Primary Adrenal Insufficiency Due to Extra pulmonary Tuberculosis in a Patient without HIV: A Case Report
Adrenal or adrenal insufficiency deals with a special pathology that has multiple etiologies and is characterized by deficiency in the secretion of steroids at this level. Around 80% of these etiologies are of autoimmune origin, however, the rest are due to infectious causes, infiltrative, genetic, vascular, neoplastic and even pharmacological diseases. The diagnosis requires high suspicion and treatment dependent on the cause. It is a life-threatening pathology that has a very broad etiology, and it does not always present as a frank adrenal crisis; therefore, high diagnostic suspicion is important.
Introduction
From 1563, Bartolommeo Eustachio’s described the adrenal glands for the first time as [1]. Three hundred years later, in 1855, Thomas Addison described the symptoms and signs observed in 11 patients who died of a disease of the adrenal glands: “anemia ... sagging of the action of the heart ... a peculiar change of color in the skin which occurs in relation to a disease of the adrenal glands defining this disorder as adrenal melisma. ”In his report, Addison showed that the adrenal glands in six of these patients were affected by tuberculosis, in three by cancer, by bleeding in one and due to idiopathic fibrosis in another [2]. Adrenal (adrenal) insufficiency is characterized by the inability of the adrenal cortex to produce sufficient amounts of glucocorticoids and mineralocorticoids [3]. In the case of primary adrenal insufficiency, this will be the result of elevated ACTH and low serum cortisol levels. The prevalence of primary adrenal insufficiency in Western societies is around 100-144 cases per million. There is a real increase in prevalence, related to a general underestimation of prevalence in the past and improvements in diagnostic conditions [4].
The reported prevalence in Europe has increased over time from 39 cases/million in England in 1968 [5], 60 in Denmark in 1974 (8), 93 in Coventry (UK) in 1992 [6], 110 in Nottingham (UK). Kingdom in 1993 [7], and 131 in Sweden in 2009 [8]. Data from other parts of the world are sparse and generally report a lower incidence; for example, in Japan the prevalence is 5 cases/million, 37% of which are caused by tuberculosis [9]. The estimated incidence of AD in Europe ranges between 4.4 and 6.2 new cases/million/year in different studies [3]. Today, in Western societies, 80% is caused by autoimmune adrenalitis followed by tuberculosis or other infectious diseases (eg, HIV/AIDS, CMV, candidiasis, histoplasmosis, syphilis, and others) and malignant diseases (eg, cancer lung, breast, colon and others) in approximately 10% of cases. Remaining causes include adrenalectomy (bilateral) (eg, for Cushing’s syndrome or adrenal tumors), genetic diseases (eg, congenital adrenal hyperplasia (CAH), congenital adrenal hypoplasia, adrenoleukodystrophy in men), and adrenal hemorrhage (eg, Waterhouse-Friderichsen syndrome in sepsis) [10, 11, 12]. The diagnosis is often overlooked and delayed; therefore, the first presentation is an acute life-threatening adrenal crisis in the emergency department.
Case Presentation
A 69-year-old male with a history of exposure to chronic coughing agents and a history of a son with pulmonary tuberculosis diagnosed and treated ten years earlier. He has three previous hospitalizations secondary to unintended weight loss, as well as hypotension and fluid and electrolyte imbalance at the expense of hyponatremia and hypercalcemia associated with acute kidney injury. His symptoms began six months prior to his admission with asthenia, adynamia, Laboratories upon admission general malaise, unintended weight loss of 12% of his body weight, as well as intolerance to the oral route, for which he sees a medical doctor who gives unspecified treatment no improvement. Due to the persistence of said symptoms, he went to the adult emergency room for evaluation. Upon admission, he arrived with TA 90/50, HR 105, FR 22, Temp 36.7ªC, he entered with low-cost data, so they began aggressive management with fluids as well as vasopressors and entered internal medicine. Upon admission to internal medicine, he was admitted with double vasopressor support, and the physical examination revealed pale skin, with hyperpigmentation in nails and oral mucosa, with cachectic and tachycardial fascies, with little oral intake, and was admitted with acute kidney injury. KDIGO 2; and bicytopenia at the expense of leukopenia and WHO grade I hypochromic normocytic anemia, as well as fluid and electrolyte imbalance at the expense of hypercalcemia and asymptomatic euvolemic hypoosmolar chronic moderate hyponatraemia and hypochloremia.
| Complementary studies | Findings |
|---|---|
| Hematic biometric | Leukocytes 3.55 10x3/UL, neutrophils 1.33 10x3/UL, lymphocytes 1.49 10x3/UL, monocytes 0.36 10x3/UL, eosinophils 0.24 10x3/UL, erythrocytes 4.02 10x3/UL, Hemoglobin 10.0 g/dL, hematocrit 32.4%, corpuscular volume medium 80.6 fL, medium corpuscular hemoglobin 24.8 pg, platelets 264 10x3/UL. |
| Clotting times | PT 15.3 sec, RNI 1.34, TTP 32.6 sec. |
| Acute phase reactants | Procalcitonin 0.01 ng/ml, Ferritin 1018.5 ng/dL, C-reactive protein 1.40 mg/dL. |
| Blood chemistry | Creatinine 5.81 mg/dL, Glucose 55 mg/dL, BUN 58 mg/dL, CK 78 U/L, CK-MB 18 U/L. |
| Liver chemistry | Total bilirubin 0.6 mg/dL, Glutamic oxaloacetic transaminase 36 U/L, Glutamic pyruvic trans- aminase 16 U/L, Albumin 3.4 g/L, Alkaline phosphatase 48 U/L, Gamma glutamyl transpepti- dase 20 U/L, Lactic dehydrogenase 145 U/L. |
| Serum electrolytes | Na 129 meq/L, K 5.4 meq/L, Cl 96 meq/L, Ca 13.1 mg/dL, corrected for albumin 13.6 mg/dL; phosph 3.0 mg/dL, Mg 1.31 mg/dL. |
The bicytopenia approach is carried out, as well as suspicion of multiple myeloma because it came with hypercalcemia, acute kidney injury, anemia, however no bone lesions were documented:
| TORCH Profile | IGG cytomegalovirus 47.8 AU/ml, IGM 0.31 AU/ml, IGG Rubella 5.2 IU/mL, IGM rubella non- reactive, IGG toxoplasma 0.06 IU/mL, IGM toxoplasma non-reactive, VDRL negative. |
|---|---|
| Viral panel | Non-reactive HIV, HBsAg, HCV and HAV IgM. |
| Peripheral blood smear | Rouleaux phenomenon. |
| Corrected reticulocytes | 0.6. |
| Iron Kinetics | Ferritin 1023, Seric Iron 80 mcg/dL, Transferrin 110 mg/dL |
| Occult blood in stool | Negative. |
| Bone marrow aspirate | Decreased cellularity, no evidence of infiltration due to malignancy. |
| Bone marrow biopsy | Hypercellularity for age (60%), reactive with the presence and maturation of the three series and moderate eosinophilia. Presence of plasma cells in 4% (Kappa positive, Lambda positive). Fibrosis grade I on the Thiele scale. |
| Flow cytometry for multiple myeloma | No plasma cells were found in the sample. The granulocytic series that represents 40.94% of total cellularity is diminished, shows asynchrony in maturation, there is a decrease in the promyelocyte, myelocyte and metamyelocyte stage. The monocytic series that represents 5.29% of the total population does not present asynchrony in its maturation stages, absence of aberrant markers. Erythroid population is increased and represents 21.36% of the entire population of total cellularity. The lymphoid population, which represents 5.36% of the total population, is diminished. There are no aberrant markers. |
As part of the approach to consumptive syndrome and intorerance to the oral route, as well as to rule out malignant causes of hypercalcemia, the following approach of laboratory and office studies is carried out:
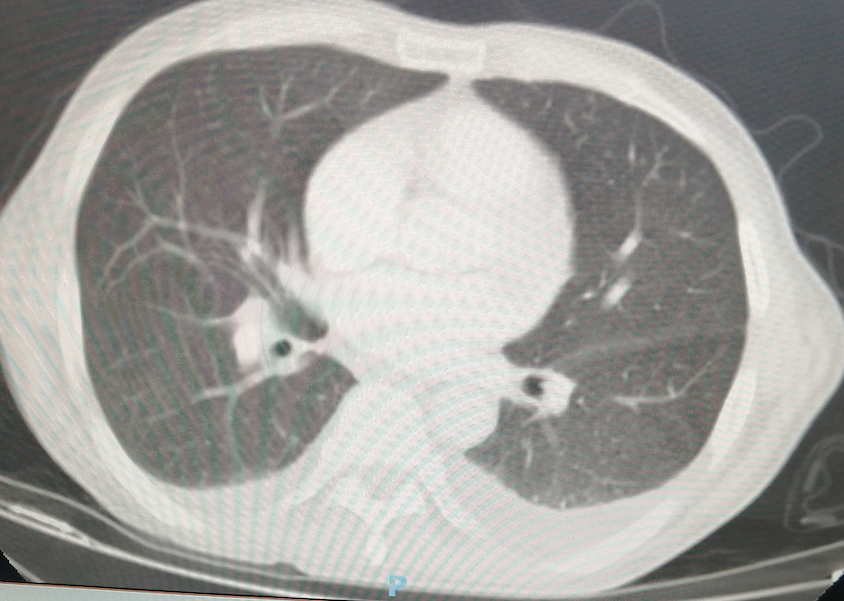
Simple and contrasted computed tomography of the skull, neck, thorax, abdomen and pelvis Calcified pulmonary granuloma in the right lung; adrenal glands without apparent anatomical alterations, the rest without alterations.
Prostate specific antigen 0.346 ng/ml.
Panendoscopy Without alterations.
Because the patient persisted with hypotension, a neoplastic process had been ruled out, the euvolemic hyponatremia approach was performed denoting Osm Urin greater than 100, as well as Na Urin greater than 30, which despite the use of diuretics for the treatment of hypercalcemia and to the depleted extracellular fluid and the low output data gives to rule out adrenal insufficiency, salt- losing brain syndrome or salt-losing kidney as well as the etiologies of this. For the part of malignant hypercalcemia, you have to take levels of PTHrP, 1,25 dihydroxyvitamin D, 25 hydroxyvitamin D.
| Intact PTH | <3.00 pg/mL. |
|---|---|
| PTH-related peptide | <1.02 pmol/L (negative) - (<1.02 pmol/L). |
| 1,25-dihydroxyvitamin D | <5 pg/mL (low) - (19.9-79.3 pg/mL). |
| 25-hydroxyvitamin D | 8.2 ng/mL (30-100 normal, 20-29 insufficient, <20 poor). |
| Protein gel electrophoresis | No monoclonal peaks. |
| Morning serum cortisol | 5.2 mcg/dL. |
| Thyroid function tests | Total T3 <1.2 ng/ml, Free T4 1.04 ng/dL, Total T4 8.66 ng/dl, TSH 3.82 uUl/ml. |
| Morning ACTH quantification | 186 pg/mL (elevated). |
| Specific antibodies | Anti-peroxidase, anti-thyroglobulin, 21-hydroxylase, anti-glutamic acid decarboxylase, and anti-islet cells: negatives. |
Similarly, because the morning serum cortisol was at the lower lower limit, adrenal insufficiency was documented with the intravenous insulin-induced hypoglycemia test with the following results:
| Intravenous insulin-induced hypoglycemia test | ||||
|---|---|---|---|---|
| Minutes | Start | 15 min | 30 min | 45 min |
| Serum glucose | 71 mg/dL. | 67 mg/dL. | 59 mg/dL. | 47 mg/dL. |
| Serum cortisol | 2.1 mcg/dL. | 1.3 mcg/dL. | 1.91 mcg/dL. | 1.97 mcg/dL. |
Due to the history of living with chronic coughs, PPD is performed, resulting in positive results, and with the complementary tests already mentioned, the diagnosis of primary adrenal insufficiency due to extrapulmonary tuberculosis is integrated. It is important to note that despite having a positive PPD, it only serves to assess latent tuberculosis, and by epidemiological definition, if there is extrapulmonary activity (in this case, adrenal insufficiency) without the need for lesions in imaging studies, together with Since the patient did not present respiratory symptoms or any other finding of pulmonary tuberculosis, it was classified as active extrapulmonary tuberculosis. It is said that in patients without HIV, extrapulmonary tuberculosis is extremely rare, and it can only be documented in about 6% of cases, making it a diagnostic challenge. Treatment was given with hydrocortisone 25 milligrams for 48 hours, responding adequately and improving blood pressure levels, and subsequently, he was switched to prednisone 5 milligrams a day and treatment for latent tuberculosis was given with isoniazid, rifampicin, and pyrazinamide and ethambutol, improving significantly.

Discussion
Primary adrenal insufficiency can be classified according to its etiology as autoimmune, infectious (as in this case), infiltrative, alterations in metabolism, granulomatous and genetic [13]. The onset of adrenal insufficiency is usually very gradual and may go unrecognized until illness or other stress precipitates an adrenal crisis. The presenting signs and symptoms of primary adrenal insufficiency are often nonspecific, leading to long delays in diagnosis. Non-specific characteristics include [14, 15, 16]:
- Fatigue (84 to 95%).
- Weight loss (66 to 76%); weight loss is mainly due to anorexia. The amount of weight lost can range from 2 to 15 kg and may not be evident until the adrenal insufficiency is advanced.
- Nausea, vomiting, abdominal pain (49 to 62%).
- Muscle and joint pain (35 to 40%).
Signs and symptoms that are more specific to primary adrenal insufficiency. These include [14]:
- Hyperpigmentation of the skin (41-74%), due to increased production of proopiomelanocortin (POMC), a prohormone that is cleaved into the biologically active hormones corticotropin (ACTH), melanocyte- stimulating hormone (MSH), and others. Elevated MSH results in increased melanin synthesis, causing hyperpigmentation.
- Postural hypotension (55 to 68%), due to mineralocorticoid deficiency.
- Desire for salt (38 to 64%).
The most common laboratory findings include [14]:
- Hyponatremia (70 to 80%)
- Hyperkalemia (30 to 40%)
- Anemia (11 to 15%)
- Hypercalcemia (6%) Confirmation of the diagnosis of adrenal insufficiency consists of 3 stages:
- Demonstrate inappropriately low cortisol secretion
- Determine whether cortisol deficiency is dependent or independent of ACTH deficiency and evaluate mineralocorticoid secretion in patients without ACTH deficiency.
- Look for a treatable cause of the primary disorder (eg, infiltrative process, autoimmune, etc.) [13]. In the case of the patient, it was a treatable cause secondary to latent tuberculosis, which was adequately treated and subsequently referred.
The 2016 Endocrine Society guidelines suggest the standard high-dose test of 250 mcg of corticotropin; however, in our case, as it is a high-cost test, it was decided to carry out the stress test with intravenous insulin, corroborating the insufficiency of serum cortisol secretion with said stimulation, in addition to the previously mentioned diagnostic approach. For treatment, hormone replacement and treating the triggering cause is recommended. In general, a variety of replacement doses are recommended, including 5 mg/m 2 given three times a day, 10 mg in the morning and 5 mg in the evening, 20 mg total dose, and 15 to 25 mg daily given in two. or three divided doses [12].
Conclusion
Adrenal insufficiency is a critically important and life- threatening disease if not properly identified. It has a very broad etiology which is important to recognize for it; give the appropriate therapy, as well as identify said etiologies and influence prevention when possible.
References
-
Eustachius B (1563) Opuscula anatomica de renum structura, efficio et administratione. In: Luchino V, et al. (Eds.), Venice.
-
Addison T (1855) On the constitutional and local effects of disease of the supra-renal capsules. Br Foreign Med Chir Rev 18(36): 404-413.
-
From the American Association of Neurological Surgeons (AANS), American Society of Neurological Surgeons (ASNR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE), Canadian Interventional Radiology Association (CIRA), Congress of Neurological Surgeons (CNS), at al. Sacks D, Baxter B, Campbell B, Carpenter JS, Cognard C, et al. (2018) Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. International journal of stroke: official journal of the International Stroke Society 13 (6): 612-632.
-
Erichsen MM, Lovas K, Fougner KJ, Jens B, Jens PB, et al. (2009) Normal overall mortality rate in Addison’s disease, but young patients are at risk of premature death. Eur J Endocrinol 160(2): 233-237.
-
Mason AS, Meade TW, Lee JA, Morris JN (1968) Epidemiological and clinical picture of Addison’s disease. Lancet 2(7571): 744-747.
-
Willis AC, Vince FP (1997) The prevalence of Addison’s disease in Coventry, UK. Postgrad Med J 73(859): 286- 288.
-
Kong MF, Jeffocoate W (1994) Eighty-six cases of Addison’s disease. Clin Endocrinol 41(6): 757-761.
-
Bjornsdottir S, Sundstrom A, Ludvigsson JF, Blomqvist P, Kampe O, et al. (2013) Drug prescription patterns in patients with Addison’s disease: a Swedish population- based cohort study. J Clin Endocrinol Metab 98(5): 2009- 2018.
-
Takayanagi R, Miura K, Nakagawa H, Nawata H (2000) Epidemiologic study of adrenal gland disorders in Japan. Biomed Pharmacother 54 (Supp1): 164s-168s.
-
Arlt W, Allolio B (2003) Adrenal insufficiency. Lancet 361(9372): 1881-1893.
-
Bornstein SR (2009) Predisposing factors for adrenal insufficiency. N Engl J Med 360(22): 2328-2339.
-
Betterle C, Morlin L (2011) Autoimmune Addison’s disease. Endocr Dev 20: 161-172.
-
Betterle C, Presotto F, Furmaniak J (2019) Epidemiology, pathogenesis, and diagnosis of Addison’s disease in adults. J Endocrinol Invest 42 (12): 1407-1433.
-
Banks I, Hahner S, Tomlinson J, Arlt W (2015) Diagnosis and treatment of adrenal insufficiency. Lancet Diabetes Endocrinol 3(3): 216-226.
-
Erichsen MM, Lovas K, Skinningsrud B, Anette BW, Dag EU, et al. (2009) Clinical, immunological and genetic characteristics of autoimmune primary adrenal insufficiency: observations from a Norwegian registry. J Clin Endocrinol Metab 94(12): 4882-4890.
-
Mitchell AL, Pearce SH (2012) Autoimmune Addison disease: pathophysiology and genetic complexity. Nat Rev Endocrinol 8: 306-316.
-
Crown A, Lightman S (2005) Why is the treatment of glucocorticoid deficiency still controversial? A review of the literature. Clin Endocrinol 63(5): 483-492.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty