Primary Hyperparathyroidism due to Ectopic Intrathymic Parathyroid Adenoma in A Child: A Case Report
Primary hyperparathyroidism (PHPT) is a rare endocrine disorder in children and adolescents. Surgery is curative in most pediatric patients with PHPT. PHPT due to ectopic parathyroid adenoma (EPA) presents the difficulty of their exact topographic diagnosis and there is no consensus for the optimal imaging modality. The 99mTc-sestamibi (99mTechnetium -labeled methoxy-isobutyl-isonitrile) scintigraphy appears to be the best exam to establish a topographic diagnosis of parathyroid adenoma. Herein, we present the case of a 14-year-old girl with the diagnosis of PHPT with bone involvement. Parathyroid scintigraphy (dual-phase and dual tracer subtraction imaging), has shown an abnormal tracer uptake in the anterior mediastinum. Computed tomography (CT), has confirmed the mediastinal seat of the adenoma, measured 40 x 24.6 mm, repressing the thymus. An adenectomy was performed using video-assisted mini-thoracoscopic surgery. Histological findings have shown intrathymic ectopic parathyroid adenoma. After surgery, the patient had profound and persistent hypocalcemia as a result of extensive remineralization in a relation to Hungry Bone Syndrome (HBS). Through this clinical report, we insist on the importance of preoperative localization of parathyroid adenoma to select the surgical approach and to avoid failed cervicotomy especially in cases of ectopic adenomas.
Ben Nasr Maali1*, El Ajmi Wassim1, Hadj Dahmane Mariem2, Abdennadher Mahdi2, Sellem Ali1 and Hammami Hatem1
Introduction
Primary hyperparathyroidism (PHPT) is rarely described in children and may be misdiagnosed. PHPT is caused by a solitary parathyroid adenoma in 65%-70% of children [1, 2]. Ectopic parathyroid adenoma (EPA) is a rare entity, accounting for 6%-16% of all parathyroid adenomas and the most common ectopic location is the thymus, which accounts for 38% of EPA [3]. In all pediatric PHTP patients, surgical removal is the only curative option [4].Thus, accurate preoperative localization of parathyroid adenomas is essential. Advanced imaging techniques provide a more precise localization, and it is now possible to consider a minimally invasive mediastinal approach in children. On this basis, 99mTc-sestamibi single-photon emission computed tomography (SPECT) and 99mTc- sestamibi SPECT/CT may be the optimal imaging modality [5]. Here, we report a rare case of PHPT due to ectopic mediastinal parathyroid adenoma in a 14-year-old girl to highlight the importance of 99mTc-sestamibi scintigraphy in the surgical management of PHPT.
Case Description
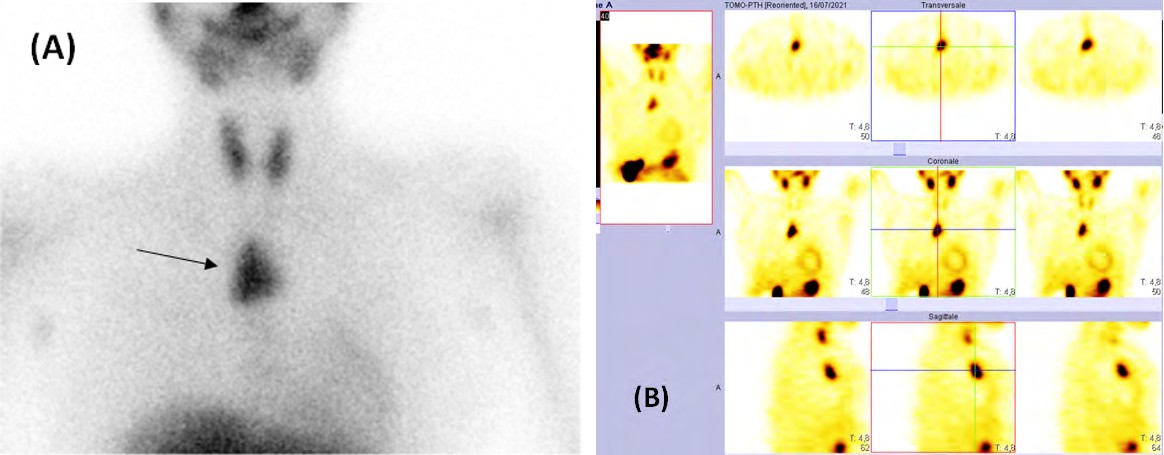
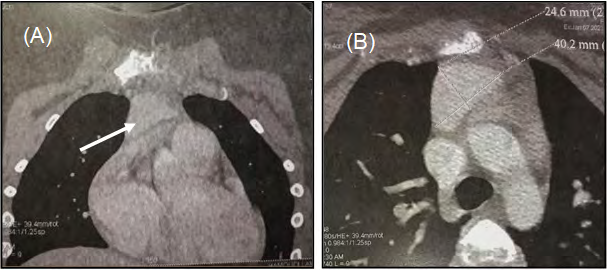
A 14-year-old girl with no previous medical or surgical history was admitted for a pathological fracture of the right femoral cervix complicating PHTP. Laboratory evaluation showed hypercalcemia (3,2mmol/l; reference range, 2,2-2,6mmol/l), hypophosphatemia (0,7mmol/l; reference range, 1,3-1,85mmol/l), elevated parathyroid hormone (2490pg/mL; reference range ,15-65pg/mL), elevated alkaline phosphatase (3682U/L ; reference range , 100- 400UI/L), elevated 24-hour urine calcium (10,36mmol/L; reference range, 0,05-0,1mmol/kg/24 hours) and vitamin D deficiency (25-OH-vitamin D level of 3,49ng/mL; reference range, 30-80ng/mL). Radiological findings have shown low bone density and multiple, variable-sized osteolytic lesions of the axial and peripheral skeleton consistent with metabolic osteodystrophy. Renal ultrasonography has shown no signs of nephrocalcinosis. Neck ultrasonography was normal. Parathyroid scintigraphy (dual-phase and dual tracer subtraction imaging), revealed a large area of increased tracer uptake in the anterior mediastinal region correlating with an EPA (Figure 1). The patient underwent a neck computed tomography (CT) with contrast injection that
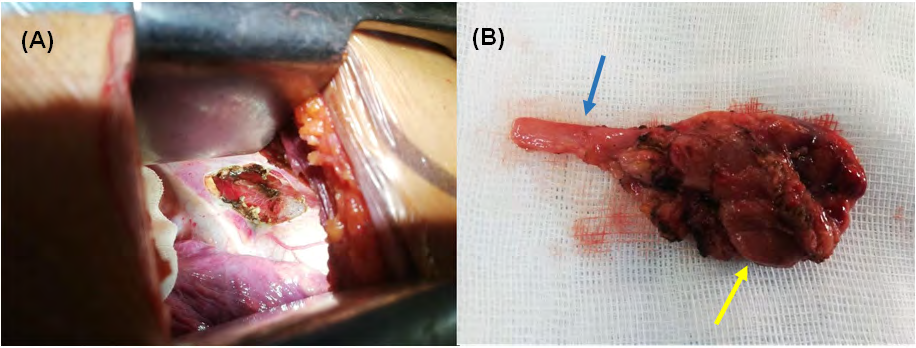
confirmed the mediastinal seat of adenoma, measured 40 x 24.6 mm, repressing the thymus gland, in direct contact with the pericardium, the right atrium and the left brachio-cephalic vein trunk, and at a distance from the large mediastinal vessels (Figure 2). There was no evidence of multiple endocrine neoplasia syndrome, familial hyperparathyroidism- jaw tumor syndrome, or family history of endocrinopathies. Magnetic resonance imaging (MRI) of the pituitary gland was normal and thoraco-abdomino-pelvic CT was unremarkable. Subsequently, the child was referred to the thoracic surgery department after treating the hypercalcemia and the femoral fracture. She underwent a video-assisted right lateral mini- thoracotomy. During the act, the ectopic parathyroid gland was found to be within the thymus. A right thymectomy was performed (Figure 3). The anatomopathological study concluded to an intrathymic parathyroid adenoma. It showed a well circumscribed nodule with a thin fibrous capsule, composed of rounded monomorphic cells with granular eosinophilic cytoplasm and regular central nuclei. Areas of hemorrhagic degeneration and calcifications were observed. The nodule was surrounded by residual thymic parenchyma. There was no evidence of lymphovascular invasion, perineural invasion or invasion into adjacent structures. During the postoperative period, the patient had persistent hypocalcemia and hypophosphatemia as a result of extensive remineralization in a relation to Hungry Bone Syndrome (HBS). She required prolonged oral calcium and calcitriol supplements. At the 6th month follow-up, serum calcium, phosphate, parathyroid hormone, alkaline phosphatase values were completely normal.
Discussion
PHPT is uncommon in the pediatric population. Unlike adult patients, children with PHPT can present with nonspecific symptoms; therefore, diagnosis may be delayed. In our case, the patient presented with a right femoral fracture complicating severe bone involvement. Most cases of PHPT are caused by sporadic isolated adenomas. However, autosomal dominant hyperparathyroidism and familial syndromes such as Multiple Endocrine Neoplasia (MEN) type I and IIA, and hyperparathyroidism jaw tumor syndrome, may also present with a single parathyroid adenoma in a child [6]. Genetic screening in children diagnosed with hyperparathyroidism is essential, as genetic mutations are observed in 24% to 46% of children with PHPT [7]. Detailed family history along with careful explorations did not suggest any evidence of MEN in our case.
PHPT due to EPA is a rare entity. The lower parathyroid glands develop from the third pharyngeal pouch in close association with the thymus. As a result, they may be found commonly within the anterosuperior mediastinum making the thymus the most common ectopic site for a parathyroid gland [2]. The curative treatment of PHPT in children is surgical removal. The traditional surgical approach has been bilateral neck exploration, a trans-sternal or transthoracic approach in cases with deep mediastinal parathyroid lesions. However, the improved sensitivity of imaging techniques has encouraged the use of less invasive surgical procedures in adults. Nowadays, recent studies have shown that minimally invasive mediastinal ectopic parathyroidectomy is safe and feasible if the anatomical position of any lesions is well determined, even in children [8, 9, 10]. Locating EPA preoperatively can be challenging. Both 99mTc-sestamibi scintigraphy and neck ultrasonography (US) are considered as the first-line preoperative imaging modalities in patients with PHPT [11]. In a meta-analysis of 43 preoperative localization technique studies, Cheung et al. have demonstrated that ultrasound and 99mTc-sestamibi-SPECT have comparable accuracy, with pooled sensitivities of 76.1% and 78.9%, respectively, and positive predictive values of 93.2% and 90.7%, respectively [12]. Thus, 99mTc-sestamibi-SPECT is recognized as the most sensitive imaging method in PHPT (sensitivity per adenoma, 95%) [13]. In fact, tomographic three-dimensional reconstruction improves separation between the activity in the thyroid gland and a parathyroid adenoma situated behind the thyroid. False-negative results can be caused by a small parathyroid adenoma, multiple adenomas, and hyperplasia. Recently, the emerging of 18F-fluorocholinepositron emission tomography/computed tomography may play a role as a second-line imaging in patients with PHPT and can also improve the localization of the hyperparathyroid glands [14]. In our case, 99mTc- sestamibi SPECT scanning had successfully detected EPA and the patient required a preoperative thoracic CT for more precise anatomic information.
Conclusion
In sum, PHTP in children is unusual. Surgical removal is the only curative treatment for children with PHTP. Accurate preoperative localization of the target lesion is critical. Detection methods include preoperative 99mTc-sestamibi scan, which has the advantage of detecting ectopic adenomas, thus allowing a minimally invasive therapeutic approach.
Conflict of Interest: The authors declare that they have no conflict of interest.
References
-
Kollars J, Zarroug AE, Heerden VJ, Lteif A, Stav- lo P, et al. (2005) Primary hyperparathyroidism in pedi- atric patients. Pediatrics 115(4): 974‑980.
-
Nicholson KJ, McCoy KL, Witchel SF, Stang MT, Carty SE, et al. (2016) Comparative characteristics of primary hyperparathyroidism in pediatric and young adult pa- tients. Surgery 160(4): 1008-1016.
-
Roy M, Mazeh H, Chen H, Sippel RS (2013) Inci- dence and localization of ectopic parathyroid adenomas in previously unexplored patients. World J Surg 37(1): 102-106.
-
Bilezikian JP (2018) Primary Hyperparathyroidism. J Clin Endocrinol Metab 103(1): 3993-4004.
-
Dasgupta DJ, Navalkissoor S, Ganatra R, Buscombe J (2013) The role of single-photon emission computed tomography/computed tomography in localizing parathyroid adenoma. Nucl Med Commun 34(7): 621- 626.
-
Roizen J, Levine MA (2012) Primary hyperparathyroidism in children and adolescents. J Chin Med Assoc 75(9): 425-434.
-
Alagaratnam S, Kurzawinski TR (2015) Aetiology, Diagnosis and Surgical Treatment of Primary Hyperparathyroidism in Children: New Trends. Horm Res Paediatr 83(6): 365-375.
-
Chou PL, Chao YK, Liu YH (2019) minimally invasive removal of mediastinal ectopic parathyroid glands: A single-center experience. Formos J Surg 52(1): 6-10.
-
Said SM, Cassivi SD, Allen MS, Deschamps C, Nichols FC, et al. (2013) Minimally invasive resection for mediastinal ectopic parathyroid glands. Ann Thorac Surg 96(4): 1229-1233.
-
Mancilla EE, Levine MA, Adzick NS (2017) Outcomes of Minimally Invasive Parathyroidectomy in Pediatric Patients with Primary Hyperparathyroidism due to Parathyroid Adenoma: A Single Institution Experience. J Pediatr Surg 52(1): 188-191.
-
Treglia G, Trimboli P, Huellner M, Giovanella L (2018) Imaging in primary hyperparathyroidism: focus on the evidence-based diagnostic performance of different methods. Minerva Endocrinol 43(2): 133-143.
-
Cheung K, Wang TS, Farrokhyar F, Roman SA, Sosa JA (2012) A meta-analysis of preoperative localization techniques for patients with primary hyperparathyroidism. Ann Surg Oncol 19(2): 577-583.
-
Oksuz MO, Dittmann H, Wicke C, Mussig K, Bares R, et al. (2011) Accuracy of parathyroid imaging: a comparison of planar scintigraphy, SPECT, SPECT-CT, and C-11 methionine PET for the detection of parathyroid adenomas and glandular hyperplasia. Diagn Interv Radiol Ank Turk 17(4): 297-307.
-
Pretet V, Rotania M, Helali M, Ignat M, Vix M, et al. (2020) 18F-Fluorocholine PET and Multiphase CT Integrated in Dual Modality PET/4D-CT for Preoperative Evaluation of Primary Hyperparathyroidism. J Clin Med 9(6): 2005.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty