Impact of Diabetes Distress on Glycemic Control
Introduction: Diabetes related distress is a recent entity that was found to be associated with poor glycemic control but it was never assessed in Tunisia nor in african countries. This study aimed at exploring the relationship between diabetes related distress and glycemic control. Methods: Cross-sectional study assessing diabetes related distress (using Problem Areas in Diabetes Scale PAID-5) and treatment adherence (using Medication Adherence Questionnaire de Morisky-Green) and glycemic control using HbA1c in Tunisian patients with Type 2 diabetes. Results: There was a statistically significant association between high PAID-5 scores and poor glycemic control. A threshold of 8.5 on PAID-5 predicts poor glycemic control and complications. Conclusion: It is recommended to screen for diabetes related distress using PAID-5 in order to detect patients with high risk of poor glycemic control and complications.
Introduction
Type 2 diabetes is a widespread chronic disease and its prevalence continues to increase [1]. An increase in diabetes- related mortality is expected, especially in developing countries [1]. In Tunisia, the prevalence of type 2 diabetes was 15.1% in 2014 [2] and should reach a rate of 26.6% in 2027 [3]. To address this public health problem, studies recommend the intensification of drug treatment to prevent the complications of diabetes [4]. However, living with this chronic disease also requires adhering to a healthy lifestyle. In addition to long-term oral or injection treatments, the patient must follow a restrictive diet, regular physical activity and monitoring of blood sugar. In addition, the patient must learn to deal with the risk of possible complications. All these demands can overwhelm patients [5]. According to the American Diabetes Association, diabetes-related distress is an entity distinctive from other psychological disorders. It is a significantly negative psychological reaction linked to emotional over-strain in the process of coping with this disease [6]. A high level of diabetes-related distress is associated with poor adherence to treatment, poor adherence to physical exercise and diet [6]. This is a recent concept that was first used in Anglo-Saxon countries and is still rare in French-speaking literature. The relationship between diabetes-related distress and glycemic control has never been explored in Tunisia or other African countries. The objectives of our work were: to investigate associations between diabetes-related distress and glycemic control. -Determine the threshold of this scale significantly associated with poor glycemic control in Tunisian patients.
Methods
This was a cross-sectional study conducted between February and June 2019 in a primary care center located in the southern suburbs of the capital Tunis. The same investigator approached the patients in the waiting room and administered questionnaires in a quiet office after obtaining informed consent. Adult patients followed for type 2 diabetes for more than one year were included. The exclusion criteria were having a severe intellectual deficit or a major complication of diabetes. Diabetes-related distress was assessed using the Problem Areas in Diabetes Scale 5-items (PAID-5) questionnaire validated in Tunisia [7, 8] (Appendix 1). Adherence was studied using the Morisky- Green Medication Adherence Questionnaire (MAQR) [9] with 6 items validated in Tunisian Arabic [10]. It allows to find out if patient has good, average or bad adherence. Demographic and clinical variables were collected from the interview and the medical record. Glycemic balance was assessed using the recent glycated hemoglobin (HbA1C) value. Poor glycemic control was defined as HbA1C≥7. Data analysis was performed using SPSS version 20 software.
Results and Discussion
Descriptive study
The investigator approached 108 patients. Eight refused to participate and 100 were included. Median age was 58 [54 – 63,75] and sex-ratio was 0,5.
Demographic features
Nearly half the sample had a primary education level (48%), 22% a secondary level, 12% a higher education level and 18% have never been to school. Regarding the professional situation, only 23% had a regular job. The rest were inactive (without profession or with precarious irregular jobs in 51% of cases and retired in 26% of cases).
Clinical Features
The median duration of diabetes was 6 years (range: 1-30). Most of the patients in the study were on Oral Anti- Diabetics (OAD) (85%) and only one patient was on insulin alone (1%), the rest being on the insulin and OAD combination. Hypertension was the most frequent comorbidity (67%) followed by dyslipidemia (50%) and finally anxio-depressive history (8%). Complications were distributed as follows: retinopathy (29%), nephropathy (26%), neuropathy (19%), coronary artery disease (7%) and obliterating arteriopathy of the lower limbs (3%). Regarding glycemic control, HbA1c values had a median of 7.85 (range: 5.3-14). Most patients in our sample had poor glycemic control (68%). The results of the MAQR compliance test showed that half had a poor level of compliance (i.e. 51%), 15% a good level of compliance and 34% an average level.
Results on the PAID-5 Scale
The diabetes-specific distress assessment on the PAID 5 questionnaire showed a median PAID-5 in our sample of 10 [2.9-15.6], with extreme values from 0 to 20.
Statistical Analysis
Relationship between diabetes-related distress and demographic variables In our study, we did not find a statistically significant relationship between the level of stress related to diabetes and the age, the gender, the professional situation or the level of education of patients. Some studies have found that stress is associated with young age [11] and unfavorable economic conditions [12]. Relationship Between diabetes-related distress and clinical variables. There was a significant relationship between stress and the presence of anxiety and depression comorbidities reported by patients (p<0.05). Authors have suggested that this relationship is bidirectional. Indeed, the presence of depressive symptoms predicted the later development of diabetes-related stress, and vice versa [13, 14].
There is a positive correlation, with a significance of 0.001, between the level of stress and the duration of diabetes progression. Indeed, the longer the disease, the more the level of distress increases. This could be explained by the accumulation of degenerative complications over time or the advent of acute complications as well as the possibility of being hospitalized [15, 16, 17]. We found that the patients on insulin (with or with our OAD) had significantly higher levels of distress (median PAID- 5 to 14 against 8 in the group without insulin and p=0.013). Switching to insulin is perceived as a sign of worsening of the disease which can induce a feeling of failure and guilt. It is a more invasive act, sometimes embarrassing to do in public and also inducing an increased risk of hypoglycemia, experienced as a restriction of freedom [18, 19]. Regarding degenerative complications, there was a significantly higher stress in patients with retinopathy, coronary artery disease and neuropathy. Table 1 details the statistical association between diabetes distress and complications. This result is confirmed by several studies [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21] especially for retinopathy and neuropathy [9, 22]. The absence of association between stress and nephropathy would be due to the fact that the latter remains silent for a long time and is detected by biological assessments and only becomes symptomatic at the advanced stage of renal insufficiency. The absence of a statistically significant relationship between PAID-5 and obliterating arteritis of the lower limbs may be due to the low number of patients who reported this complication (3%) (Table 1).
| Median of PAID-5 | p | ||
|---|---|---|---|
| Retinopathy | Yes | 15 | 0,006* |
| No | 8 | ||
| Nephropathy | Yes | 13 | 0,121 |
| No | 9 | ||
| Neuropathy | Yes | 15 | 0,022* |
| No | 9 | ||
| Coronaropathy | Yes | 16 | 0,021* |
| No | 9 | ||
| Obliterating arteritis of the lower limbs | Yes | 9 | 0,864 |
| No | 10 |
Table 1: Relationship between PAID-5 diabetes related degenerative complications.
*p<0,05 Table 1: Relationship between PAID-5 diabetes related degenerative complications.
Distress level and Glycemic control
A high level of distress was associated with high level of HbA1C (r=0,473, p<0.001).
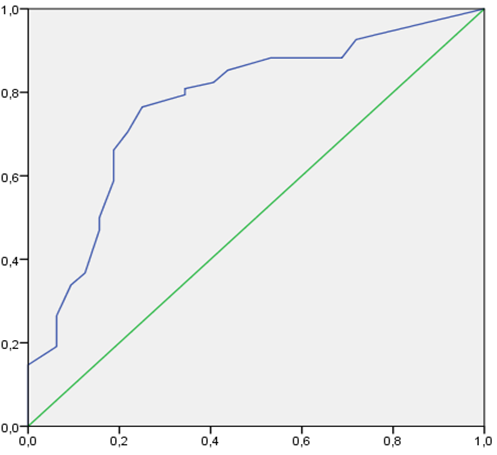
Determining Threshold of PAID-5 Associated with Poor Glycemic Control
A ROC curve (Receiver Operating Characteristics) was used to assess the ability of PAID-5 questionnaire to detect poor glycemic control. This curve allows to transform the quantitative variables into qualitative variables with two modalities. For the determination of the threshold at which to “cut” the quantitative variable, we therefore established ROC curves. After verifying that the area under the curve is significantly > 0.5, we chose as threshold the value of the variable that corresponds to the best “sensitivity-specificity” couple. The area under the curve was 0.774 [0.674 – 0.874], p<0.001 (Figure 1). At the threshold of 8.5, the sensitivity is 70.6% and the specificity is 78.1% (Table 2).
| Area under the curve | CI of 95% | p | Sensitivity | Specificity | |
|---|---|---|---|---|---|
| 8,5 | 77,4 | [0,674 – 0,874] | <0,001 | 70,6% | 78,1% |
Table 2: PAID-5 threshold.
The percentage of patients with a PAID-5 score greater than 8.5 and having uncontrolled diabetes was statistically significant (p<0.001) (Table 3). This association between stress and poor glycemic control is reported in the literature [23, 24]. Several explanations seem plausible. Indeed, a distressed patient would do fewer self-management activities and would have poor adherence to treatment [23, 25]. In other cases, having unbalanced diabetes could cause a feeling of helplessness which would increase the stress related to the disease [26].
| Poor control (N=68) | Good control | Odds Ratio | P | ||
|---|---|---|---|---|---|
| (N=32) | IC (95%) | ||||
| Diabetes related distress | Yes (N=55) | 48 (87,3%) | 7 (12,7%) | 8,57 [3,19-23] | <0,001 |
| No (N=45) | 20 (44,4%) | 25 (55,6%) |
Table 3: Association between distress and glycemic control.
Limits
First, the sample of patients who participated in our work is not necessarily representative of all patients with diabetes in Tunisia. We recruited them from a single primary care center. The sample is relatively small. The random convenience recruitment method poses another limit to the generalization of the results, but we chose it for its feasibility.
Recommendations for Primary Care Physicians
Screening for diabetes-related distress would be very useful for primary care physicians in the follow-up of patients with diabetes. It allows to detect patients who are most at risk of developing complications, to better understand their patients and to initiate dialogue about the emotional impact of the disease. Screening for this psychological distress using a validated measurement instrument such as the PAID-5 should be regular. It should be performed when the therapeutic objectives are not achieved despite adequate treatment, upon initiation of insulin therapy or when degenerative complications appear [6].
References
-
Ogurtsova K, Da Rocha Fernandes JD, Huang Y, Linnenkamp U, Guariguata L, et al. (2017) IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract 128: 40-50.
-
Ben Romdhane H, Ben Ali S, Aissi W, Traissac P, Aounallah- Skhiri H, et al. 2014 Prevalence of diabetes in Northern African countries: the case of Tunisia. BMC Public Health 14: 86.
-
Saidi O, O’Flaherty M, Mansour NB, Aissi W, Lassoued O, et al. (2015) Forecasting Tunisian type 2 diabetes prevalence to 2027: validation of a simple model. BMC Public Health 15: 104.
-
Shaoning Lv, Ross P, Tori K (2017) The optimal blood glucose level for critically ill adult patients. Nurs Crit Care 22(5): 312-319.
-
Polonsky WH, Fisher L, Earles J, Dudl RJ, Lees J, et al. (2005) Assessing psychosocial distress in diabetes: development of the diabetes distress scale. Diabetes Care 28(3): 626-631.
-
American Diabetes Association (2019) 5. Lifestyle Management: Standards of Medical Care in Diabetes-2019. Diabetes Care 42(Suppl 1): S46-S60.
-
Nicolucci A, Kovacs Burns K, Holt RI, Comaschi M, Hermanns N, et al. (2013) Diabetes Attitudes, Wishes and Needs second study (DAWN2): cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabet Med 30(7): 767-777.
-
McGuire BE, Morrison TG, Hermanns N, Skovlund S, Eldrup E, et al. (2010) Short-form measures of diabetes- related emotional distress: the Problem Areas in Diabetes Scale (PAID)-5 and PAID-1. Diabetologia 53(1): 66-69.
-
Abdelghaffar W (2020) Validation transculturelle d’un questionnaire de “stress lié au diabète” [Thèse]. Psychiatrie: Tunis.
-
Morisky DE, Green LW, Levine DM (1986) Concurrent and Predictive Validity of a Self-Reported Measure of Medication Adherence. Med Care 24(1): 67-74.
-
Hamdi S (2017) Education thérapeutique des patients diabétiques: Effet sur l’équilibre glycémique, les connaissances sur le diabète, l’observance et la qualité de vie [Thèse]. Nutrition: Tunis, pp: 58.
-
Huis In ‘t Veld EM, Makine C, Nouwen A, Karsidag C, Kadioglu P, et al. (2011) Validation of the Turkish version of the problem areas in diabetes scale. Cardiovasc Psychiatry Neurol 2011: 315068.
-
Snoek FJ, Pouwer F, Welch GW, Polonsky WH (2000) Diabetes-related emotional distress in Dutch and US diabetic patients: cross-cultural validity of the problem areas in diabetes scale. Diabetes Care 23(9):1305-1309.
-
Hermanns N, Kulzer B, Krichbaum M, Kubiak T, Haak T (2006) How to screen for depression and emotional problems in patients with diabetes: comparison of screening characteristics of depression questionnaires, measurement of diabetes-specific emotional problems and standard clinical assessment. Diabetologia 49(3): 469-477.
-
Snoek FJ, Kersch NY, Eldrup E, Harman-Boehm I, Hermanns N, et al. (2012) Monitoring of Individual Needs in Diabetes (MIND)-2: follow-up data from the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) MIND study. Diabetes Care 35(11): 2128-2132.
-
Siaw MYL, Tai BB, Lee JY (2017) Psychometric properties of the Chinese version of the Problem Areas in Diabetes scale (SG‐PAID‐C) among high‐risk polypharmacy patients with uncontrolled type 2 diabetes in Singapore. J Diabetes Investig 8(2): 235-242.
-
Papathanasiou A, Koutsovasilis A, Shea S, Philalithis A, Papavasiliou S, et al. (2014) The Problem Areas in Diabetes (PAID) scale: psychometric evaluation survey in a Greek sample with type 2 diabetes. J Psychiatr Ment Health Nurs. 21(4): 345-353.
-
Arzaghi SM, Mahjouri MY, Heshmat R, Khashayar P, Larijani B, et al. (2011) Psychometric properties of the Iranian version of the Problem Areas in Diabetes scale (IR-PAID-20). Iran J Diabetes Metab Disorders 10: 1-7.
-
Fisher L, Glasgow RE, Strycker LA (2010) The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes care 33(5): 1034-1036.
-
Petrak F, Stridde E, Leverkus F, Crispin AA, Forst T, et al. (2007) Development and validation of a new measure to evaluate psychological resistance to insulin treatment. Diabetes Care 30(9): 2199-2204.
-
Fisher L, Mullan JT, Skaff MM, Glasgow RE, Arean P, et al. (2009) Predicting diabetes distress in patients with type 2 diabetes: a longitudinal study. Diabet Med 26(6): 622-627.
-
Ellouze F, Damak R, El Karoui M, Mami H, M’rad MF, et al. (2017) Depression in Tunisian type 2 diabetic patients: prevalence and association to glycemic control and to treatment compliance. Tunis Med 95(3): 210-214.
-
Gahlan D, Rajput R, Gehlawat P, Gupta R (2018) Prevalence and determinants of diabetes distress in patients of diabetes mellitus in a tertiary care centre. Diabetes Metab Syndr 12(3): 333-336.
-
Van Bastelaar KMP, Pouwer F, Geelhoed‐Duijvestijn PHLM, Tack CJ, Bazelmans E, et al. (2010) Diabetes‐ specific emotional distress mediates the association between depressive symptoms and glycaemic control in Type 1 and Type 2 diabetes. Diabet Med 27(7): 798-803.
-
Fisher L, Mullan JT, Arean P, Glasgow RE, Hessler D, et al. (2010) Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care 33(1): 23-28.
-
Abdelghaffar W, Amiri H, Zouari B (2020) Self-care activities adherence in Tunisian patients with type 2 diabetes: role of diabetes-related distress and self- efficacy. Acta Diabetol 57(5): 631-633.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty