Treatment Strategies for Elderly and Frail COVID-19 Patients
The Coronavirus Disease 2019 (COVID-19) pandemic has had a tremendous negative impact on the health systems of all countries worldwide. Medical services had been halted due to disrupted supply chains, arising from the havoc wreaked by the pandemic. Essential life-saving medicines couldn’t reach the patients who needed them most. Moreover, there was a severe shortage of doctors and nurses too. With the progress of the pandemic, the hospitals became increasingly overburdened. As a result, treating COVID patients became extremely challenging. Caring for the elderly became even more challenging. Notably, this vulnerable group had been disproportionately affected by the pandemic and have had to bear the brunt of the burden. Treatment strategies for elderly and frail patients need to be tailor-made and fine-tuned, so that these cater to their specialized needs. The various strategies for treating this group of patients have been discussed in this review.
Abbreviations
WHO: World Health Organization; ADL: Activities of Daily Living; CDC: Centers for Disease Control and Prevention; ICU: Intensive Care Unit; ARDS: Acute Respiratory Distress Syndrome; AEs: Adverse Events; SOC: Standard of Care; HIV: Human Immunodeficiency Virus; MAbs: Monoclonal Antibodies; USFDA: United States Food and Drug Administration; MEWS: Modified Early Warning Score.
Introduction
The World Health Organization (WHO) defines ‘frailty’ as “a condition characterized by an increased age-related vulnerability due to a reduced physiological reserve and function of systemic organs, and is associated with an impairment of activities of daily living (ADL)” [1]. Frailty is a common occurrence in older adults, aged above 70 years. The incidence of frailty occurs more with age. It has been found that 15% and 25% of individuals above 65 and 85 years are affected by frailty, respectively [2].
Coronavirus Disease 2019 (COVID-19) can affect people of all ages, but especially the elderly and frail. Since the beginning of the COVID-19 pandemic, the elderly have been most affected by severe disease.
This is largely due to the presence of various comorbidities, including hypertension, diabetes, respiratory, and cardiovascular diseases [3].
Susceptibility of Elderly and Frail Individuals to COVID-19
Elderly and frail COVID patients are much more susceptible to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection and account for approximately 51% of hospitalized patients. Risk factors such as malnutrition, prolonged bed rest, and associated comorbidities can aggravate the infection. Frail older adults are at a higher risk of severe disease than non-frail older adults. Moreover, these patients are at a higher risk of dying compared to those who are not frail [4]. The Centers for Disease Control and Prevention (CDC) has reported that adults aged above 65 years account for 31% of COVID cases, 45% of hospitalizations, 53% of Intensive Care Unit (ICU) admissions, and 80% of deaths from the disease. Notably, the highest percentage of severe outcomes is in those aged above 85 years [5].
Pathogenesis of COVID-19 in Elderly and Frail Individuals
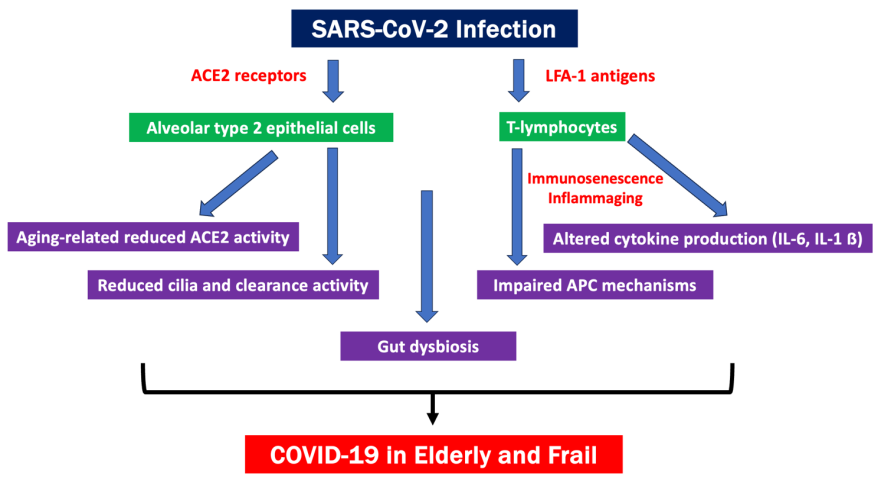
Several mechanisms of pathogenesis of COVID-19 in elderly and frail individuals have been identified. These include immunosenescence, inflammaging, and gut microbial dysbiosis [6]. Immunosenescence occurs due to impairment of the immune system and is linked to aging. The immune system of elderly individuals is very weak, resulting in reduced capacity to fight infections, which hampers pathogen clearance. Inflammaging is another immune mechanism associated with aging. This is characterized by chronic systemic inflammation. In inflammaging, the immune system is always hyperactive, but not effective [7]. Microbial dysbiosis of the gut is also associated with aging. It can result from oxidative stress, chronic systemic inflammation, insulin resistance, and may impair muscle contraction. Gut dysbiosis is also associated with altered inflammatory response and immune function in elderly COVID patients, leading to increased severity of disease [8]. Figure 1 shows the main aging-related mechanisms that may be involved in promoting severe forms of COVID-19 in older adults.
Strategies for Treating Elderly and Frail COVID-19 Patients
Various drugs are available to reduce the disease severity, hospitalization, morbidity, and mortality in COVID patients. Some of these include steroids, antivirals, monoclonal antibodies, antisenescence drugs, as well as some non- pharmacological interventions. These are briefly discussed below.
Corticosteroids: Dexamethasone is the drug of choice for treating hospitalized patients suffering from severe COVID-19 pneumonia. For elderly patients, cortisone therapy is recommended where hyperinflammation is present. The United Kingdom’s clinical trial, named ‘Randomized Evaluation of COVID-19 Therapy’ (RECOVERY) has demonstrated the efficacy of dexamethasone in reducing mortality within 28 days in COVID patients undergoing invasive mechanical ventilation or on oxygen support.
It has been shown that prolonged administration of corticosteroids is likely to accelerate recovery from Acute Respiratory Distress Syndrome (ARDS), thereby reducing the number of hospital deaths [9]. It has also been demonstrated that an early short course of methylprednisolone can improve clinical outcomes in COVID patients with moderate- to-severe disease [10]. Experts have recommended that administration of short courses of corticosteroids at low- to-moderate doses may be used in selected COVID patients presenting with hyperactive immune responses.
Glucocorticoids should be used with caution in elderly COVID patients as excessive doses can lead to immunosuppression, resulting in delayed clearance of the virus. During glucocorticoid use, its detrimental effect on fluid retention and blood pressure should be kept in mind. The elderly may also exhibit fluctuations in blood glucose levels compared to younger adults. So, in order to prevent glucocorticoid-induced diabetes, large doses and long-term use should be avoided.
Antivirals
Only two antivirals have been proven to be beneficial in elderly patients (Remdesivir and PaxlovidTM), which are highlighted below:
Remdesivir: The is the first antiviral drug to be approved for COVID patients at high risk of developing severe disease. Remdesivir is a viral RNA polymerase inhibitor and adenosine nucleotide analogue [11].
There is limited evidence on the effectiveness and safety of remdesivir in elderly and frail COVID patients. Having said this, some studies have shown that this drug can reduce the risk of severe disease in this vulnerable population. An analysis, based on the SEMI-COVID-19 Registry of 4,331 elderly hospitalized COVID patients aged ≥ 80 years in Spain, has shown that 140 of these elderly patients who were treated with remdesivir had a lower risk of death, compared to those who were not treated [12].
Despite its beneficial effects, remdesivir can cause severe hepatic and/or renal dysfunction. Therefore, the drug should be used with caution, with monitoring of liver and kidney function. There is little evidence on the safety profile of remdesivir in elderly and frail COVID patients. A study was conducted on 80 COVID patients of whom 32.5% were aged ≥ 80 years. This study showed that remdesivir-induced liver dysfunction occurred in 36.3% of all age groups, with no significant difference in adverse events (AEs) between the younger and older patients [13].
PaxlovidTM: This antiviral is a combination of nirmatrelvir and ritonavir and has been approved for treating COVID patients. It is recommended for patients who do not require supplemental oxygen therapy and should be administered within 5 days of onset of symptoms. PaxlovidTM can reduce the risk of severe disease by 89%, compared to standard of care (SOC), without any safety issues [14].
Nirmatrelvir inhibits the 3CL main protease (Mpro) of SARS-CoV-2 and reduces its replication in human cells, while ritonavir is a strong inhibitor of cytochrome P450 (CYP) 3A4 and acts as a strong pharmacokinetic boosting agent. Ritonavir is a repurposed drug, which has long been used as a protease inhibitor against the Human Immunodeficiency Virus (HIV) in AIDS patients. The drug is capable of reducing hospitalization rates and risk of death associated with COVID-19 in elderly patients aged ≥ 65 years, but not in younger patients [15]. Despite its benefits, PaxlovidTM is limited by the interactions with other drugs, which could complicate matters while treating the elderly and frail, where comorbidities are often associated with polypharmacy [16].
Monoclonal Antibodies
Monoclonal antibodies (mAbs) can be used for treating hospitalized COVID patients to reduce the chances of severe disease. However, treatment with mAbs should begin within seven days of symptom onset. Some mAbs include casirivimab/imdevimab, bamlanivimab/etesevimab, and sotrovimab. Notably, mAbs can be used in elderly individuals. This is substantiated by studies that have tested mAbs in this population. For example, a single-center retrospective observational study conducted in France among 36 elderly hospitalized patients who were administered sotrovimab, showed that none of them required specialized care in an ICU. Additionally, there were no significant AEs after treatment [17].
The PROVENT randomized, phase 3 clinical trial was conducted on 5,197 elderly individuals > 60 years of age. The trial evaluated one dose of tixagevimab-cilgavimab (Evusheld) vs placebo in these vulnerable individuals at increased risk of SARS-CoV-2 infection. The study showed a significant risk reduction in drug vs placebo-treated patients [18]. The efficacy and safety of Evusheld for early treatment of COVID-19 was evaluated in the TACKLE Study. This study showed a significant reduction in progression to severe disease or death in drug vs placebo-treated patients [19]. Based on these findings, Evusheld has been recommended for COVID patients aged ≥ 60 years with comorbidities or poor response to vaccination.
Tocilizumab is a mAb that directly targets Interleukin 6 (IL-6) receptors. This mAb has been shown to improve the clinical outcomes in severe COVID-19 by suppressing the immune response [20]. Other mAbs that specifically target the IL-6 pathway, such as sarilumab and siltuximab, are also recommended for treating severe COVID cases with pulmonary complications.
Besides the above, there are some cocktail mAbs. One such cocktail is composed of two fully humanized mAbs, namely, imdemab and casirivimab, which bind to different parts of the SARS-CoV-2 spike protein, thereby increasing antiviral efficacy and minimizing the chance of virus escape. These two mAbs have been officially approved by the United States Food and Drug Administration (USFDA) for use in the form of a cocktail. The USFDA recommends using this cocktail for treating non-hospitalized patients with mild-to-moderate COVID-19, who are at an elevated risk of developing serious illness [21].
Antisenescence Drugs
Several drugs have been proposed to possess antisenescence properties. But only rapamycin has shown some promise for elderly COVID patients. Rapamycin is generally used as an anti-aging drug that slows down the process of senescence, which has been demonstrated by human cell culture and animal models [22]. Rapamycin has been found to significantly reduce the expression of IL-6, a senescence marker present in serum. This is especially observed in elderly patients and those with Coronary Heart Disease (CHD) or reduced T-cell counts [23]. In the context of COVID-19, rapamycin is likely to halt the progression to severe disease by down regulating the IL-6 pathway and decreasing the number of senescent T-cells [24]. Thus, experts advise that this promising antisenescence drug should be further evaluated clinically in elderly COVID patients.
Non-Pharmacological Interventions
Asymptomatic or paucisymptomatic elderly COVID patients should be carefully evaluated. Keeping hydrated, maintaining adequate nutrition, and stabilizing underlying disorders are essential to reduce the risk of hospitalization due to deterioration of physical and mental health. Frail COVID patients who are hospitalized are at a higher risk of hyperactive delirium, which is often associated with risk factors such as acute urinary tract infection (UTI), hospitalization stress, lung failure, hypoxia, dehydration, and pain. Therefore, reducing these risk factors is likely to decrease the risk of developing delirium, which is often linked to increased in-hospital mortality risk from COVID-19, especially in the elderly and frail [25].
A thorough clinical evaluation is essential for promptly identifying any causes for deterioration of the patient’s condition. Monitoring the peripheral oxygen saturation (SpO2) and employing scales, such as the Six Minute Walk Test and the Modified Early Warning Score (MEWS) are very useful for evaluating the risk of deterioration of elderly COVID patients [26].
Conclusion
The COVID-19 pandemic has opened our eyes to the historic challenge of protecting the elderly and frail population worldwide. Protecting older people is a central question in maintaining global health as a whole. Although vaccination has radically improved the outcome of COVID patients in general, elderly and frail patients still remain vulnerable despite full vaccination. Therefore, effective therapies are very important for saving the lives of this vulnerable population. Physicians are encouraged to develop personalized treatment plans that are tailored to the specific needs of the elderly and frail, which will require a comprehensive geriatric assessment to identify the lacunae in the current treatment approaches. But just developing therapies will not suffice. Side-by-side, it must be remembered that there are still huge barriers in access to quality healthcare, especially in low-resource countries. These challenges must be overcome in order to ensure equitable access to healthcare across the globe, especially among those who need it most.
References
-
Clinical Consortium on Healthy Ageing. Topic Focus: Frailty and Intrinsic Capacity (2016). World Health Organization.
-
Tana C, Moffa L, Falasca K, Vecchiet J, Tana M, et al. (2023) Approach to COVID-19 in older adults and indications for improving the outcomes. Annals of Medicine 55(2): 2265298.
-
Jachymek M, Cader A, Ptak M, Witkiewicz W, Szymanski AG, et al. (2022) The value of clinical frailty scale (CFS) as a prognostic tool in predicting mortality in COVID-19 - A retrospective cohort study. International Journal of Environmental Research and Public Health 19(3): 1104.
-
Fernandes AL, Pereira RMR (2022) Frailty in the context of COVID-19 pandemic: A life-threatening condition. Frontiers in Medicine 9: 965562.
-
CDC COVID-19 Response Team (2020) Severe outcomes among patients with coronavirus disease 2019 (COVID- 19)-United States, February 12 - March 16, 2020. Morbidity and Mortality Weekly Report 69(12): 343- 346.
-
Mueller AL, McNamara MS, Sinclair DA (2020) Why does COVID-19 disproportionately affect older people? Aging 12(10): 9959-9981.
-
Franceschi C, Bonafè M, Valensin S, Olivieri F, De Luca M, et al. (2000) Inflammaging. An evolutionary perspective on immunosenescence. Annals of the New York Academy of Sciences 908(1): 244-254.
-
Ticinesi A, Tana C, Nouvenne A (2019) The intestinal microbiome and its relevance for functionality in older persons. Current Opinion in Clinical Nutrition and Metabolic Care 22(1): 4-12.
-
Meduri GU, Schwingshackl A, Hermans G (2016) Prolonged glucocorticoid treatment in ARDS: Impact on intensive care unit-acquired weakness. Frontiers in Pediatrics 4: 69.
-
Fadel R, Morrison AR, Vahia A, Smith ZR, Chaudhry Z, et al. (2020) Early short course corticosteroids in hospitalized patients with COVID-19. Clinical Infectious Diseases 71(16): 2114-2120.
-
Garibaldi BT, Wang K, Robinson ML, Betz J, Alexander GC, et al. (2022) Real-world effectiveness of remdesivir in adults hospitalized with coronavirus disease 2019 (COVID-19): A retrospective, multicenter comparative effectiveness study. Clinical Infectious Diseases 75(1): e516-e524.
-
Ramos-Rincon JM, López-Carmona MD, Palacios LC, López-Sampalo A, Rivas MR, et al. (2022) Remdesivir in very old patients (≥80 years) hospitalized with COVID-19: Real world data from the SEMI-COVID-19 registry. Journal of Clinical Medicine 11(13): 3769.
-
Kanai O, Fujita K, Nanba K, Esaka N, Hata H, et al. (2021) Safety of remdesivir for patients 80 years of age or older with coronavirus disease 2019 (COVID-19). Drugs and Aging 38(12): 1067-1074.
-
Hammond J, Tebbe HL, Gardner A, Abreu P, Bao W, et al. (2022) Oral nirmatrelvir for high-risk, non-hospitalized adults with COVID-19. New England Journal of Medicine 386(15): 1397-1408.
-
Arbel R, Sagy YW, Hoshen M, Battat E, Lavie G, et al. (2022) Nirmatrelvir use and severe COVID-19 outcomes during the omicron surge. New England Journal of Medicine 387(9): 790-798.
-
Chen J, Browne T (2022) Optimizing medication reconciliation among older adults during COVID-19 infection treatment with paxlovid. Innovation in Aging. 6 (S1): 828-829.
-
Brandin T, Capelle H, Allemand J, Cheung LF, Dumazer C (2023) 4CPS-074 Efficacy and safety of sotrovimab: Results of a retrospective observational study in a French hospital. European Journal of Hospital Pharmacy 30 (S1): A48.
-
Levin MJ, Ustianowski A, De Wit S, Launay O, Avila M, et al. (2022) Intramuscular AZD7442 (Tixagevimab- Cilgavimab) for prevention of COVID-19. New England Journal of Medicine 386(23): 2188-2200.
-
Montgomery H, Hobbs FDR, Padilla F, Arbetter D, Templeton A, et al. (2022) Efficacy and safety of intramuscular administration of tixagevimab-cilgavimab for early outpatient treatment of COVID-19 (TACKLE): A phase 3, randomized, double-blind, placebo-controlled trial. Lancet Respiratory Medicine 10(10): 985-996.
-
Xu X, Han M, Li T, Sun W, Wang D, et al. (2020) Effective treatment of severe COVID-19 patients with tocilizumab. Proceedings of the National Academy of Sciences of the United States of America 117(20): 10970-10975.
-
Li Q, Zhao C (2021) A review of the current status of clinical management of COVID-19 in the elderly. Medical Science Monitor 27: e930278.
-
Sargiacomo C, Sotgia F, Lisanti MP (2020) COVID-19 and chronological aging: Senolytics and other anti-aging drugs for the treatment or prevention of coronavirus infection? Aging (Albany NY) 12(8): 6511-6517.
-
Singh M, Jensen MD, Lerman A, Kushwaha S, Rihal CS, et al. (2016) Effect of low-dose rapamycin on senescence markers and physical functioning in older adults with coronary artery disease: Results of a pilot study. Journal of Frailty and Aging 5(4): 204-207.
-
Omarjee L, Janin A, Perrot F, Laviolle B, Meilhac O, et al. (2020) Targeting T-cell senescence and cytokine storm with rapamycin to prevent severe progression in COVID-19. Clinical Immunology 216: 108464.
-
Parrotta I, Bencivenga L, Okoye C, Bellelli G, Fumagalli S, et al. (2023) Frailty and hyperactive delirium in hospitalized older patients with COVID-19: An insight from GeroCovid registry. Aging Clinical and Experimental Research 35(2): 433-442.
-
Tagliabue F, Schena D, Galassi L, Magni M, Guerrazzi G, et al. (2021) Modified national early warning score as early predictor of outcome in COVID-19 pandemic. SN Comprehensive Clinical Medicine 3(9): 1863-1869.