Innovative Ways of Treating Diabetic Peripheral Neuropathy in the United States: A Narrative Review
Diabetes is a prevalent disease in the United States with severe, life changing and costly complications. One such complication is peripheral neuropathy which manifests itself as a chronic pain and decreased sensation. The exact mechanism of its development is not completely understood; however, it has been determined that a prolonged state of hyperglycemia leads to oxidative and nitrosative stress to the nerve fibers, edema, inflammation, demyelination and ischemia. The current approach to treatment of diabetic neuropathy focuses on three main aspects: glycemic control, lifestyle modifications and management of neuropathic pain. Because the management of neuropathic pain has varied success among different patients and does not address the underlying pathophysiology of nerve damage, novel technologies and treatment techniques are being developed. Among those are the hyperbaric oxygen therapy and angiogenesis stimulating agents. Animal studies produced impressive results, such as enhanced angiogenesis, decreased inflammation and nerve regeneration. Human trials are also being conducted, and those technologies might be the next big step in the treatment of patients with diabetic peripheral neuropathy.
Introduction
According to The Center for Disease Control and Prevention (CDC), 28.7 million Americans - 8.7% of the total US population - have diabetes mellitus in 2019 [1]. One of the most common and debilitating complications of diabetes is peripheral neuropathy that afflicts between 6% and 51% of adults depending on age, glucose control, duration and type of the disease [2]. Diabetic peripheral neuropathy contributes significantly to patient morbidity causing chronic pain, impaired sensation, increased falls and restrictions in activities of daily living. Other more serious complications include development of foot ulcers, severe infections and lower limb amputations [2]. Additionally, diabetic peripheral neuropathy is a significant financial burden on the US healthcare system, costing between $4.6 and $13.7 billion annually [3]. None of the current treatment options cure the neuropathy, and some have serious side effects. Fortunately, several promising innovations may transform the treatment of this disease.
Pathophysiology of Diabetic Neuropathy
Polyol Pathway
Even though the exact mechanism of peripheral nerve injury still eludes scientists, studies have discovered several factors that contribute to the development of diabetic neuropathy. The pathophysiology of diabetic neuropathy revolves around the polyol pathway. It is a two-step process during which glucose is reduced to sorbitol, which in turn is oxidized to fructose. The first step is catalyzed by the enzyme aldose reductase in the presence of cofactor nicotinamide adenine dinucleotide phosphate (NADPH). The second step is facilitated by the enzyme sorbitol dehydrogenase and requires nicotinamide adenine dinucleotide (NAD+) as a cofactor. Hyperactivity of the polyol pathway alters cell’s normal biochemistry, resulting in the following changes: alteration of the redox state, disruption of the sodium- potassium pump and formation of advanced glycation end products (AGEs) [4, 5].
Alteration of the Redox State
Hyperactivity of the polyol pathway results in excessive consumption of NADPH and NAD+ for production of NADP+ and NADH cofactors, respectively, which leads to a chain of metabolic imbalances. NADPH, for instance, is needed to convert glutathione disulfide (GSSH) into glutathione (GSH) by glutathione reductase. Glutathione plays an important role in preventing oxidative stress in human cells by converting hydrogen peroxide (H2O2) - a dangerous reactive oxygen species (ROS) - into water (H2O) [6]. NADPH is also used by nitric oxide synthase to produce nitric oxide (NO) from arginine. NO is a signaling molecule that causes vasodilation [7]. NADH and NADPH are substrates for an enzyme NADPH oxidase to produce superoxide anions - free radical species - that contribute to the oxidative and nitrosative stress [8, 9]. NAD+ is needed to synthesize taurine - a sulfur-containing amino acid - that works as an antioxidant, calcium modulator and neurotransmitter in the Schwann cells [10]. As the result of the altered redox state, peripheral nerves suffer oxidative and nitrosative stress due to accumulation of reactive oxygen species, nitrogen species and depletion of antioxidants. In addition, vasoconstriction of the arterioles that nourish peripheral nerves leads to their ischemia [4, 5].
Disruption of the Sodium-Potassium Pump
Glucose at high concentration inhibits the sodium- dependent transport system for myo-inositol in peripheral nerves, leading to depletion of this molecule in the cells [11, 12, 13]. Myo-inositol is an important component of phosphatidylinositol, which is a component of phosphatidylinositol 4,5-bisphosphate (PIP2). PIP2, being the crucial molecule of the IP3/DAG signaling system, is then split into inositol 1,4,5-triphosphate (IP3) and diacylglycerol (DAG), which translocate intracellular calcium and stimulate protein kinase C, respectively [14, 15]. Protein kinase C modulates activity of the sodium-potassium pump. Decrease in Na+-K+-ATPase activity leads to intracellular Na+ accumulation, decrease in Na+ permeability, increase in K+ permeability and cell edema, which in turn impedes action potential propagation, nerve demyelination and decreases nerve conduction [16].
Formation of Advanced Glycation End Products
The final product of the polyol pathway is fructose. At high concentrations both glucose and fructose can non- enzymatically bind with proteins, lipids and nucleic acids, the process called glycation or Maillard reaction, forming advanced glycation end products (AGE) [17]. There are several mechanisms by which AGE accumulation leads to cellular dysfunction. Firstly, AGE can bind with collagen fibers of the endothelial cells of the vasa nervorum, causing loss of elasticity and thickening of the capillary basement membrane, leading to endoneural microangiopathy [18, 19]. Secondly, AGE can deposit in the peripheral nerve tissues and Schwann sells which disrupts their functions, causes cell death and leads to nerve demyelination [20]. Thirdly, AGE can bind with multiple cell-surface-expressed AGE receptors (RAGE), activating several signaling pathways in the cells: Janus kinase (JAK2)-signal transducer and activator of transcription (STAT1) pathway, phosphoinositide-3- kinase (PI3K)-protein kinase B (PKB, or Akt) pathway, mitogen‑activated protein kinase (MAPK)-extracellular signal‑regulated kinase (ERK) pathway and NADPH oxidase- ROS pathway. Activation of the aforementioned pathways results in the production of proinflammatory and profibrotic cytokines, growth factors and oxidative and nitrosative stress [17, 21, 22, 23]. All this causes cell damage, inflammation, fibrosis and death, which ultimately leads to neuronal impairment. Complete pathophysiology of diabetic peripheral neuropathy is summarized in Figure 1.
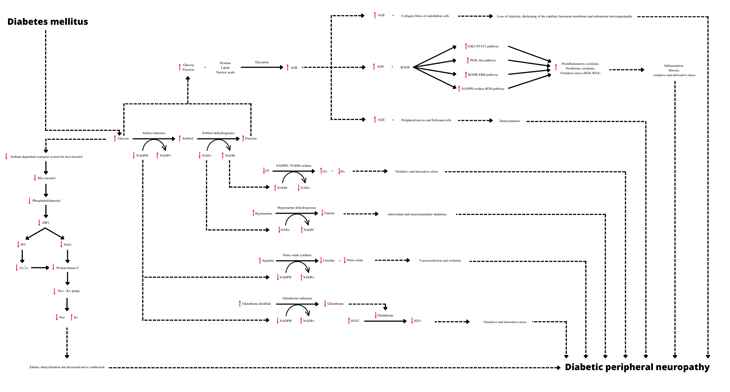
AGE: advanced glycation end products; RAGE: AGE receptors; NAD+ or NADH+: nicotinamide adenine dinucleotide; NADP or NADPH: nicotinamide adenine dinucleotide phosphate; ROS: reactive oxygen species; RNS: reactive nitrogen species; O2: oxygen; O2-: oxygen superoxide anion; H : hydrogen cation; H2O2: hydrogen peroxide; H2O: water; PIP2: phosphatidylinositol 4,5-bisphosphate; IP3: inositol 1,4,5-triphosphate; DAG: diacylglycerol; JAK2: Janus kinase; STAT1: signal transducer and activator of transcription; PI3K: phosphoinositide-3-kinase; Akt or PKB: protein kinase B; MAPK: mitogen‑activated protein kinase; ERK: extracellular signal‑regulated kinase Figure 1: Pathophysiology of diabetic peripheral neuropathy.
Current Treatment
The current approach to treatment of diabetic neuropathy focuses on three main aspects: glycemic control, lifestyle modifications and management of neuropathic pain [24].
Glycemic Control
Since the defining feature of diabetes is high blood glucose level, tight glycemic control is of paramount importance to the success of the treatment. Glycosylated hemoglobin - also known as hemoglobin A1c (HbA1c) - estimates the average blood glucose level over the past three months, and is currently the standard way to measure patient’s glycemic control as well as to calculate the risk for complications [25].
Lifestyle Modifications
The purpose of lifestyle modifications for a diabetic patient is to develop good and healthy habits and to eliminate bad and damaging ones, thus reducing the risk for potential complications as well as helping the body to repair and heal itself. Nutrition, physical activity, weight loss and cessation of damaging substances are main components of lifestyle modifications.
Nutrition: Balanced diet is important for maintaining normal blood glucose level, and thus essential in management of diabetes. Eating more non-starchy vegetables (e.g., green beans, spinach and broccoli), consuming less added sugars and refined grains (e.g., pasta, white bread and rice), focusing on whole foods instead of processed ones (e.g., canned fruits and vegetables, luncheon meals and cookies), and having smaller portions at higher frequencies are the principal aspects of a healthy diet [26]. Vitamins and supplements may also be added to the diet for additional benefit. For example, several studies have observed some improvements of neuropathic symptoms in diabetic patients with the use of alpha-lipoic acid (ALA) - an antioxidant [27, 28]. However, United States Food and Drug Administration (U.S. FDA) does not yet support the use of this drug for the treatment of diabetic neuropathy. Thiamine and its synthetic derivative benfotiamine is another example of a promising safe and cheap supplement to treat neuropathic symptoms in diabetic patients. Even though beneficial effects of thiamine in treating diabetic microangiopathy have been shown since 1996 [29, 30], more recent studies have failed to show significant improvements in peripheral nerve function [31]. Because the evidence is currently inconclusive, benfotiamine is not considered to be the standard therapy for treating diabetic neuropathy. In conclusion, proper nutrition could be summarized in the following statement: consuming the right sugars, proteins, fats, vitamins, minerals and trace elements in the right amounts at the right times. Physical Activity: Another key component of diabetes management is exercise. Multiple studies have highlighted several beneficial effects of physical activity on the body, such as increased sensitivity to insulin [32, 33, 34, 35]. Induction of antioxidant defense systems Golbidi S, et al. [36], reduction in inflammatory markers, production of anti-inflammatory compounds and interleukins [37]. Improvement of neuropathic symptoms and even regeneration of peripheral nerves and increased nerve sensitivity [38, 39]. Weight loss: The third major aspect of a successful diabetes treatment is weight loss. Obesity has become a worldwide epidemic WHO [40], and excess fat deposition throughout the body has been directly linked with hyperinsulinemia and development of diabetes mellitus type 2 [41]. In particular, it has been shown that visceral fat is metabolically active and produces a range of adipose-specific cytokines as well as pro-inflammatory cytokines that contribute to insulin resistance [42]. This is why strategic use of weight loss in diabetic patients has been recommended by The American Diabetes Association (ADA), The American Association of Clinical Endocrinologists (AACE) and The American College of Endocrinology (ACE) [43, 44]. Cessation of Damaging Substances: The final component of lifestyle modifications that assists in the treatment of diabetic peripheral neuropathy is elimination of substances that are damaging to vascular and neuronal tissues. It has been confirmed by multiple studies that smoking, for example, causes the development of both macro and microvascular complications as well as directly damages insulin producing cells of the pancreas by increasing inflammatory and oxidative stress to the tissues [45]. Excessive consumption of alcohol also induces oxidative stress in the vasculature by increasing production of free radicals as well as making the cells more susceptible to other stressors [46]. Illicit drugs, such as cocaine, have also been shown to exhibit vascular toxicity by causing profound vasoconstriction, endothelial damage, blood clot formation and elevation of pro-inflammatory cytokines [47]. As mentioned earlier, prolonged hyperglycemia causes damage to the blood vessels and peripheral nerves, so cessation of substances that negatively affect the same tissues would make sense for the management of the diabetic peripheral neuropathy.
Management of Neuropathic Pain
Neuropathic pain is one of the most common complications of diabetes. Pain management in such situations is quite challenging, however, there is a general agreement regarding the best pharmacological approach. First-Line Medications: The following three drug classes are recommended as the first-line therapy: anticonvulsants, serotonin and norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs) [24, 48].
Anticonvulsants, such as Gabapentin or Pregabalin, work by selectively inhibiting voltage-gated Ca++ channels containing the alpha-2-delta-2 subunit, decreasing the synaptic release of several neurotransmitters and, as a result, interfering with pain signal transmission [49, 50]. As the name suggests, serotonin and norepinephrine reuptake inhibitors, such as Duloxetine or Venlafaxine, work by inhibiting reuptake of serotonin and norepinephrine, leading to increased concentrations of those neurotransmitters in the synaptic cleft. Norepinephrine exhibits analgesic effect by binding with alpha-2-adrenergic receptors in the dorsal horns of the spinal cord. Those receptors are coupled with the inhibitory G protein, which inhibits voltage-gated Ca++ channels in the presynaptic membrane. This impedes the flow of Ca++ through the membrane, which inhibits the release of excitatory neurotransmitters into the synaptic cleft [51]. Tricyclic antidepressants, such as Amitriptyline, act by blocking reuptake of norepinephrine and serotonin by the presynaptic terminal, leading to accumulation of these neurotransmitters in the synaptic cleft [52]. As described earlier, norepinephrine accumulation leads to analgesic effect in the spinal cord. Second-Line Medications: The only medication that is recommended as a second-line for management of neuropathic pain is Tramadol. Tramadol is a selective agonist of opioid mu receptors, activation of which in the midbrain leads to formation of descending inhibitory impulses to the pain carrying neurons of the dorsal horns. Tramadol also inhibits reuptake of serotonin and norepinephrine just like SNRIs or TCAs [53, 54]. Third-Line Medications: Third-line treatments are reserved for patients who were not able to achieve adequate pain control with more conventional medications, and are primarily comprised of strong opioids, anticonvulsants other than gabapentinoids and cannabinoids. Analgesic effects of strong opioids, such as Morphine and Oxycodone, is achieved through stimulation of mu receptors in the central nervous system54. Cannabinoids, such as Nabiximol, work by stimulating cannabinoid receptors type 1 (CB1) and type 2 (CB2). Activation of the CB1 receptors at the presynaptic terminal results in inhibited of the voltage-gated Ca++ channels, which subsequently leads to decreased release of neurotransmitters and inhibition of pain transmission [55]. Additional Approaches: Some patients may require more special approaches to pain management. However, those treatment methods have various degrees of success among patients. Carbamazepine, for example, is used for trigeminal neuralgia. It works by blocking voltage-gated Na+ channels, which leads to inhibition of action potential and decreased propagation of pain signals [56]. Localized neuropathic pain could be treated by topical agents, such as Lidocaine or Capsaicin, or by subcutaneous injections of botulinum toxin.
Just like Carbamazepine, Lidocaine exhibits its analgesic effect by blocking voltage-gated Na+ channels [57]. Capsaicin, on the other hand, works as an agonist to the transient receptor potential vanilloid 1 (TRPV 1), which serves as a transmembrane Ca++ channel. Capsaicin also binds with receptors at the endoplasmic reticulum, allowing Ca++ to flow into the cytoplasm. Increased concentration of Ca++ in the cytoplasm inactivates Na+ channels, interfering with action potential propagation, reducing neuronal responsiveness and muting the pain stimuli in the short term. Excess Ca++ also activates proteases, which cause the breakdown of cytoskeleton, interrupting fast axonal transport of neurotransmitters and contributing to an anesthetic effect in the medium term. At higher concentrations capsaicin directly inhibits electron transport chain by competing with one of its important components - ubiquinone. Due to mitochondrial damage proper metabolism cannot be maintained in the nerve endings of the skin where capsaicin has been applied, leading to nerve fiber retraction. This is the mechanism of the long term pain relief [58].
Botulinum toxin is a neurotoxin that works by blocking presynaptic release of acetylcholine at the neuromuscular junction, causing temporary muscle paralysis. Its pain modulating effect is not well understood, however, it is hypothesized that it comes from impairing the release of substance P, glutamate, calcitonin gene-related peptide, somatostatin, serotonin, ATP and bradykinin [59, 60].
Another approach to management of neuropathic pain is the use of transcutaneous electrical nerve stimulation (TENS). This procedure works by placing small electrodes on the skin and passing electrical impulses through them. This stimulates large diameter A-beta sensory afferent nerve fibers, which leads to inhibition of small pain fibers of the same dermatome by stimulation of gamma-aminobutyric acid (GABA) and opioid receptors in the dorsal horns of the spinal cord, preventing the pain signals from reaching the brain [61, 62].
Recently, pain management providers have become more adept at injecting specific nerve tracts to provide pain relief. These treatments have included steroids Wong F, et al. [63], analgesics and sclerosing agents64 to affect the nerve. There has been varying degrees of success with these techniques, and many diabetic patients have not had the same results as non-diabetic patients with these interventions [65, 66].
New Frontiers
As discussed earlier, prolonged state of hyperglycemia causes nerve fibers to suffer oxidative and nitrosative stress, edema, inflammation, demyelination and ischemia, resulting in diabetic peripheral neuropathy. Tapping into the very physiology that causes such a debilitating complication of diabetes, several new treatment methods have been developing over the past several years that strive to not only slow down the progression of the neuropathy but to reverse it.
Hyperbaric Oxygen Therapy
The first treatment method is the use of hyperbaric oxygen therapy (HBO). HBO has been used for many generations as a treatment for arterial gas embolism, severe carbon monoxide poisoning, smoke inhalation and decompression sickness in divers and pilots [67]. The patient is placed in a chamber which is pressurized using 100% O2. This increases plasma oxygen concentration twenty-fold, raising tissue- cellular diffusion gradient, which improves cellular oxygen supply [67]. Tissue hyperoxia stimulates collagen matrix formation, which is essential for angiogenesis and wound healing [67]. Excess O2 causes arteriolar vasoconstriction, which decreases tissue edema without causing hypoxia [68]. Increased partial pressure of O2 in the tissues also leads to reduction of inflammatory mediators and cytokines [69]. HBO has been the standard of care for patients with diabetic foot ulcers, and has prevented amputations in many of these patients [70, 71, 72]. After the treatment, many patients have also reported an improvement in their sensations. Those results have not been all positive however, as some have noted an increased pain in the wound [73]. Those findings could be due to enhanced angiogenesis stimulated by the treatment or could be a direct effect of the treatment on the pathological nerves in the region. Further research is necessary to elucidate the effectiveness of this treatment on diabetic neuropathy.
Angiogenesis Stimulating Agents
As mentioned, nerve ischemia is one the major reasons for diabetic peripheral neuropathy. In an attempt to slow down progression of this process and reverse nerve damage new cutting-edge technologies that promote angiogenesis have been developing. Bone Marrow-Derived Cells: One of those potential therapies focuses on the use of bone marrow-derived mononuclear and endothelial progenitor cells. Those cells contain angiogenic and neurotrophic cytokines that promote neural neovascularization [74]. Vascular endothelial growth factor (VEGF) is one of the main angiogenic cytokines that promotes proliferation and migration of endothelial cells in the ischemic tissues [75]. It also enhances Schwann cell proliferation and migration Schratzberger P, et al. [76], and facilitates axonal outgrowth [77]. Insulin-like growth factor (IGF) promotes blood vessel remodeling [78], nerve regeneration [79, 80]. Schwann cell mitogenesis and myelination [81]. Nerve growth factor (NGF) induces angiogenesis [82], and also has neuroprotective and repair functions [83]. A study, published in 2009, was successfully able to demonstrate increased capillary density and blood supply in the nerves of diabetic mice [84]. Clinical trials are being conducted in order to determine if similar effects could be achieved in humans. Human Amniotic Fluid Derived Cells: Another novel approach to the treatment of diabetic neuropathy is the use of human amniotic fluid derived mesenchymal stem cells (hAFMSCs) [85]. Those cells express features of both mesenchymal and neural stem cells, secrete various neurotrophic factors [86, 87], modulate inflammatory processes Pan HC, et al. [88], and are able to cause peripheral nerve regeneration. Animal studies were successful in showing nerve regeneration in diabetic mice Chiang CY, et al. [85], and human trials are under way. Human Placenta and Placental Derivatives: The third possible path to treat diabetic neuropathy revolves around the use of human placenta and placental derivatives [89]. Placental extracts, for example, contain cells that express VEGF - a potent growth factor - functions of which were discussed earlier. Several studies have demonstrated their positive effect on the nerve regeneration in mice [90]. Clinical trials are currently being conducted to determine their usefulness in treating diabetic neuropathy in humans.
Conclusion
Peripheral neuropathy is a debilitating complication of diabetes that affects many patients, and it manifests itself in chronic pain and loss of sensations. Current treatment approaches primarily focus on pain management aspect with various degrees of success. Over the years, however, our understanding of the mechanisms underlying the development of diabetic neuropathy has advanced. Based on this knowledge, new treatment techniques and approaches have been developing that aim to address one of the primary causes of diabetic neuropathy - nerve ischemia. On the cutting edge of this development are such techniques as hyperbaric oxygen therapy and angiogenesis stimulating agents that aim not only to slow down the progression of nerve degeneration, but to facilitate its regeneration. While those techniques are still in their infancy, they have already showed promising results, and represent a major step in the treatment of patients with diabetic neuropathy.
References
-
CDC (2022) Prevalence of Diagnosed Diabetes. Diabetes. Centers for Disease control and Prevention.
-
Hicks CW, Selvin E (2019) Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr Diab Rep 19(10): 86.
-
Gordois A, Scuffham P, Shearer A, Oglesby A, Tobian JA (2003) The health care costs of diabetic peripheral neuropathy in the US. Diabetes Care 26(6): 1790-1795.
-
Yagihashi S, Mizukami H, Sugimoto K (2011) Mechanism of diabetic neuropathy: Where are we now and where to go? J Diabetes Investig 2(1): 18-32.
-
Niimi N, Yako H, Takaku S, Chung SK, Sango K (2021) Aldose Reductase and the Polyol Pathway in Schwann Cells: Old and New Problems. Int J Mol Sci 22(3): 1031.
-
Couto N, Wood J, Barber J (2016) The role of glutathione reductase and related enzymes on cellular redox homoeostasis network. Free Radic Biol Med 95: 27-42.
-
Forstermann U, Sessa WC (2012) Nitric oxide synthases: regulation and function. Eur Heart J 33(7): 829-837.
-
Tarafdar A, Pula G (2018) The Role of NADPH Oxidases and Oxidative Stress in Neurodegenerative Disorders. Int J Mol Sci 19(12): 3824.
-
Torres IP, Pech LM, Ruiz MER, Soto ME, Lans VG (2020) Nitrosative Stress and Its Association with Cardiometabolic Disorders. Molecules 25(11): 2555.
-
Askwith T, Zeng W, Eggo MC, Stevens MJ (2012) Taurine reduces nitrosative stress and nitric oxide synthase expression in high glucose-exposed human Schwann cells. Exp Neurol 233(1): 154-162.
-
Barrese V, Stott JB, Baldwin SN, Parreno GM, Greenwood IA (2020) SMIT (Sodium-Myo-Inositol Transporter) 1 Regulates Arterial Contractility Through the Modulation of Vascular Kv7 Channels. Arterioscler Thromb Vasc Biol 40(10): 2468-2480.
-
Greene DA, Lattimer SA (1982) Sodium- and energy- dependent uptake of myo-inositol by rabbit peripheral nerve. Competitive inhibition by glucose and lack of an insulin effect. J Clin Invest 70(5): 1009-1018.
-
Gillon KR, Hawthorne JN (1983) Transport of myo- inositol into endoneurial preparations of sciatic nerve from normal and streptozotocin-diabetic rats. Biochem J 210(3): 775-781.
-
Foskett JK, White C, Cheung KH, Mak DOD (2007) Inositol Trisphosphate Receptor Ca2+ Release Channels. Physiol Rev 87(2): 593-658.
-
Berridge MJ (1993) Inositol trisphosphate and calcium signalling. Nature 361(6410): 315-325.
-
Greene DA, Lattimer SA, Sima AA (1988) Are disturbances of sorbitol, phosphoinositide, and Na+-K+- ATPase regulation involved in pathogenesis of diabetic neuropathy? Diabetes 37(6): 688-693.
-
Shen CY, Lu CH, Wu CH, Li KJ, Kuo YM, et al. (2020) The Development of Maillard Reaction, and Advanced Glycation End Product (AGE)-Receptor for AGE (RAGE) Signaling Inhibitors as Novel Therapeutic Strategies for Patients with AGE-Related Diseases. Molecules 25(23): 5591.
-
Dyer DG, Dunn JA, Thorpe SR, Bailie KE, Lyons TJ, et al. (1993) Accumulation of Maillard reaction products in skin collagen in diabetes and aging. J Clin Invest 91(6): 2463-2469.
-
Kent MJ, Light ND, Bailey AJ (1985) Evidence for glucose- mediated covalent cross-linking of collagen after glycosylation in vitro. Biochem J 225(3): 745-752.
-
Sugimoto K, Yasujima M, Yagihashi S (2008) Role of advanced glycation end products in diabetic neuropathy. Curr Pharm Des 14(10): 953-961.
-
Ott C, Jacobs K, Haucke E, Santos AN, Grune T, et al. (2014) Role of advanced glycation end products in cellular signaling. Redox Biol 2: 411-429.
-
Sorci G, Riuzzi F, Giambanco I, Donato R (2013) RAGE in tissue homeostasis, repair and regeneration. Biochim Biophys Acta 1833(1): 101-109.
-
Sanajou D, Haghjo AG, Argani H, Aslani S (2018) AGE- RAGE axis blockade in diabetic nephropathy: Current status and future directions. Eur J Pharmacol 833: 158- 164.
-
Feldman EL, Callaghan BC, Busui RP, Zochodne DW, Wright DE, et al. (2019) Diabetic neuropathy. Nat Rev Dis Primer 5(1): 42.
-
CDC (2018) All About Your A1C. Diabetes. Centers for Disease Control and Prevention.
-
CDC (2021) Meal Planning. Diabetes. Centers for Disease Control and Prevention.
-
Ziegler D, Hanefeld M, Ruhnau KJ, Hasche H, Lobisch M, et al. (1999) Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a 7-month multicenter randomized controlled trial (ALADIN III Study). ALADIN III Study Group. Alpha- Lipoic Acid in Diabetic Neuropathy. Diabetes Care 22(8): 1296-1301.
-
Ziegler D, Ametov A, Barinov A, Dyck PJ, Gurieva I, et al. (2006) Oral treatment with alpha-lipoic acid improves symptomatic diabetic polyneuropathy: the SYDNEY 2 trial. Diabetes Care 29(11): 2365-2370.
-
Stracke H, Lindemann A, Federlin K (1996) A benfotiamine-vitamin B combination in treatment of diabetic polyneuropathy. Exp Clin Endocrinol Diabetes Off J Ger Soc Endocrinol Ger Diabetes Assoc 104(4): 311- 316.
-
La Selva M, Beltramo E, Pagnozzi F, Bena E, Molinatti PA, et al. (1996) Thiamine corrects delayed replication and decreases production of lactate and advanced glycation end-products in bovine retinal and human umbilical vein endothelial cells cultured under high glucose conditions. Diabetologia 39(11): 1263-1268.
-
Fraser DA, Diep LM, Hovden IA, Nilsen KB, Sveen KA, et al. (2012) The Effects of Long-Term Oral Benfotiamine Supplementation on Peripheral Nerve Function and Inflammatory Markers in Patients With Type 1 Diabetes. Diabetes Care 35(5): 1095-1097.
-
McClatchey PM, Williams IM, Xu Z, Mignemi NA, Hughey CC, et al. (2019) Perfusion controls muscle glucose uptake by altering the rate of glucose dispersion in vivo. Am J Physiol - Endocrinol Metab 317(6): E1022-E1036.
-
Cartee GD (2015) Mechanisms for greater insulin- stimulated glucose uptake in normal and insulin- resistant skeletal muscle after acute exercise. Am J Physiol Endocrinol Metab 309(12): E949-E959.
-
McGarrah RW, Slentz CA, Kraus WE (2016) The Effect of Vigorous- Versus Moderate-Intensity Aerobic Exercise on Insulin Action. Curr Cardiol Rep 18(12): 117.
-
Way KL, Hackett DA, Baker MK, Johnson NA (2016) The Effect of Regular Exercise on Insulin Sensitivity in Type 2 Diabetes Mellitus: A Systematic Review and Meta- Analysis. Diabetes Metab J 40(4): 253-271.
-
Golbidi S, Badran M, Laher I (2012) Antioxidant and Anti- Inflammatory Effects of Exercise in Diabetic Patients. Exp Diabetes Res 2012: 941868.
-
Kasapis C, Thompson PD (2005) The effects of physical activity on serum C-reactive protein and inflammatory markers: a systematic review. J Am Coll Cardiol 45(10): 1563-1569.
-
Kluding PM, Pasnoor M, Singh R, Jernigan S, Farmer K, et al. (2012) The Effect of Exercise on Neuropathic Symptoms, Nerve Function, and Cutaneous Innervation in People with Diabetic Peripheral Neuropathy. J Diabetes Complications 26(5): 424-429.
-
Singleton JR, Marcus RL, Lessard M, Jackson JE, Smith AG (2015) Supervised exercise improves cutaneous reinnervation capacity in metabolic syndrome patients. Ann Neurol 77(1): 146-153.
-
WHO (2021) Obesity and overweight. World Health Organization.
-
Langenberg C, Sharp SJ, Schulze MB, Rolandsson O, Overvad K, et al. (2012)Long-Term Risk of Incident Type 2 Diabetes and Measures of Overall and Regional Obesity: The EPIC-InterAct Case-Cohort Study. PLoS Med 9(6): e1001230.
-
Fang L, Guo F, Zhou L, Stahl R, Grams J (2015) The cell size and distribution of adipocytes from subcutaneous and visceral fat is associated with type 2 diabetes mellitus in humans. Adipocyte 4(4): 273-279.
-
Davies MJ, DAlessio DA, Fradkin J, Kernan WN, Mathieu C, et al. (2018) Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 41(12): 2669-2701.
-
Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, et al. (2018) Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm - 2018 Executive Summary. Endocr Pract Off J Am Coll Endocrinol Am Assoc Clin Endocrinol 24(1): 91-120.
-
Mosson MS, Milnerowicz H (2017) The impact of smoking on the development of diabetes and its complications. Diab Vasc Dis Res 14(4): 265-276.
-
Phillips SA, Osborn K, Hwang CL, Sabbahi A, Piano MR (2019) Ethanol induced oxidative stress in the vasculature: Friend or Foe. Curr Hypertens Rev 16(3): 181-191.
-
Bachi K, Mani V, Jeyachandran D, Fayad ZA, Goldstein RZ, et al. (2017) Vascular disease in cocaine addiction. Atherosclerosis 262: 154-162.
-
Rosenberger DC, Blechschmidt V, Timmerman H, Wolff A, Treede RD (2020) Challenges of neuropathic pain: focus on diabetic neuropathy. J Neural Transm 127(4): 589-624.
-
Sills GJ (2006) The mechanisms of action of gabapentin and pregabalin. Curr Opin Pharmacol 6(1): 108-113.
-
Taylor CP, Angelotti T, Fauman E (2007) Pharmacology and mechanism of action of pregabalin: the calcium channel alpha2-delta (alpha2-delta) subunit as a target for antiepileptic drug discovery. Epilepsy Res 73(2): 137-150.
-
Obata H (2017) Analgesic Mechanisms of Antidepressants for Neuropathic Pain. Int J Mol Sci 18(11): 2483.
-
Moraczewski J, Aedma KK (2022) Tricyclic Antidepressants. StatPearls.
-
Dayer P, Desmeules J, Collart L (1997) Pharmacology of tramadol. Drugs 53(2): 18-24.
-
Dhaliwal A, Gupta M (2021) Physiology, Opioid Receptor. StatPearls.
-
Sheikh NK, Dua A (2022) Cannabinoids. StatPearls.
-
Maan JS, Duong T vi H, Saadabadi A (2022) Carbamazepine. StatPearls.
-
Yang X, Wei X, Mu Y, Li Q, Liu J (2020) A review of the mechanism of the central analgesic effect of lidocaine. Medicine (Baltimore) 99(17): e19898.
-
Anand P, Bley K (2011) Topical capsaicin for pain management: therapeutic potential and mechanisms of action of the new high-concentration capsaicin 8% patch. BJA Br J Anaesth 107(4): 490-502.
-
Lagueny A, Burbaud P (1996) Mechanism of action, clinical indication and results of treatment of botulinum toxin. Neurophysiol Clin Clin Neurophysiol 26(4): 216- 226.
-
Kumar R (2018) Therapeutic use of botulinum toxin in pain treatment. Neuronal Signal 2(3): NS20180058.
-
Johnson M (2007) Transcutaneous Electrical Nerve Stimulation: Mechanisms, Clinical Application and Evidence. Rev Pain 1(1): 7-11.
-
Melzack R, Wall PD (1965) Pain mechanisms: a new theory. Science 150(3699): 971-979.
-
Wong F, Namdari B, Dupler S, Kovac MF, Makarova N, et al. (2016) No difference in pain reduction after epidural steroid injections in diabetic versus nondiabetic patients: A retrospective cohort study. J Anaesthesiol Clin Pharmacol 32(1): 84-88.
-
Publishing L, Guiboles (2013) Sclerotherapy in the patient with diabetes: indications and results. Servier - Phlebolymphology.
-
Baeriswyl M, Taffe P, Kirkham KR, Bathory I, Rancati V, et al. (2018) Comparison of peripheral nerve blockade characteristics between non-diabetic patients and patients suffering from diabetic neuropathy: a prospective cohort study. Anaesthesia 73(9): 1110-1117.
-
Prasad GVK (2019) Peripheral Nerve Blocks in Patients with Diabetic Neuropathy and other Neuropathies: A Narrative Review. Int J Contemp Med Res IJCMR 6(10): 1-6.
-
Leach RM, Rees PJ, Wilmshurst P (1998) Hyperbaric oxygen therapy. BMJ 317(7166): 1140-1143.
-
Nylander G, Lewis D, Nordstrom H, Larsson J (1985) Reduction of postischemic edema with hyperbaric oxygen. Plast Reconstr Surg 76(4): 596-603.
-
Schiavo S, DeBacker J, Djaiani C, Bhatia A, Englesakis M, et al. (2021) Mechanistic Rationale and Clinical Efficacy of Hyperbaric Oxygen Therapy in Chronic Neuropathic Pain: An Evidence-Based Narrative Review. Pain Res Manag 2021: 8817504.
-
Liu R, Li L, Yang M, Boden G, Yang G (2013) Systematic review of the effectiveness of hyperbaric oxygenation therapy in the management of chronic diabetic foot ulcers. Mayo Clin Proc 88(2): 166-175.
-
Stoekenbroek RM, Santema TB, Legemate DA, Ubbink DT, Brink AVD, et al. (2014) Hyperbaric oxygen for the treatment of diabetic foot ulcers: a systematic review. Eur J Vasc Endovasc Surg Off J Eur Soc Vasc Surg 47(6): 647-655.
-
Wiedmann IR, Bennett M, Kranke P (2005) Systematic review of hyperbaric oxygen in the management of chronic wounds. Br J Surg 92(1): 24-32.
-
Heyboer M, Sharma D, Santiago W, McCulloch N (2017) Hyperbaric Oxygen Therapy: Side Effects Defined and Quantified. Adv Wound Care 6(6): 210-224.
-
Kim H, Kim JJ, Yoon YS (2012) Emerging Therapy for Diabetic Neuropathy: Cell Therapy Targeting Vessels and Nerves. Endocr Metab Immune Disord Drug Targets 12(2): 168-178.
-
Shweiki D, Itin A, Soffer D, Keshet E (1992) Vascular endothelial growth factor induced by hypoxia may mediate hypoxia-initiated angiogenesis. Nature 359(6398): 843-845.
-
Schratzberger P, Schratzberger G, Silver M, Curry C, Kearney M, et al. (2000) Favorable effect of VEGF gene transfer on ischemic peripheral neuropathy. Nat Med 6(4): 405-413.
-
Sondell M, Lundborg G, Kanje M (1999) Vascular endothelial growth factor stimulates Schwann cell invasion and neovascularization of acellular nerve grafts. Brain Res 846(2): 219-228.
-
Lopez CL, LeRoith D, Aleman IT (2004) Insulin-like growth factor I is required for vessel remodeling in the adult brain. Proc Natl Acad Sci USA 101(26): 9833-9838.
-
Near SL, Whalen LR, Miller JA, Ishii DN (1992) Insulin-like growth factor II stimulates motor nerve regeneration. Proc Natl Acad Sci USA 89(24): 11716-11720.
-
Fernyhough P, Willars GB, Lindsay RM, Tomlinson DR (1993) Insulin and insulin-like growth factor I enhance regeneration in cultured adult rat sensory neurones. Brain Res 607(1-2): 117-124.
-
Cheng HL, Russell JW, Feldman EL (1999) IGF-I promotes peripheral nervous system myelination. Ann N Y Acad Sci 883: 124-130.
-
Graiani G, Emanueli C, Desortes E, Linthout SV, Pinna A, et al. (2004) Nerve growth factor promotes reparative angiogenesis and inhibits endothelial apoptosis in cutaneous wounds of Type 1 diabetic mice. Diabetologia 47(6): 1047-1054.
-
Sofroniew MV, Howe CL, Mobley WC (2001) Nerve growth factor signaling, neuroprotection, and neural repair. Annu Rev Neurosci 24: 1217-1281.
-
Jeong JO, Kim MO, Kim H, Lee MY, Kim AW, et al. (2009) Dual Angiogenic and Neurotrophic Effects of Bone Marrow-Derived Endothelial Progenitor Cells on Diabetic Neuropathy. Circulation 119(5): 699-708.
-
Chiang CY, Liu SA, Sheu ML, Chen FC, Chen CJ, et al. (2016) Feasibility of Human Amniotic Fluid Derived Stem Cells in Alleviation of Neuropathic Pain in Chronic Constrictive Injury Nerve Model. PLoS ONE 11(7): e0159482.
-
Pan HC, Cheng FC, Chen CJ, Lai SZ, Lee CW, et al. (2007) Post-injury regeneration in rat sciatic nerve facilitated by neurotrophic factors secreted by amniotic fluid mesenchymal stem cells. J Clin Neurosci Off J Neurosurg Soc Australas 14(11): 1089-1098.
-
Pan HC, Yang DY, Chiu YT, Lai SZ, Wang YC, et al. (2006) Enhanced regeneration in injured sciatic nerve by human amniotic mesenchymal stem cell. J Clin Neurosci Off J Neurosurg Soc Australas 13(5): 570-575.
-
Pan HC, Chen CJ, Cheng FC, Ho SP, Liu MJ, et al. (2009) Combination of G-CSF administration and human amniotic fluid mesenchymal stem cell transplantation promotes peripheral nerve regeneration. Neurochem Res 34(3): 518-527.
-
Pogozhykh O, Prokopyuk V, Figueiredo C, Pogozhykh D (2018) Placenta and Placental Derivatives in Regenerative Therapies: Experimental Studies, History, and Prospects. Stem Cells Int 2018: 4837930.
-
Park JY, Lee J, Jeong M, Min S, Kim SY, et al. (2014) Effect of Hominis Placenta on cutaneous wound healing in normal and diabetic mice. Nutr Res Pract 8(4): 404-409.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty