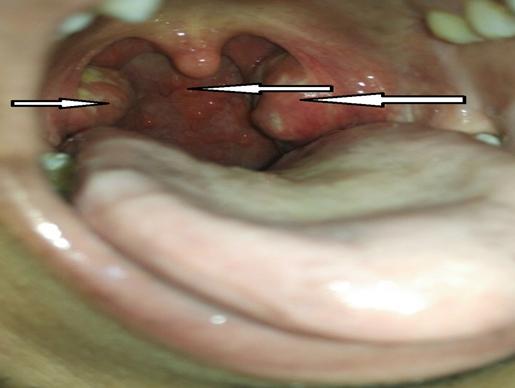
A 50 year old female a known case of hyperthyroidism on tablet carbimazole 30mg once daily since 1 year, presented in the emergency room with complaints of high grade fever with rigors, severe throat pain, painful swallowing and lose stools since 5 days. She had no other comorbidities. On examination of the throat she had bilaterally enlarged and inflamed tonsils, with congested posterior pharyngeal wall (Figure 1). Systemic examination was unremarkable with Watofsky score of 20. All routine blood investigations were sent including blood and throat swab cultures and are described in Table 1 and Table 2.
| Investigation | Report | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Heamoglobin | 12.1 g/dl | |||||||||||||||||||||
| PLATELETS | 1.45 | |||||||||||||||||||||
| Erythrocyte Sedimentation Rate | 108 | |||||||||||||||||||||
| Malaria Parasite | NEGATIVE | |||||||||||||||||||||
| DENGUE | NEGATIVE | |||||||||||||||||||||
| T3 | 95.4 g/ml | |||||||||||||||||||||
| T4 | 8.4 µg/ml | |||||||||||||||||||||
| TSH | < 0.01 µIU/ml |
Table 1: Base Line investigations.
| Investigation | Report | ||||
|---|---|---|---|---|---|
| Peripheral smear | Severe leucopoenia with marked neutropenia, reactive lymphocytosis and relative eosinophilia. | ||||
| Throat swab culture and sensitivity | Gram stain: few pus cells, few gram negative & gram negative bacilli seen. Organism: Klebsiella pneumoniae. | ||||
| USG neck | Few enlarged lymph nodes bilaterally in levels 2, 3, 4, largest measuring 1.4 cm. Right lobe of thyroid showed a cyst measuring 3mm normal in vascularity. |
Table 2: Special Investigations.
Treatment and Outcome
Patient was isolated and reverse barrier nursing was initiated. Carbimazole was withheld immediately. Patient was started empirically on injectable cefoperazone and sulbactum 1.5 gm twice daily, injection metronidazole 500 mg thrice daily. Paracetamol was given for fever spikes and chlorhexidine mouthwash for oral congestion. On symptomatic treatment patient WBC’s showed increasing trend as described in Table 3 and patient got relieved symptomatically. Then patient was advised radio iodine ablation and was discharged only beta blockers.
| WBC Count | Day 1 | Day 3 | Day 7 |
|---|---|---|---|
| 650 | 2610 | 6150 |
Table 3: White Blood Cells (WBCs) Increasing Trend.
Discussion
Carbimazole, a prodrug which gets converted into the active form methimazole. It is used alone or in combination with other medications for the treatment of hyperthyroidism. This therapy usually started with two to three divided doses in total of 30–60 mg/day but the maximum daily dose should not exceed 120mg. usually within 4–8 weeks of starting therapy, symptoms will diminish and circulating thyroid hormone levels will return to normal. Typical range of daily maintenance dose in adults is 5–30 mg/day. The serum half-life of carbimazole is five to six hours but have prolonged half- life intra thyroid. Thionamides like methimazole, carbimazole and propyl thiouracil may cause minor side effects like pruritus, rash, urticaria, arthralgia, arthritis, fever, abnormal taste sensation, nausea, or vomiting in up to 13 percent of patients [4]. But some of the serious side effects are agranulocytosis and hepatotoxicity. The incidence of carbimazole induced agranulocytosis is 0.3– 0.6% [5] and has got a mortality rate of 21.5% [6]. In 1983, a study conducted by Cooper et al. concluded that methimazole in higher doses of 30 mg/day and age of 40 years or above caused greater risk for the development of agranulocytosis [7]. Drug-induced agranulocytosis usually occurs within 1–2 months of taking the anti-thyroid medication but the onset in some cases may get delayed, like in our case patient developed agranulocytosis after being on carbimazole for one year. Over a period of 1–2 weeks, the WBC count usually returns to normal after discontinuing the offending drug and the time taken can be estimated between days to months [8, 9]. The mechanism behind agranulocytosis is considered to be immune mediated destruction of granulocytes and idiosyncratic drug reactions. Successful treatment of anti- thyroid drug-induced agranulocytosis by GCSF (granulocyte colony-stimulating factor) has been reported [10]. It enhances the recovery of the peripheral blood granulocyte lineage which results in the faster normalization of peripheral granulocyte count as well as reduction in chances of fatal complications like bacterial infections [11].
Conclusion
Thionamides are used to treat hyperthyroidism and hyperthyroid patients started on anti-thyroid medications, should be warned about the dangerous side effects, not only on initiation of the medication but on every follow up visit as well. Patients taking anti thyroid medications presenting with high grade fever with neck discomfort, agranulocytosis should be suspected and timely investigations are required to confirm. Here the treatment has paradox in form of withholding medications instead of prescribing medications with symptomatic support.
References
-
Davis TF, Laurberg P, Bahn RS (2016) Hyperthyroid. Melmed S, Polonsky KS, Larsen PR, Kronberg HM (Eds.), Disorders in Williams Textbook of Endocrinology. 13th (Edn.), Elsevier, pp: 369-415.
-
Usha Menon V, Sundaram KR, Unnikrishnan AG, Jayakumar RV, Nair V (2009) High prevalence of undetected thyroid disorders in an iodine sufficient adult south Indian population. J Indian Med Assoc 107(2): 72-77.
-
Cooper DS (2005) Antithyroid drugs. N Engl J Med 352(9): 905-917.
-
Sundaresh V, Brito JP, Wang Z, Prokop LJ, Stan MN, et al. (2013) Comparative effectiveness of therapies for Graves' hyperthyroidism: a systematic review and network meta-analysis. J Clin Endocrinol Metab 98(9): 3671-3677.
-
Genet P, Pulik M, Lionnet F, Bremont C (1994) Use of colony stimulating factors for the treatment of carbimazole-induced agranulocytosis. Am J Hematol 47(4): 334-335.
-
Juliá A, Olona M, Bueno J, Revilla E, Rosselló J, et al. (1991) Drug-induced agranulocytosis: Prognostic factors in a series of 168 episodes. Br J Haematol 79(3): 366-372.
-
Cooper DS, Goldminz D, Levin AA, Ladenson PW, Daniels GH, et al. (1983) Agranulocytosis associated with antithyroid drugs. Effects of patient age and drug dose. Ann Intern Med 98(1): 26-29.
-
Tavintharan S, Rajasoorya C, Chew LS (1997) Carbimazole-induced agranulocytosis-a report of 2 recent cases. Singapore Med J 38(9): 386-387.
-
Ng SC (1995) Carbimazole-induced agranulocytosis treated with granulocyte-macrophage colony stimulating factor-a case report. Ann Acad Med Singapore 24(3): 465-466.
-
Gerl A, Gerhartz H, Wilmanns W (1991) GM-CSF for agranulocytosis. J Intern Med 230(1): 90-91. Sheng WH, Hung CC, Chen YC, Fang CT, Hsieh SM, et al. (1999) Antithyroid-drug-induced agranulocytosis complicated by life-threatening infections. QJM 92(8): 455-461.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty