Features of COVID-19 in the Elderly
The Coronavirus Disease 2019 (COVID-19) pandemic has caused havoc across the world over the past three years. The elderly people suffered the most during this unprecedented global public health calamity. The degree of suffering was magnified many fold in the elderly and frail individuals. They experienced atypical clinical disease presentation and developed more severe disease. Morbidity and mortality was also significantly higher in this group. Various risk factors have been identified that explain why older individuals are afflicted disproportionately and why they have an increased need for intensive care. Notably, severity of infections, vaccine-induced immune responses, and long-term outcomes of COVID-19 were also accentuated in the elderly, which have been explored in this review article..
Introduction
COVID-19 is caused by a coronavirus known as the severe acute respiratory syndrome coronavirus 2 (SARS- CoV-2). This belongs to the class of ß-coronaviruses, which have a single-stranded, positive-sense RNA genome of approximately 30 kb in size. The name ‘coronavirus’ comes from the Latin (‘corona’ = ‘crown’), as it resembles a crown due to the presence of spike proteins on its outer surface. Coronaviruses infects animals as well as humans. The animal coronaviruses were detected in the 1920s, whereas the first human coronavirus, named B814, was isolated in 1965 from the nasal swab of a boy suffering from a cold. The virus was isolated by Prof. David Tyrell, who was then the Director of
- the Common Cold Unit in Salisbury, Wiltshire, UK.
- In recent times, several novel coronaviruses with pandemic potential have been identified, of which severe acute respiratory syndrome coronavirus 1 (SARS-CoV-1) and the Middle-East respiratory syndrome coronavirus (MERS-
- CoV) have caused major global outbreaks (Table 1) [1].
- Virus
- Place of Discovery
- Year of Discovery
- SARS-CoV-1
- Yunnan, China
- 2003
- NL63
- Amsterdam, The
- Netherlands
- 2004
- HCoV-NH
- New Haven,
- Connecticut, USA
- 2005
- HKU-1
- Hong Kong
- 2005
- MERS-CoV
- Saudi Arabia
- 2012
- SARS-CoV-2
- Wuhan, China
- 2019
Table 1: Recently discovered coronaviruses with pandemic
Origin and Transmission of SARS-CoV-2
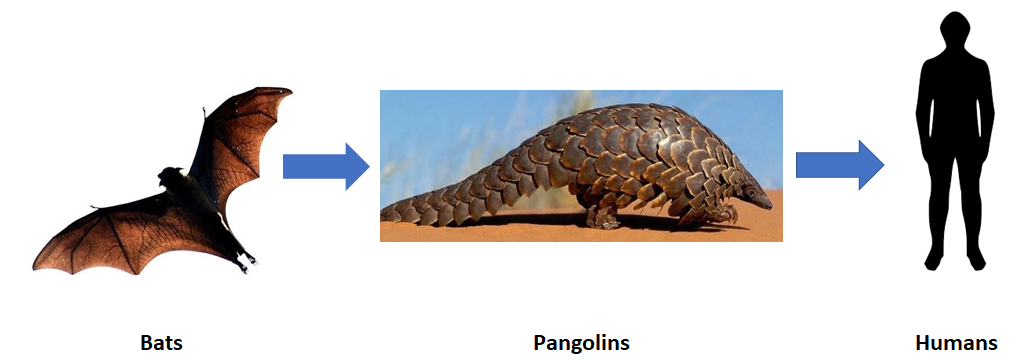
COVID-19 is caused by SARS-CoV-2, which normally circulates in bats that act as the reservoir host. It is believed that the virus was transmitted from bats to pangolins (intermediate host) and then jumped the species barrier and infected humans (incidental host), leading to human-to- human transmission (Figure 1).
It is now common knowledge that the pandemic originated in the city of Wuhan in the Hubei Province of eastern China. The notorious wet market in the city has been blamed for the origin of the initial outbreak.
Here, meat of exotic animals is sold for consumption, as a result of which the conditions are ripe for transmission of novel pathogens from animals to humans. And this is exactly what had happened.
The virus spread far-and-wide within a very short span of time. Wuhan is well connected with other major cities across China, including Beijing, Shanghai, and Hong Kong. This allowed the virus to spread to hitherto unaffected areas in China and subsequently worldwide by air travel (Figure 2).

The World Health Organization’s Role in Tackling the COVID-19 Pandemic
WHO has been instrumental in tackling the pandemic on a war footing from start to finish. Initially, at the fag end of 2019, there was a cluster of pneumonia cases in Wuhan that exhibited atypical symptoms. This observation was reported to the Chinese authorities, but were not heeded. As a result, the situation spiraled out of control. When the WHO came to know about it on 31st December 2019, it was too late! Nevertheless, WHO swung into action from the following day (New Year’s Day, 2020) to tackle a potential pandemic of gigantic proportions. The timeline of WHO’s response is highlighted in Table 2 [2].
| Date | Response |
|---|---|
| 31st December 2019 | Cluster of atypical pneumonia cases of unknown cause reported from Wuhan, China |
| 1st January 2020 | WHO activated its Incident Management Support Team |
| 11th January 2020 | First genomic sequence of SARS-CoV-2 shared by China First COVID-19 death reported from China |
| 13th January 2020 | First COVID-19 death reported from outside China, in Thailand |
| 22nd January 2020 | WHO confirmed human-to-human transmission of SARS-CoV-2 |
| 30th January 2020 | WHO declared COVID-19 as a Public Health Emergency of International Concern (PHEIC), the highest level of warning under the International Health Regulations (IHR) |
| 11th March 2020 | WHO declared COVID-19 as a ‘pandemic’ |
Table 2: Timeline of WHO’s initial response to the COVID-19 pandemic.
Features of Acute Phase of COVID-19
SARS-CoV-2 infection mainly causes respiratory problems and is primarily transmitted through respiratory droplets and direct contact [3]. As of 23rd May 2024, there were 704 million confirmed cases and seven million deaths in 231 countries worldwide [4]. Numerous symptoms have been identified, many of which overlap. This indicates that infection of many organs occur simultaneously. Symptoms may include cough, fatigue, anosmia, ageusia, breathing difficulty, myalgia, and forgetfulness, among many others. The major symptoms and their underlying pathology are presented in Figure 3.

Major complications of SARS-CoV-2 infection in the acute phase of COVID-19 include acute viral pneumonitis that leads to acute respiratory distress syndrome (ARDS), acute kidney injury (AKI), proinflammatory hypercoagulable blood with thromboembolism, sepsis, and cardiac problems. It is believed that a pro-inflammatory state accompanied by cytokine release are responsible for the complications [5, 6].
Serious complications that characterize severe COVID depend on many risk factors and morbidities, which are listed below:
- Cancer
- Cerebrovascular diseases
- Chronic kidney disease (CKD)
- Chronic lung diseases
- Chronic liver diseases
- Type-2 diabetes mellitus
- Physical disabilities
- Congestive heart failure, coronary artery disease, and other cardiomyopathies
- Psychiatric disorders
- Obesity
- Physical inactivity
- History of smoking
- Use of immunosuppressive drugs
Features of COVID-19 in the Elderly
The elderly bore the brunt of the burden during the entire span of the COVID-19 pandemic, which the WHO aptly termed as a Public Health Emergency of International Concern (PHEIC) way back in January, 2020.
Elderly individuals have been found to be more susceptible to SARS-CoV-2 infection. At the beginning of the pandemic, China reported that there was increased severity of disease and mortality among elderly individuals aged 60 years and above, which was similar to the pattern observed in Europe [7]. Deaths were as high as 10% in the elderly (>70 years), compared to <1% in young adults [8]. This is worrisome, as this age group accounts of 12% of the global population, or in other words, 800 million people [9].
Moreover, older COVID patients showed increased need for mechanical ventilation in intensive care units (ICUs), compared to young adults [10].
Older patients also exhibit atypical clinical signs and those with respiratory infection can also experience fatigue, anorexia and delirium, even though fever and productive cough are absent [11]. This can result in delayed diagnosis, thereby contributing to increased mortality.
Research has shown that approximately 1 in 10 elderly people die from COVID-19. In case of hospitalized old-age patients, approximately 11% succumb. This reflects the decreased resilience of elderly COVID patients. Eight out of 10 elderly COVID patients exhibit at least one comorbidity. Hypertension is the most common, followed by diabetes mellitus, and cardiovascular disease. This indicates the likelihood of adverse outcomes in this group of patients. Most common symptoms are fever (83%), cough (60%), and dyspnea (42%). Dry cough (56%) is more common than productive cough (28%). Among gastrointestinal symptoms, diarrhea is the most common, followed by anorexia. Hematological findings indicate that lymphopenia (52%) is most common in elderly COVID patients, followed by leukopenia (20%). Bilateral lung infiltrates (76%) is the most common radiologic finding in elderly patients. Oxygen support is required by 84% of elderly individuals, while invasive mechanical ventilation is required by 21%. About 4% individuals require non-invasive ventilation. With reference to complications in elderly COVID patients, the most common is secondary infection (34%), followed by AKI (22%), and ARDS (20%) [12].
In case of prolonged immobilization and restricted movement, as occurs during hospitalization, muscle mass and strength have been found to significantly decrease, particularly in elderly individuals. Notably, elderly COVID patients tend to have prolonged hospital or ICU stays, which on average is three weeks.
Bed rest is recommended to reduce the metabolic demand and reorient resources to facilitate recovery. However, prolonged immobilization during hospital stays have a negative impact on the body. These include muscle wasting, loss of contractile strength of muscles, and reduction in muscle protein turnover, among others [13]. The effect of prolonged immobility on the musculoskeletal system of patients has been reported earlier [14], but little information is available in case of patients infected with SARS-CoV-2. Thus, there is scope to address this aspect through research.
Conclusion
Over the past three years, much has been learned about COVID-19 and its many ramifications. Yet there is much more that remains to be deciphered. Studies have shown that older COVID patients exhibit severe disease, critical illness, and high mortality. They also experience muscle weakness and muscle loss due to prolonged inactivity, arising from hospitalization and lockdowns. They also experience many other complications, compared to their younger counterparts. Thus, concerted efforts should be made to alleviate the suffering of this vulnerable and neglected population, who possess the collective wisdom capable of benefitting this and future generations.
References
-
Bharati K (2020) History of coronaviruses: Why is it important in the context of COVID-19. Indian Science Cruiser 34(6): 6-10.
-
Bharati K (2020) What impact could the COVID-19 pandemic have on public health. Indian Science Cruiser 34(2): 47-53.
-
Harapan H, Itoh N, Yufika A, Winardi W, Keam S, et al. (2020) Coronavirus disease 2019 (COVID-19): A literature review. Journal of Infection and Public Health 13(5): 667-673.
-
Coronavirus Tracker (2024) Covid-19 Coronavirus Pandemic. Worldometer.
-
Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, et al. (2020) COVID-19: Consider cytokine storm syndromes and immunosuppression. The Lancet 395(10229): 1033-1034.
-
Ranucci M, Ballotta A, Di Dedda U, Bayshnikova E, Poli MD, et al. (2020) The procoagulant pattern of patients with COVID-19 acute respiratory distress syndrome. Journal of Thrombosis and Haemostasis 18(7): 1747- 1751.
-
Who (2020) Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Reliefweb.
-
Onder G, Rezza G, Brusaferro S (2020) Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. Journal of the American Medical Association 323(18): 1775-1776.
-
Divo MJ, Martinez CH, Mannino DM (2014) Ageing and the epidemiology of multimorbidity. European Respiratory Journal 44(4): 1055-1068.
-
Liu K, Chen Y, Lin R, Han K (2020) Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. Journal of Information Security 80(6): e14-e18.
-
Limpawattana P, Phungoen P, Mitsungnern T, Laosuangkoon W, Tansangworn N (2016) Atypical presentations of older adults at the emergency department and associated factors. Archives of Gerontology and Geriatrics 62: 97-102.
-
Singhal S, Kumar P, Singh S, Saha S, Dey AB (2021) Clinical features and outcomes of COVID-19 in order adults: A systematic review and meta-analysis. BMC Geriatrics 21(1): 321.
-
Bloomfield SA (1997) Changes in musculoskeletal structure and function with prolonged bed rest. Medicine & Science in Sports & Exercise 29(2): 197-206.
-
Stainsby BE, Howitt S, Porr J (2011) Neuromusculoskeletal disorders following SARS: A case series. The Journal of the Canadian Chiropractic Association 55(1): 32-39.