Thyroid Cancer in Patients with Rheumatic Diseases
Summary: A close bidirectional relationship coexists in patients with malignancies diseases and rheumatic diseases (RD). The autoimmune thyroid disease and RD go beyond the multifactorial causes of malignant development. Different autoimmune elements produced by thyroid cancer are detected in SEL and RA patients. Autoantibodies against the thyroid gland are also detected in patients with RD. The objectives of this study are to know the clinical behavior of both entities and to describe the clinical characteristics of the patients with rheumatic diseases and thyroid cancer concurrent. Methods: This is a descriptive study with a serie of cases and reviews of literature. The records of patients with diagnosis of thyroid cancer and rheumatic disease according to American Rheumatology Collage were reviewed during the study period. The risk factor, clinical characteristics of the patients and histological subtype of thyroid cancer were classified according to world health organizations (WHO) using AGES-stage system. The thyroid cancer staging was done according to the American Joint Committee on Cancer (AJCC) and therapeutic approached. The univariable review was realized with frequency and percentage using excel program 2010. The laboratory test was processed using operative laboratory system ClinSis 2015. Results: The records of 250 patients with thyroid cancer diagnosed, 5 with rheumatic diseases, represent 2%. Female 4 (80%) 1 man (20%). 3 Systemic Erythematous Lupus (SEL) (60%) and 2 Rheumatoid arthritis (RA) (40%) 1 patient with both. The age range was 22-48 years old, the average age was 33 years old. Serologic test to SEL reveled: Antinuclear antibodies (ANAiFi) positive in all cases and the patients with RA: Rheumatic Factor positive 100%. SEL patients presented hematologic and cardiovascular symptoms in all cases and one case with chronic failure kidney, with successful kidney transplant during two years and then required hemodialysis. The echocardiogram reported pulmonary hypertension, mitral and tricuspid valves insufficiency and 1 patient with severe tricuspid valves insufficiency plus right heart dilatation. One case with left hip severe osteoarthritis that required hip replacement. There was another patient with incidental finding: pleural effusion, ascitis and hepatomegaly. The patient with both disease died by severe pulmonary hypertension. Rheumatoid arthritis was diagnosed in 2 patients (40%) 1 man and 1 female. 1 patient with symmetric polyarthritis, morning stiffness and joint limitation, affecting elbow and carpus. The other presented polyarthritis compromising both hands and cervical spine, who developed left lower limb edema with Doppler report of proximal pseudoaneurysm. The classic papillary carcinoma was diagnosed in the majority of cases, and it was classified as low risk in patients with SEL and patients with intermediate risk were RA patients. The thyroid cancer staging was: staging I corresponded to SEL and staging IV corresponded to RA. The surgical approach was two patients with total thyroidectomy and one with right lobectomy in SEL. Two total thyroidectomy plus modified radical neck dissection corresponded to RA patients due to extra capsular extension and nodal positive. These used radio ablation with Iodo. Conclusion: The rheumatic diseases (SEL and RA) concurrent in patients with thyroid cancer, were presented in the minority of cases in our little serie. The young woman was the most affected. Most of the cases presented hematologic symptoms and a severe case with Rhupus syndrome that die for pulmonary complication. The patients with classic papillary thyroid cancer in early stage (low risk) were treated with total thyroidectomy plus radio iodine ablation in the majority of the cases without complications. Our result is similar as the international literature.
Introduction
Several chapters have been written about cancer with autoimmunity and show a bidirectional relationship. Patients with malignancies diseases may develop rheumatic manifestation [1]. Autoantibodie activity has been identified in patients with solid tumors and hematological malignancies also anty-oncoprotein antibodies, anti-tumor suppressor genes, antiproliferation associated antigens, to name a few [2, 3, 4]. Antinuclear antibodies are detected in patients with cancer (Anti-DNA, Anti- phospholipid autoantibodies), 2-12% of these patients have lupus anticoagulation activity. These autoantibodies are called Natural autoantibodies [5, 6].
The activation of autoimmune mechanisms among patients with cancer may be associated with development of rheumatic diseases (RD). On the other hand, several studies in patients with RD has demonstrated the increased risk to develop cancer, compared with general population [7, 8]. Various RD have strong association with benign thyroid disorders (Hashimoto’s and Grave diseases, thyroid acropacy) due to influence of several risk factor: genetic and environment, iodine intake, chronic infection diseases, that at the end, develop a really autoimmune systemic reaction [9]. The objectives ares to know the clinical behavior of both entity and to describe the clinical characteristics of the patients with rheumatic diseases and thyroid cancer concurrent.
Methods
This is a descriptive study with a serie of cases and reviews of literature. The records of patients with diagnosis of thyroid cancer and rheumatic disease according to American Rheumatology Collage were reviewed during the study period [10]. The risk factor, clinical characteristics of the patients and histological subtype of thyroid cancer were classified according to world health organizations (WHO) and AGES-stage system [11, 12]. The thyroid cancer staging was done according to the American Joint Committee on Cancer (AJCC) and therapeutic approached [13]. The univariable review was realized with frequency and percentage using excel program 2010. The laboratory test was processed using operative laboratory system ClinSis 2015.
Results
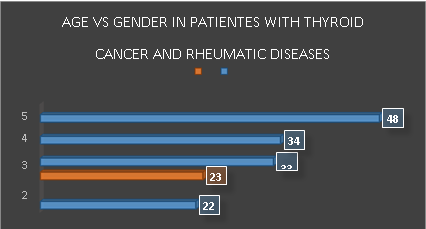
The file a record of 250 patients with thyroid cancer diagnosed was reviewed, 5 patients with rheumatic diseases, represent 2%, female 4 (80%) 1 man (20%). The age range was 22-48 years old, the average age was 33 years old (Figure 1).
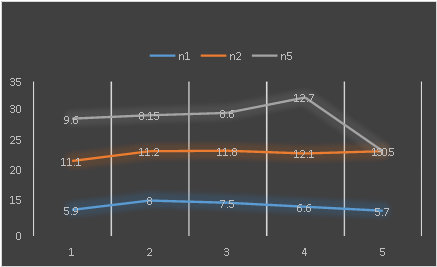
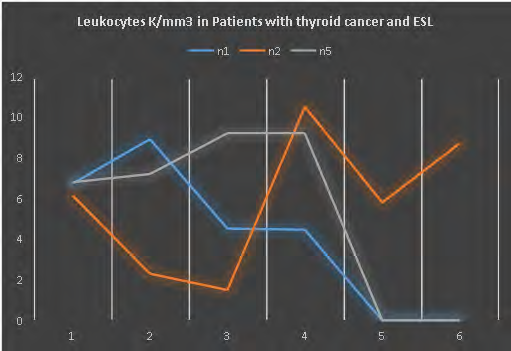
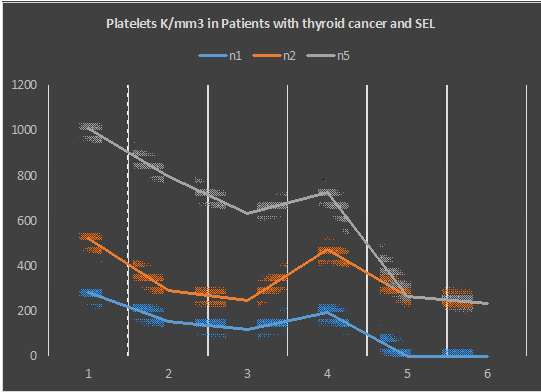
The rheumatic diseases diagnosed were 3 Systemic Erythematous Lupus (SEL) (60%) and 2 Rheumatoid arthritis (RA) (40%) 1 patient with both diseases. The clinical presentation to SEL, were hematologic symptoms the
3 patients (Figures 2-4), 1 patient with high blood pressure, chronic failure kidney and hemodialysis therapy for 2 years, she had successful kidney transplant for two years and then required hemodialysis therapy.
Serologic test to SEL reveled: Antinuclear antibodies (ANA-iFi) positive in 3 cases (100%), Anti-Cal antibodies positive 1 Patient (33.3%), Rheumatoid factor positive 1 patient that presented both diseases. 2 patients (66%) the echocardiogram reported pulmonary hypertension (33mmHg/ 50mmHg), mitral and tricuspid valves insufficiency 1 patient (33.3%) and 1 patient with severe tricuspid valves insufficiency plus right heart dilatation. Only 1 patient with normal echocardiogram.
Imagine finding TC reported left hip severe osteoarthritis, required hip replacements, the patients with both diseases; 1 patient with 10th costal fractured as incidental finding plus pleural effusion, ascites and hepatomegaly. The 3 patients (100%) were treated with Plaquinol and 1 case with Metrotexate. The patient with both disease died by severe pulmonary hypertension. Rheumatoid arthritis was diagnosed 2 patients (40%), 1 man and 1 female, 1 patient with symmetric polyarthritis , morning stiffness and joint limitation, affecting elbow and carpus; the other presented polyarthritis compromise both hands and cervical spine, after developed left lower limb edema with Doppler report of proximal pseudoaneurysm.
Serologic test to RA were Rheumatic Factor positive 2 patients, (100%), Citrullinated cyclic peptide antibodies and PC Reactive positive 1 patient. 1 patient developed left sub deltoid bursitis diagnosed by ultrasound. The hematologic test was normal in both patients. Both were treated with Plaquinol and Metrotexate. The Papillary carcinoma classic was diagnosed in 4 patients (80%), 1 patients (20%) with Follicular variant of Papillary carcinoma corresponded to the man patient. The risk factor classification using AGES stage system was: 3 patients diagnosed with SEL were low risk (60%) and 2 patients with intermediate risk were RA patients (40%).
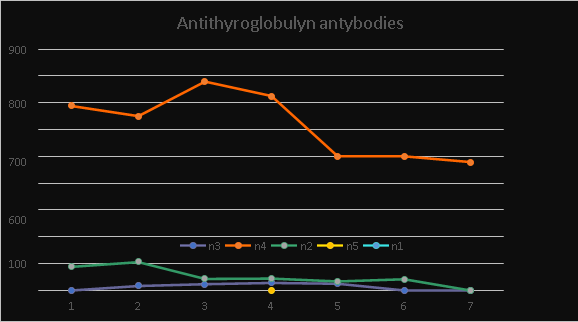
The thyroid cancer staging was: 3 patients with clinical staging I corresponded to SEL (60%) and 2 patients with clinical staging IV corresponded to RA (40%). The right lobe was affected in 4 patients (80%) and 1 in the left lobe of the thyroid (20%). The surgical approached was 2 patients with Total thyroidectomy and 1 with right lobectomy in SEL. 2 Total thyroidectomy plus modified radical neck dissection corresponded to RA patients (40%). Surgical pathologic reported: 2 Papillary microcarcinoma less than 10mm and 1 measured 15mm, 1 Hashimoto Thyroiditis concomitants with cancer and 1 multifocally carcinoma. 1 papillary microcarcinoma and 1 measured less than 20mm in RA patients. 2 extra thyroid extensions were reported: extra capsular extension and neck nodal positive in patients with RA. 4 patients used Radio ablation iodine (RAI) therapy (80%), 2 ESL and 2 RA patients. The report of Antithyroglobulyn antibodies range was 15, 9-778, 5. 1 patient with RA with high level prior and post-surgery. Without evidence of disease post-surgery, the rest were normal (Figure 5).
Discussion
The thyroid cancer is the most common between the endocrine tumors. Nowadays the diagnosed in early stage is due to use of high technology ultrasound in the clinical practice. Those have been reflected in several researches with an increase incidence in the last decade [14, 15, 16]. The coexistence among malignant neoplasm and autoimmune disease (AID) has been demonstrated; a particular group is the Systemic Erythematous Lupus (SEL) patients, the range of 0.4-3.4% the thyroid cancer was found in this people group as our results [17]. The autoimmune thyroid disease (ATD)
as Hashimoto’s thyroiditis (HT)or Graves Basedow disease could be a clinical manifestation of AID (ESL or Rheumatic Arthritis) [9, 18].
One of our patients treated by papillary thyroid cancer (PTC) development LES two years later; we reviewed the first Fine Needle aspiration (FNA) the report was Hashimoto Thyroiditis and follow up a new FNA reported the thyroid cancer. This topic was described by Biro same as our patient. The period of time of duration of diagnosed of SEL when cancer, the range was 2-30 years [19]. The 62% of patients with ATD have someone RD. The 51 % of patients with SEL have antibodies anti thyroid compared with control (p:<0.05) [20, 21, 22, 23]. The first proposed about the relationship among AID and malignancies neoplasm was by Virchow and after several papers published different aspect about this topic [24, 25, 26, 27]. The relationship among gender and age, have been established in both entities, ours results are similar as international literature. It is currently know that increasing age and female gender are associated with increasing risk of developing autoimmune disorders [28, 29]. The close relationship of ATD and RD go too far in the heterogeneity to development malignant neoplasms. Different paper reported the increase risk of cancer in patients with SEL. Lewis, et al. reported an increased risk of malignity in 484 patients with SEL [8, 30].
Lymphomas and Soft tissue Sarcoma are more common in SEL than general population. Petterson series reported 12 female patients with thyroid cancer. However, other authors did not find this relation [8, 31]. In our serie of cases there are 3 female patients with SEL and thyroid cancer, as reported by Petterson. Different autoimmune elements produced by thyroid cancer are detected in SEL and RA patients, this clearly show coexist autoantibodies against the thyroid gland in patients with RD [32]. The patients with SEL have functional disorder in humoral and cellular immunity system. In thyroiditis, especially HT, parenchyma of thyroid gland is progressively lost and replaced by cells of the inflammatory infiltrate. The persistent stimulation of residual thyrocytes with such molecules could induce the activation of NF-β in follicular cells, thereby creating a functional network between thyroid epithelial cells and inflammatory cells [33].
This cytological alterations and nuclear modifications are similar to those of papillary carcinomas, suggesting that both neoplastic and autoimmune diseases could share the same molecular pathogenesis [34]. The mitogen-activated protein kinase (MAPK) signaling pathway is a foremost event in the carcinogenesis of the most common endocrine malignancy, the papillary thyroid carcinoma (PTC). Affected elements include RET/PTC re-arrangements and point mutations of the RAS and BRAF genes. Mutations in these genes are found in over 70% of PTC [35, 36]. Other concurrent factor detected in patients with AD is several viral infections that could contribute to development thyroid cancer, such as Hepatitis C infection. These patients have high levels of serum anti- thyroperoxidase and/or anti- thyroglobulin autoantibodies. Hepatitis C chronic infection shows a higher prevalence of papillary thyroid cancer than controls, in particular in patients with autoimmune thyroiditis [37].
Clinical presentation of the patients with SEL was hematologic symptoms, anemia, leucopenia and platelets diseases. Hematological complications are frequent in SEL and are considered as good prognosis compared to other organs involvement. Miranda reported thrombocytopenia (severe in 62%), it was the most common hematological feature followed by hemolytic anemia (severe in 37%) and neutropenia (severe in 89%) [38, 39]. On the other hand, the level serum antibodies thyroid in ours patients did not present a relevant change. Is precise to remember that less of 25 % patients with thyroid cancer have antibodies thyroid positive, and 10 % are present in normal population [40, 41]. One patient with thyroid cancer and both RD (SLE and RA). This clinical manifestation is called Rhupus syndrome or overlap syndrome between RA and SEL. However, this syndrome is still in debate, some consider as different entity and others as aggressive presentation of SLE, with bad prognosis same as our dead patient [42, 43]. Rubini analyzed clinical and serological data of 176 patients with diagnosis of Rhupus, derived from a total of 16 studies. A strong heterogeneity in the elements taken into account to establish the presence of Rhupus, reflecting the lack of consensus and validated criteria to define the disease [44, 45]. SEL affect several organ, the kidney appears to be one of the most common, and at the same time, more serious complication. The prevalence of renal disease ranged from 29 to 75%. The patients with lupus nephritis, despite treatment, 10-15% go into end stage renal failure [46, 47].
The recurrent lupus nephritis is common in patients with kidney transplant, those with major prevalence in case when was associated with a receiving kidney from living donor, as our patient [48]. On the other hand, the lung manifestation occur most commonly in SEL patients: pleural effusion 58%, as our results and a severe case of bilateral effusion 50% [49, 50]. The pulmonary hypertension occurs in 25% patients with SEL due to interstitial diseases, recurrent embolism and vasculitis. This is a bad prognosis because they develop pulmonary and heart failure same as our case [51]. The cardiac compromise is frequent in SEL patients, as ours cases; the first report was realized by Osler in 1895. The prevalence is variable; the range could be major 50%. The lupus can affect several cardiac structure (pericardium, myocardium and endocardium, valves, conduction tissue and coronary artery) [52, 53].
The bone fracture has several factors in the pathogenesis of the SEL; bone resorption is secondary to vasculitis and decrease of bone matrix secondary to use steroid therapy in the patients. Femoral head is the most affected 5-50 % reported by Resnick. Ours patients with Rhupus Syndrome received a hip replacement [54, 55]. The patients with RA have similar risk to develop cancer as SEL, but, still is controversial topic. Jianguang Ji, reported that RA had worse prognosis for all and many site specific cancer compared with patients without RA. Their series reported 64 patients with thyroid cancer, almost all older patients, different as our result [56, 57]. However, Hemminki, et al. [58] only found few cases of thyroid cancer related to RA, their series present major number case of lymphomas and squamous cell skin cancer.
Almost all of patients showed morning stiffness as reported by Ndongo S, et al. [59]. In the large overlapping field of infections and rheumatology, many autoimmune diseases may present as fever of unknown origin, and, on the other hand, many different infectious agents cause signs and symptoms mimicking a systemic autoimmune disease. Clinical manifestations affecting the skin and its annexes, oral cavity, joints, and periarticular structures and also major organs such as the heart and vascular system, lung, liver, spleen, and gastrointestinal tract can be initial symptoms of a systemic autoimmune disease. The good knowledge of underlying pathogenetic mechanisms of particular clinical manifestations, the through physical examination, and the accurate use and interpretation of laboratory, serological, and imaging findings are necessary skills in overcoming the challenging differential diagnosis [60].
The most frequent comorbidity reported by Rajaine was dyslipidemia (43.5%) followed by hypertension, as one of ours cases (37, 9%) and thyroid cancer the malignancy tumors most frequent in RA patients [61, 62]. The Rheumatoid factor is positive in ours patients as other paper 93% [63]. However, other paper reported low level of rheumatoid factor positive as in Angelotti study (65.5% of cases) [64]. The majority of ours patients with thyroid cancers are classic papillary. One case with previous HT similar as other paper. This has been a topic of discussion as other aspect of autoimmune diseases such as the rheumatic diseases [65, 66]. The question of How thyroid malignancies develop despite immune responses, or does disorder thyroiditis develop because of an antitumor immune response, or if the neoplasm arose from previous chronic inflammation [67].
Within this controversy, it is important to be clear about the role of cellular and humoral immunity [68, 69]. Ferrari reported cancer onset can be associated to the extended and serious immune stimulus linked to the autoimmune disease and paraneoplastic autoimmune diseases characterized by rheumatic manifestation that can occur before, contemporaneously or after the onset of the tumors [70]. Almost all the patients diagnosed in early stage and classified as Low Risk detected during the follow up for their rheumatic diseases. The standard treatment was total thyroidectomy plus I-131 ablation by positive nodal and capsular invasion. Total thyroidectomy as the primary initial surgical treatment option for nearly all differentiated thyroid cancer >1cm with or without evidence of loco-regional or distant metastases. The requirement for routine use of radio Iodine ablation (RIA) was one of the major reasons given in support of total thyroidectomy in low to intermediate risk patients, our current more selective approach to RAI ablation [71].
Only one case with right lobectomy, the case of SEL plus chronic failure kidney was a conservative consideration to reduce the risk of other complication. Often lobectomy was done based on proper selection of low to intermediate risk patients considering comorbidity conditions [72, 73, 74].
Conclusion
The rheumatic diseases (SEL and RA) concurrent in patients with thyroid cancer, were presented in the minority of cases in our little serie. The young woman was the most affected, the majority with Hematologic symptoms, there was a severe case with Rhupus syndrome that die for pulmonary complication. The patients with classic papillary thyroid cancer in early stage (low risk) were treated with total thyroidectomy plus radio iodine ablation in the majority of the cases without complications. Our results are similar as the international literature.
References
-
Abu Shakra M, Buskila D, Ehrenfeld M, Conrad K, Shoenfeld Y (2001) Cancer and autoimmunity: autoimmune rheumatic feature in patients with malignancies. Ann Rheum Dis 60(5): 433-441.
-
Sorokini I, Ben Mahrez K, Bracone A, Thierry D, Ishii S, et al. (1991) Presence of circulating anty-c-myb gen product antibodies in the human sera. Int J Cancer 47(5): 665-669.
-
Leonardo F, Rush V, Langenfeld J, Dmitrovsky E, Klimstra DS (1999) Overexpresion of Cyclid D and E is frequent in broncheal pre neoplasm and precedes squamous cell carcinoma development. Cancer Res 59(10): 2470-2476.
-
Laura Sterian Ward (2014) Immune Response in Thyroid Cancer: Widening the Boundaries. Scientifica 20.
-
Swissa M, Cohen Y, Shoenfeld Y (1992) Autoantibodies in the sera of patients with Lymphoma. Leuk Lymphoma 7(1-2): 117-122.
-
Love PE, Santora SA (1990) Antiphospholipid Antibodies: Anticardiolipin and the Lupus Anticoagulant in Systemic Lupus Erythematosus (SLE) and in Non-SLE Disorders: Prevalence and Clinical Significance. Annals Intern Med 112(9): 682-698.
-
Abu Shakra M, Shoenfeld Y (1993) Introduction to natural autoantibodies. Natural antibodies CRC press 15: 33.
-
Petterson T, Pukkala E, Teppo L, Frima C (1992) Increase of risk cancer in patients with Systemic Erythematous Lupus. Annals of Rheumatic Diseases 51(4): 437-439.
-
Boelaret K, Newby PR, Simmonds MJ, Holder RL, Carr Smith JD, et al. (2010) Prevalence and relative risk of other autoimmune disease in subject with Autoimmune Thyroid Diseases. Am J Med 123(2): 183.
-
American College of Rheumatology (2010) Ann Rheum Dis 69: 1580-1588
-
Lam A (2017) Pathology of endocrine tumors update: World Health Organization new classification 2017-other thyroid tumors. AJSP Rev Rep 22(4): 209-216.
-
Raue F, Raue KF (2016) Thyroid cancer: Risk Stratified Management and individualize theraphy. Clin Cancer Res 22(20): 5012-5021.
-
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. (2009) Revised American Thyroid Association. Guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19(11): 1167- 1214.
-
Robert U, Yawai Z (2014) The Epidemic of Thyroid Cancer in United State: The Role of Endocrinologist and Ultrasound. Thyroid 24(3): 472-479.
-
Davies L, Welch HG (2006) Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA 295(18): 2164-2167.
-
Kilfoy BA, Zheng T, Holford TR, Han X, Ward MH, et al. (2009) International patterns and trends in thyroid cancer incidence, 1973-2002. Cancer Causes and Control 20(5): 525-531.
-
Harach HR, Fransilla KO, Wasenius VM (1985) Occult papillary carcinoma of the thyroid. A “normal” finding in Finland. A systematic autopsy study. Cancer 56(3): 531- 538.
-
Ruggeri RM, Trimarchi F, Giuffrida G, Certo R, Cama E, et al. (2017) Autoimmune comorbidities in Hashimoto’s thyroiditis: different patterns of association in adulthood and childhood/adolescence. Eur J Endocrinol 176(2): 133-141.
-
Biro E, Szekanecz Z, Czirják L, Dankó K, Kiss E, et al. (2006) Association of systemic autoimmune diseases and autoimmune thyroid disease. Clin Rheumatol 25(2): 240-245.
-
Antonelli A, Mosca M, Fallahi P, Neri R, Ferrari SM, et al. (2010) Thyroid Cancer in Systemic Lupus Erythematosus: A Case-Control Study. J Clin Endocrinol Metabol 95(1): 314-318.
-
Soy M, Guldiken S, Arikan E, Altun BU, Tugrul A (2007) Frecuence of Rheumatic disease in patients with autoimmune thyroid diseases. Rheumatol Int 27(6): 575-577.
-
Weetman AP, Walpart MJ (1987) The Association of Autoimmune Thyroiditis with Systemic Lupus Erythematosus. Br J Rheumatol 26(5): 359-361.
-
Weetman AP (2011) Diseases associated with thyroid autoimmunity: explanations for the expanding spectrum. Clin Endocrinol 74(4): 411-418.
-
Tektonidou MG (2010) Presence of Other Autoimmune Diseases in Subjects with Autoimmune Thyroid Disease. Am J Med 23(10): e23.
-
Dailey ME, Lindsay S, Skahen R (1955) Relation of thyroid neoplasms to Hashimoto disease of the thyroid gland. AMA Arch Surg 70(2): 291-297.
-
Brown R, Francis GL (2011) Autoimmune Thyroid Disorders. Journal of Thyroid Research 2.
-
Balkwill F, Mantovani A (2001) Inflammation and cancer: back to virchow?. Lancet 357(9255): 539-545.
-
Cassou A, Congiu LA (2001) Adult Onset Still’s diseases: A rare association with Autoimmune Thyroiditis. Ann Rheum Diseases 60(Suppl 1).
-
Tuba Tüley Koca (2015) Association Thyroid Disorders and Rheumatic Diseases. Turk J Phys Med Rhab 61: 187- 189.
-
Lewis RB, Castor CW, Knisley RE, Bole GG (1976) Frequency of neoplasia in Systemic Erythematous Lupus and Rheumatoid Arthritis. Arthritis Rheum 19(6): 1256- 1260.
-
Kawano Y, Nambu M, Uejima Y, Sato S, Suganuma E, et al. (2017) Risk Factors for Thyroid Cancer in Systemic Lupus Erythematosus. Global Pediatric Health 4: 1-11.
-
Kebebew E, Treseler PA, Ituarte PH, Clark OH (2001) Coexisting Chronic Lymphocytic Thyroiditis and Papillary Thyroid cancer revisited. World J Surg 25(5): 632-637.
-
Pacifico F, Leonardi A (2010) Role of NF-κB in thyroid cancer. Mol Cell Endocrinol 321(1): 29-35.
-
Weetman AP (2004) Cellular immune responses in autoimmune thyroid disease. Clin Endocrinol 61(4): 405-413.
-
Ciampi R, Nikiforov YE (2007) RET/PTC rearrangements and BRAF mutations in thyroid tumorigenesis. Endocrinology 148(3): 936-941.
-
Cunha LL, Ferreira RC, Marcello MA, Vassallo J, Ward LS (2011) Clinical and Pathological Implications of Concurrent Autoimmune Thyroid Disorders and Papillary Thyroid Cancer. J Thyroid Res.
-
Fallahi P, Ferrari SM, Politti U, Giuggioli D, Ferri C, et al. (2014) Autoimmune and Neoplastic Thyroid Diseases Associated with Hepatitis C Chronic Infection. Int J Endocrinol.
-
Miranda D, Ángeles U (2014) Mortality in hospitalized patients with Systemic Erythematous Lupus with hematologic manifestation. Case control study. Annals Rheumatic Disease 73(Suppl 2).
-
Sule Yavuz Dondu Cansu (2019) What do Hematological abnormalities tell us in SEL, results from two independent multicenter european SEL cohorts. Annals Rheumatic Diseases 13: 393
-
Spencer CA, Lopresti JS, Fatemi S, Nicoloff JT (1999) Detection of residual recurrent differentiated thyroid carcinoma by serum thyroglobulin measurement. Thyroid 9(5): 435-441.
-
Hollowel JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, et al. (2002) Serum TSH, T (4) and thyroid antibodies in United State population (1988-1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab 87(2): 489-499.
-
Ikeda K, Sanayama Y, Makita S, Hosokawa J, Yamagata M, et al. (2013) Efficacy of Abatacept for Arthritis in Patients with an Overlap Syndrome between Rheumatoid Arthritis and Systemic Lupus Erythematosus. Clin Dev Immunol.
-
Panush RS, Edwards NL, Longley S, Webster E (1988) ‘Rhupus’ Syndrome. Arch Intern Med 148(7): 1633- 1636.
-
Rubini E, Grazietta S (2019) Annals Rheumatic Diseases.
-
Foddai SG, Rubini E (2019) The prevalence of Rhupus syndrome in a mono enteric tertiary referral cohort. Annals Rheumatic Diseases.
-
Wallace DJ, Podell TE, Weiner JM, Cox MB, Klinenberg JR, et al. (1982) Lupus nephritis. Experience with 230 patients in a private practice from 1950 to 1980. Am J Med 72(2): 209-220.
-
Mavragani CP, Moutsopoulos H (2003) Lupus nephritis: current issues. Ann Rheum Dis 62(9): 795-798.
-
Norby GE, Strøm EH, Midtvedt K, Hartmann A, Gilboe IM, et al. (2010) Recurrent Lupus nephritis after kidney transplant. Ann Rheum Dis 69(8): 1484-1487.
-
Omer SB Alamoudi, Suzan M Attar (2015) Pulmonary manifestation in Systemic Lupus Erythematous. Respiratory 20(3): 474-480.
-
Lalani TA, Kanne JP, Hatfield GA, Chen P (2004) Imagine finding in Systemic Lupus Erythematous. Radiography 24(4): 1069-1086.
-
Minai O (2009) An update in Pulmonary hypertension in Systemic Erythematous Lupus-do we need to know about it?. Lupus 18(1): 92.
-
Ashrafi R, Garg P, McKay E, Gosney J, Chuah S, et al. (2011) Aggressive Cardiac Involvement in Systemic Lupus Erythematosus: A Case Report and a Comprehensive Literature Review. Cardiol Res Pract 578.
-
Appengeller S, Pineau CA, Clarke AE (2011) Acute lupus myocarditis: Clinical features and outcome. Lupus 20(9): 981-988.
-
Resnick D (1996) Bone and Join imagine. 2nd (Edn.), Philadelphia, Saunder.
-
Tasneem AL, Kanne JP, Hatfield GA, Chen P (2014) Imagine finding in SEL. Radiographics 24(4): 1069-1086.
-
Jianguang Ji, Xiangdong Liu, Sundquist K, Sundquist J (2011) Survival of cancer in patients with rheumatoid arthritis: a follow up study in Sweden of patients hospitalized with rheumatoid arthritis 1 years before diagnosis of cancer. Rheumatology 50(8): 1513-1518.
-
Huang WK, Chiou MJ, Kuo CF, Lin YC, Yu KH, et al. (2014) No overall increased risk of cancer in patients with rheumatoid arthritis: a nation wide dynamic cohort study in Taiwan. Rheumatology International 34(10): 1379-1386.
-
Hemminki K, Li X, Sundquist K, Sundquist J (2008) Cancer risk in hospitalized rheumatoid arthritis patients. Rheumatology 47(5): 698-701.
-
Ndongo S, Lekpa FK, Ka MM, Ndiaye N, Diop TM (2009) Presentation and severity of rheumatoid arthritis at diagnosis in Senegal. Rheumatology 48(9): 1111-1113.
-
Haralampos MM, Evangelia Z, Vlachoyiannopoulos PG (2018) Rheumatic Manifestations: A Compilation. Rheumatology in Questions 141-150.
-
Namas R, Joshi A, Ali Z, Jamal Al S, Abuzakouk M (2019) Demographic and Clinical Patterns of Rheumatoid Arthritis in an Emirati Cohort from United Arab Emirates. International Journal of Rheumatology 10.
-
Innala L, Sjoberg C, Moller B, Ljung L, Smedby T, et al. (2016) Co-morbidity in patients with early rheumatoid arthritis - inflammation matters. Arthritis Research & Therapy 18(1): 33-40.
-
Claudia Ickinger, Eustasius Musenge, Mohammed Tikly (2011) Rheumatoid arthritis-clinical aspects: 134. Predictors of Joint Damage in South Africans with Rheumatoid Arthritis. Rheumatology 50(Suppl 3): 93- 104.
-
Teh CL, Wong JS (2008) The pattern and clinical manifestations of rheumatoid arthritis in Sarawak General Clinical. Rheumatology 27(11): 1437-1440.
-
Lee JH, Kim Y, Choi JW, Kim YS (2013) The association between papillary thyroid carcinomaand histologically proven Hashimoto’s thiroiditis: a meta- analysis. Eurp Jour Endocrin 168(3): 343-349.
-
Min Zhang, Xiao ML, Guo SW, Long Q, Jin HT, et al. (2014) The thyroid cancer in systemic Erythematous Lupus: a meta-analysis. Int J Clin Exp Pathol 7(9): 6270-6273.
-
Ehlers M, Schott M (2014) Hashimoto’s thyroiditis and papillary thyroid cancer: are they immunological link?. Trends Endocrinol Metab 25(12): 656-664.
-
Francesco F, Maria GC, Nicoleta F (2017) Thyroid autoimmunity and cancer. Endocrin Immunol 48: 97- 109.
-
Nagayama Y (2018) Thyroid Autoimmunity and thyroid cancer-The pathogenesis connection. Update Horm Metab Res 50(12): 922-931.
-
Ferrari SM, Elia G, Virili C, Centanni M, Antonelli A, et al. (2017) Systemic Lupus Erythematous Lupus and thyroid Autoimmunity. Front Endocrinol (Lausanne) 8: 138.
-
Ruel E, Thomas S, Dinan M, Perkins JM, Roman SA, et al. (2015) Adjuvant radioactive iodine therapy is associated with improved survival for patients with intermediate- risk papillary thyroid cancer. J Clin Endocrinol Metab 100(4): 1529-1536.
-
Mendelsohn AH, Elashoff DA, Abemayor E, St John MA (2010) Surgery for papillary thyroid carcinoma: is lobectomy enough?. Arch Otolaryngol Head Neck Surg 136(11): 1055-1061.
-
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, et al. (2016) 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 26(1): 1-133.
-
Nguyen XV, Roy Choudhury K, Tessler FN, Hoang JK (2018) Effect of tumor size on risk metastatic disease. Thyroid 28(3): 295-300.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty