Urinary Incontinence and Overactive Bladder Syndrome Impact on Quality of Women Sexual Life
Background: To evaluate the impact of overactive bladder syndrome (OAB) and urinary incontinence (UI) on women sexual life in patients from Hospital of Lithuanian University of Health Sciences Kaunas Clinic (LUHS KC) Woman consultation. Methods: Participants were questioned anonymously, using “The Female Sexual Function Index” (FSFI) survey. Data analysis was made using SPSS 20.0 program. Results: The first research showed that all FSFI domains means were statistically higher in women without UI during sexual intercourse, than those with UI. In addition, the second research showed that according to age all the domains scores were found higher in the groups of women (with or without overactive bladder syndrome) younger than 60 years old (p
Introduction
In 2002 International Continence Society defined Overactive bladder syndrome as a symptom complex of urinary urgency (with or without urge incontinence), urinary frequency (voiding 8 or more times in a 24-h period), and nocturia (awakening at night to void) without any pathologic or metabolic disorders [1]. According to the recent results in the United States, United Kingdom and Sweden from the Epidemiology of Lower Urinary Tract Symptoms (EpiLUTS) prevalence of overactive bladder syndrome among women aged 40y and older is from 32,6% to 41,3% [2, 3].
Although the reasons of why overactive bladder syndrome occurs are not clearly known. However, in most of the researches, main variables are highlighted, such as gender, age, race, ethnicity, vaginal childbirth, dietary and lifestyle factors, comorbid conditions as constipation, diabetes and obesity. According to studies, 28% of women that have had OAB but have not suffered from urge urinary incontinence, after 16 years started to feel the symptoms of it. Overactive bladder syndrome is debilitating and bothersome condition, which has a negative impact on overall health-related quality of life (HRQOL) in all 6
domains: physical functioning, role functioning, social functioning, mental health, health perception and bodily pain [4, 5, 6, 7, 8, 9]. In 2008 Nicolson et al. stated that patients feel the state of anxiety about previous urgency, fear about access to toilets outside the home, and because of that they organize their life around a variety of coping strategies [10, 11]. In addition, many scientific studies from all over the world suggested, that women with OAB suffer from pain or discomfort, dysuria, vulvodynia, needing to void during or after intercourse, and often feel unattractive to their partners, if they have to wear pads in bed [12, 13, 14]. Concerning the fact that there is still the gap of knowledge about these conditions we decided to describe findings of our researches in this article. Main goal of our studies was to investigate women with urinary incontinence or overactive bladder syndrome sexual function and sexual relationship with their partners.
Methods
This article discusses data of two studies that have been done in Lithuanian University of Health Sciences Kaunas Clinics (LUHS KC) Women consultation. The first research was carried out from January 2013 until May 2013. The second research was carried out over a restricted period of time from December 2014 until March 2015. In both researches participants were questioned anonymously, using “The Female Sexual Function Index” (FSFI) survey. In the first research, survey had two additional questions about urinary incontinence during sexual intercourse (1. Can you hold in urine? 2. Does it affect the relationship with partner?).The inclusion criteria were as follows: all women with UI who were between 17 and 75 years of age in the first investigation and women with OAB who were between 40 and 75 in the second investigation, could read and write, could communicate, did not have perception problems and were willing to voluntarily complete the surveys were included in the study. Women who had stress incontinence or mixed urinary incontinence or had not had sexual intercourse through the past year were excluded from these studies. In the research of 2013, there were given out 150 surveys, 96 of them gave feedback. In the following year research 90 surveys were given out and 77 of them gave feedback but only 60 surveys were completed correctly and were used. Data analysis was made using SPSS 20.0 program. Results of those surveys were considered significant when p<0.05. For both surveys bioethics authorizations were granted (No.BEC-MF-306, No.BEC-MF-297).
Results
First research
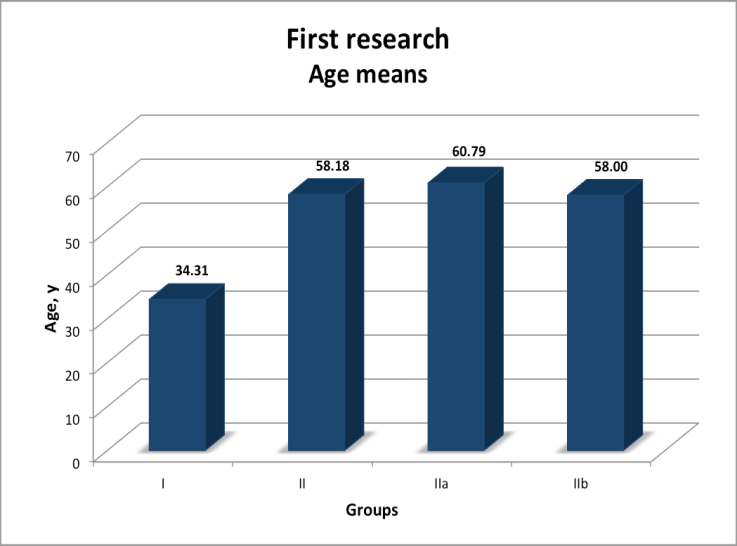
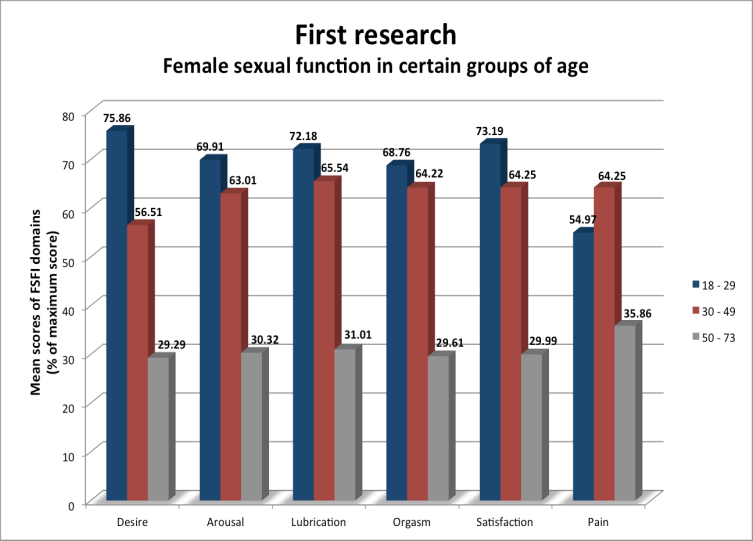
Women who participated in the research were between 17 and 73 years of age. Average age of participants was 41.8±16,1 years old (Figure1). While analyzing the data from FSFI survey, certain criteria were taken into consideration, such as desire, arousal, level of lubrication, orgasm, satisfaction and pain. Participants were divided into two groups: I (control group) - women who do not have problems with urinary incontinence during sexual intercourse (68, 5%), II (patient group) - women who have problems with urinary incontinence during sexual intercourse (31.5%). Second group was divided into two subgroups “a” and “b”. IIa (patient group) - women who have problems with urinary incontinence during sexual intercourse, but overall their relationships with partners are not harmed (51.9%) and group IIb (patient group)- women who have problems with urinary incontinence during sexual intercourse and because of that their relationships with partners are harmed (48.1%). II group age was statistically significant higher comparing with the control group (p<0.05). Continuing, sexual function of all women who have participated in the survey was evaluated by certain groups of age as well (Figure 2).Comparison was made between control group and patient group, which showed that all FSFI domains means are statistically higher of those women, who do not have urinary incontinence during sexual intercourse, than those who have. In patient group IIb orgasm and pain results were statistically higher than in the group IIa. Other FSFI domains results between subgroups were not statistically significant.
Second research
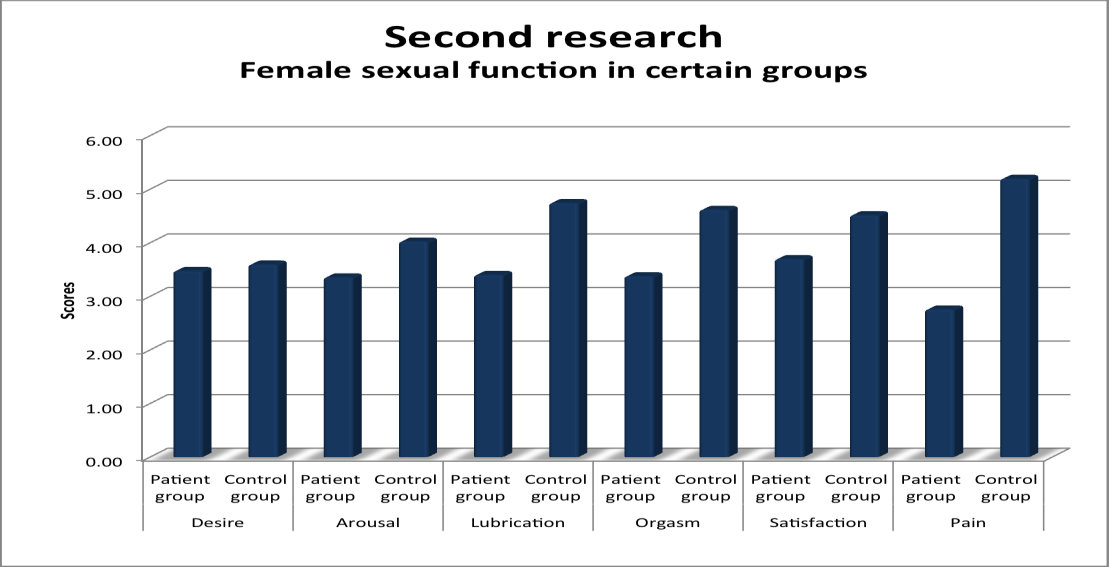
The age of women who participated in the research was between 41 and 71 years, the mean of age was 53,30y (range 9.272y). The findings from FSFI (The Female Sexual Function Index) questionnaires were used to measure sexual functioning of 6 domains in women: desire, arousal, lubrication, pain, orgasm, and satisfaction during sexual activity or intercourse. Respondents were divided into two groups: I (control group) - women without overactive bladder syndrome (66,7%): Ia – 40-59 years old women, Ib - ≥ 60 years old women; II (patient group) – women with overactive bladder syndrome (33,3%): IIa - 40-59 years old women, IIb ≥ 60 years old women. In the patient group 75% of women have been sexually active during the last four weeks, in the control group 100% of women have had sexual activity during the last four weeks. We determined that the difference of age between the groups were not statistically significant by using Student t test (p=0,361). Man - Whitney U test was used to compare FSFI domains scores between the groups: desire (p=0,918), arousal (p=0,534) and satisfaction (p=0.110) had no statistically significant difference, lubrication (p=0,019), orgasm (p=0,042) and pain (p=0,000) scores were statistically significantly lower in the patient group (Figure 3). The groups were also compared according to age. Scores of all the domains were higher in the groups of women (with or without overactive bladder syndrome) younger than 60 years old, except pain had no statistically significant difference in the patient group (Table 1). Also a moderate negative (r from -0.5 to -0.7) correlation had been determined between the women age and FSFI domains including desire, arousal, lubrication, orgasm and satisfaction. A weak negative linear relationship (r from 0,3 to -0,3) had been determined between age and pain.
| Control group | Patient group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FSFI domains | ||||||||||||
| <60y | ≥ 60y | p | <60y | ≥ 60y | p | |||||||
| Desire | 3,94 | 2,25 | 0,000 | 4,16 | 1,90 | 0,004 | ||||||
| Arousal | 4,33 | 2,81 | 0,003 | 4,29 | 1,20 | 0,002 | ||||||
| Lubrication | 5,07 | 3,45 | 0,001 | 4,31 | 1,30 | 0,007 | ||||||
| Orgasm | 4,89 | 3,55 | 0,004 | 4,31 | 1,20 | 0,002 | ||||||
| Satisfaction | 4,84 | 3,25 | 0,006 | 4,66 | 1,47 | 0,001 | ||||||
| Pain | 5,39 | 4,45 | 0,044 | 3,40 | 1,27 | 0,054 |
Discussion
Overactive bladder syndrome and urinary incontinence are closely related health problems, however the OAB syndrome can also be diagnosed to patients who have symptoms (frequent urination and nocturia) but still can hold urine. These two disorders are more common in women than men and progress with age [15]. There is no epidemiologic data on prevalence of overactive bladder syndrome or urinary incontinence in Lithuania. Most patients do not mention their complaints to the doctor because they think that overactive bladder symptoms are just normal changes due to effects of aging and deliveries. Previous researches suggest that parity may have an impact for OAB and urinary incontinence manifestation, possibly because of neurologic injury during vaginal delivery [16]. Despite that, neither patients nor medical practitioners should consider these two conditions as a normal state, because both OAB and urinary incontinence have a negative impact on the quality of life [17]. Furthermore, some authors even affirm that overactive bladder syndrome is associated with higher level of depression and stress, reduced working capacity and worse quality of sleep [18, 16]. In both described researches we ascertained that women with OAB or UI have a significantly worse sexual function comparing to women who have no urogynecologic disorders. Accordingly it is reflected in the findings of all six FSFI domains (desire, arousal, lubrication, pain, orgasm, and satisfaction). The greatest difference between the control group and patient group was in pain domain according to both of our researches. Likewise several foreign studies have also noticed association between OAB or UI and sexual function. As a result, women with overactive bladder symptoms had lower mean scores for all six domains of the FSFI [19, 20]. One of Coyne‘s KS et al. study presented the extracts from the interview with women who have OAB. Some of them complained about pain that lasted up to two days after sexual intercourse [13]. Moreover, previous studies have reported that sexual dysfunction in patients with OAB syndrome also results from suprapubic pain, dysuria, vulvodynia, and repeated experiences of having to go to the toilet or of needing to void during intercourse [21]. On the other hand, one research made in Turkey suggested that there was no statistically significant difference between the patient and control groups in the domains of pain and lubrication [22]. It is important to note that there are a lot of other factors which may have influence on sexual function, such as hormone balance, number of vaginal deliveries, pelvic organ prolapse, previous surgical interventions, social factors, chronic diseases (diabetes, thyroid diseases) and older age. Previous studies have reported that regardless of age, OAB patients experience more co-morbid conditions than non-OAB patients [20]. Therefore we chose to compare women sexual function in different age groups. In the first research women with UI older than 49y had the lowest scores of pain and arousal domains. In the second research women with OAB older than 60y had the lowest scores of desire and satisfaction components. Regardless the difference of the problems in patients with overactive bladder syndrome or urinary incontinence, in both researches overall sexual function was worse in older patients groups. In the first research respondents had also to answer two additional questions: 1. Can you hold in urine? 2. Does it affect relationship with partner? 31, 5% of women stated their inability to hold in urine during sexual intercourse. Less than a half of those respondents complained about the negative effect on their relationships with partners. Accordingly we suggest that urinary incontinence during sexual intercourse may not be the main reason that affects relationships between partners. However, previous researches reported that overactive bladder syndrome without urinary incontinence has negative effect on partners relationships due to decreased intimacy, fear of incontinence, urinary urgency and interruptions during intercourse to visit the bathroom before, during, and after sexual intercourse [13]. One of the most unexpected aspects in our first research was that sexual function is better in women who have urinary incontinence during sexual intercourse and because of that their relationships with partners are harmed, than those who have the same problem with urinary incontinence but their relationships are not harmed. We think it is because of older age of those who have urinary incontinence but are not fighting with partners. However, further researches are needed to confirm this statement. Ultimately we would like to clarify the limitations of our studies. Both researches had small sample size, which occurred because they both had been done in the same hospital and had been done during short periods of time. After all we think that the main aim and clinical implication of these studies is to note the impact of OAB and UI on women sexual health. Summing up the results of our researches and references, it is clear that general practitioners and sexologists should pay more attention to these conditions in order to improve women overall health and quality of life.
Conclusion
First research
- Evaluating women sexual function according to the groups of age: women between 18 and 29 years mostly have problems in an orgasm domain. Women between 30 and 49 mostly have problems in arousal and lubrication domains. Women from 50 to 73 years mostly have problems in pain and arousal domains.
- Women who are suffering from urinary incontinence during sexual intercourse have significantly worse sexual function, than those who do not have this problem.
- Less than a half of participants answered that urinary incontinence bothers sexual intercourse with partner.
- Sexual function is better in women who have urinary incontinence during sexual intercourse and because of that their relationships with partners are harmed, than those who have the same problem with urinary incontinence but their relationships are not harmed.
Second research
- As the age of participants is rising, sexual function is deteriorating and most problems arise in desire and satisfaction domains.
- Healthy women had significantly higher percentage of sexual intercourses throughout last four weeks, than those who have overactive bladder syndrome.
- Women who suffer from overactive bladder syndrome, sexual function is significantly worse, than those who do not suffer from it.
Those women most likely experience a decrease of lubrication, pain during sexual intercourse and lack of orgasm.
References
-
MacDiarmid S, Rosenberg M (2005) Overactive bladder in women: symptom impact and treatment expectations. Current medical research and opinion 21(9): 1413-1421.
-
Coyne KS, Sexton CC, Thompson C, Zoe S, Milsom I, et al. (2011) The impact of OAB on sexual health in men and women: results from EpiLUTS. Journal of Sexual Medicine 8(6): 1603-1615.
-
Eapen RS, Radomski SB (2016) Review of the epidemiology of overactive bladder. Dove Press Journal: Research and Reports in Urology 8: 71-76.
-
Coyne KS, Margolis MK, Brewster - Jordan J, Sutherland SE, Bavendam T, et al. (2007) Evaluating the Impact of Overactive Bladder on Sexual Health in Women: What is Relevant? Journal of Sexual Medicine 4(1): 124-136.
-
Serels S (2004) The Wet patient: understanding patients with overactive bladder and incontinence. Current medical research and opinion 20(6): 791- 801.
-
Wein AJ, Rovner ES (2002) Defintion and Epidemiology of Overactive Bladder. Urology 60(5 S1): 7-12.
-
Chen J, Sweet G, Shindel A (2013) Urinary Disorders and Female Sexual Function. Current Urology Reports 14(4): 298-308.
-
Ergenoglu AM, Yeniel AO, Itil IM, Askar N, Meseri R, et al. (2012) Overactive bladder and its effects on sexual dysfunction among women. Acta Obstetrica et Gynecologica Scandinavica 92(10): 1202-1207.
-
Irwin DE, Milsom I, Chancellor MB, Kopp Z, Guan Z (2010)Dynamic progression of Overactive Bladder and Urinary Incontinence Symptoms: A systematic review. European Association of Urology 58(4): 532- 543.
-
Kraus AR, Bavendam T, Brake T, Griebling TL (2010) Vulnerable Elderly Patients and Overactive Bladder Syndrome. Drugs Aging 27(9): 697-713.
-
Kinsey D, Pretorius S, Glover L, Alexander T (2014) The psychological impact of overactive bladder: A systematic review. Journal of Health Psychology 21(1): 69-81.
-
Dmochowski RR, Newman DK (2007) Impact of overactive bladder on women in the United States: results of a national survey. Current medical research and opinion 23(1): 65-76.
-
Abrams P, Kelleher CJ, Kerr LA, Rogers RG (2000) Overactive bladder significantly affects quality of life. American Journal of Managed Care 6(11): S580-S590.
-
Milsom I, Abrams P, Cardozo L, Roberts RG, Thuroff J, et al. (2001) How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. Journal of the British Association of Urological Surgeons 87(9): 760- 766.
-
Sut HK, Kaplan PB, Sut N, Tekbas S (2012) The assessment of quality of life in female Turkish patients with overactive bladder. International Journal of Nursing Practice 18(1): 20-17.
-
Stewart WF, Van Rooyen JB, Cundiff GW, Abrams P, Herzog AR, et al. (2003) Prevalence and burden of overactive bladder in the United States. World Journal of Urology 20(6): 327-336.
-
Simeonova Z, Milson I, Kullendorff AM, Molander U, Bengtsson C (1999) The prevalence of urinary incontinence and its influence on the quality of life in women from an urban Swedish population. Acta Obstetrica et Gynecologica Scandinavica 78(6): 546- 551.
-
Irwin DE, Milsom I, Hunskaar S (2006) Population- based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. European Urology 50(6): 1306-1314.
-
Kogan MI, Zachoval R, Özyurt C, Schäfer T, Christensen N (2014) Epidemiology and impact of urinary incontinence, overactive bladder, and other lower urinary tract symptoms: results of the EPIC survey in Russia, Czech Republic, and Turkey. Current Medical Research & Opinion 30(10): 2119-2130.
-
Coyne KS, Margolis MK, Jumadilova Z, Bavendam T, Rogers RG, et al. (2007) Overactive Bladder and Women’s Sexual Health: What is the Impact? Journal of Sexual Medicine 4(3): 656-666.
-
Kim YH, Seo JT, Yoon H (2005) The effect of overactive bladder syndrome on the sexual quality of life in Korean young and middle aged women. International Journal of Impotence Research 17(2): 158-163.
-
Sen I, Onaran M, Aksakal N, Acar C, Tan MO, et al. (2006) The Impact of Urinary Incontinence on Female Sexual Function. Advances in Therapy 23(6): 999- 1008.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’