Prenatal Diagnosis of Bilateral Fetal Duplex Kidneys and a Short Review about Duplex Kidneys
Duplex kidney is one of common major congenital abnormalities of the urinary tract with an incidence about 1% of all live births and higher frequency in females than in males. Majority of duplex kidneys are unilateral. Although the antenatal diagnosis of fetal hydronephrosis is simple, the diagnosis of fetal renal duplication is infrequent, especially in case the collecting system is not dilated. Here we reported bilateral duplex collecting system that is prenatally diagnosed with obstruction findings on one kidney and no obstructive findings on other side.
Gencdal and Sefa Kelekci
Izmir Katip Celebi University, Faculty of Medicine, Department of Obstetrics and Gynecology, Izmir, Turkey diagnosed with obstruction findings on one kidney and no obstructive findings on other side.
Introduction
Renal malformations consist 17% of prenatally diagnosed anomalies [1]. Duplex kidneys have a 1:125incidence in postmortem series and can be described common renal anomalies [2]. Most of affected individual’s course asymptomatically throughout life but a proportion will be symptomatic such as recurrent urinary tract infections [3]. So, prenatal detection of duplex renal system will be crucial. Prenatal diagnosis fetal duplex renal system is rare. Duplex renal system is a general definition congenital abnormality of the urinary tract characterized by partial or total duplication of the collecting system and renal pelvis and parenchyma [4]. It can be classified on the basis of which renal pole is involved (i.e., superior or inferior); on whether or not an ureterocele is associated with; and on the position of ureterocele (i.e., within the bladder or in the urethra) and function of the distal ureteral orifice (blind, stenotic, sphincteric or incompetent [5]. On prenatal sonography various findings can be detected. Always affected kidney has a greater size than the other. If urinary flow is affected, obstruction findings can be seen: eccentric hydronephrosis, most commonly involving the upper pole of the kidney; ballooning of the submucosal segment of the ureter into the bladder, leading to an intravesical cyst (ureterocele); and dilated ureter, due to either stenosis at the ureterovesical junction or reflux [6]. Structural anomalies of the kidney such asduplex kidneys are associated with a malpositioned ureteral orifice in embryonic period [7]. So, the underlying causeof duplex kidney and ureters may be the abnormal positioning and development of the primary uretericbud, or the development of an ectopic bud along the anterior– posterior axis of the Wolffian ducts. Consequently, two pelvicaliceal systems, associated with incomplete, partial or complete duplication of the ureters (single, bifid or double ureters). A bifid pelvis occurs when two pelvicaliceal systems join at the ureteropelvic junction. Partial duplication occurs when two bifid ureters join prior to emptying into the bladder. Where there are double ureters, each ureter drains a separate pelvicaliceal system and opens separately into the urinary or genital tract. Duplex kidneys have upper and lower poles, with the upper pole comprising about one-third of the parenchyma [8]. The upper pole ureter crosses the lower pole ureter, and may end low downside to other in the bladder, or ectopically, usually into the urethra, or rarely to vagina in females. Where it ends in the bladder it often forms an intra vesical ureterocele. Ureteroceles form cysticdilatations of the submucosal segment of the intravesical ureter with narrowing of the ureteral orifice [9]. The Weigert-Meyer Law is used to describe themigration and crossing of the ureteric buds which results in the lower pole of the duplex kidney draining through the upper ureteric orifice, and vice versa[10, 11].
Case Report
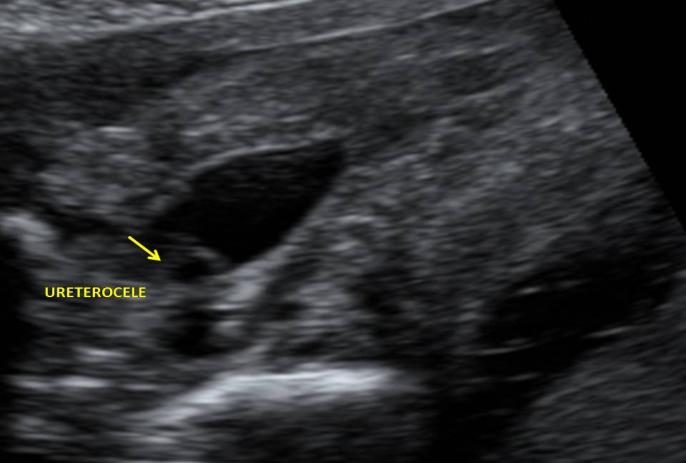
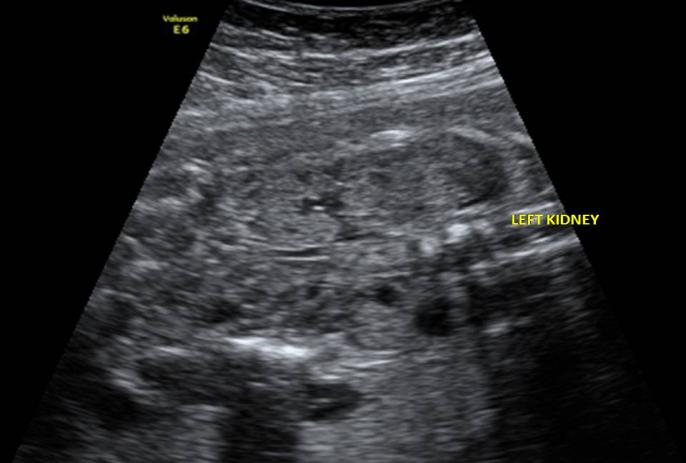
A 23-year-old woman, gravida 3, para 1, was referred at 25weeks gestation after detection of multiple anechoic masses in the fetal abdomen. Her medical and obstetric histories were unremarkable and the pregnancy had been otherwise uncomplicated. At referral, sonographic examination revealed a singleton male fetus with biometric measurements consistent with dates, posterior located placenta and normal amniotic fluid volume. Detailed examination of the fetal anatomy revealed bilateral duplex kidneys with unilateral severe hydronephrosis of the upper pole of right side; the renal upper pole AP was measured 18 mm, proximal ureter was measured 5,5 mm and distal ureter was 3.7 mm (Figure 1). The diameter of the right kidney was 50x22x33 mm. The ureter draining the upper moieties of right side were dilated, and the fetal bladder appeared septated, although a closer examination revealed one 3,8 mm tortuous, sac like structures protruding into the fetal bladder (ureterocele) and filling it almost completely (Figure 2). Left kidney also had double renal pelvis and double collecting systems. The diameter was 39x20x24mm and increased in size. But that was not hydronephrotic and ureterocele was not present on this side (Figure 3).
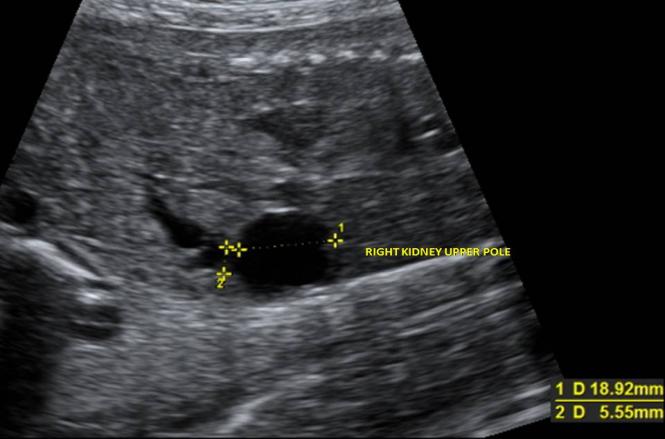
Figure 1: Right kidney upper pole and dilated pelvis. There was no other system additional structural anomaly. Fetal cardiac examination revealed normal findings. Cordocentesis is performed for karyotyping due to maternal anxiety. Fetal blood sampling revealed a normal 46, XYkaryo type. The patient delivered a male weighing 3200gram, withApgar scores of 9 and 10 at 1 and 5 min, respectively. Postnatal, surgery is planned for hydronephrotic kidney by pediatric urology.
Discussion
Commonly duplex renal system is unilateral. Postnatal data suggest that between 83 and 90% of cases are unilateral [12] and with involvement of the upper renal segment in 85% of cases and ureterocelein 24 to 47% of cases [13]. In our case duplex renal system was bilaterally present and only right kidney had obstructive sonographic pattern. Sizes of both kidneys were increased and both kidneys had double collecting system and ureters. Only the ureter of right kidney upper pole was dilated and ureterocele was only present on the intravesicale part of this ureter. There is no single ultrasonographic feature that is pathognomonic of duplex renal system because of the variable anatomic presentations of this anomaly. However, a combination of ultrasonographic patterns allows a high degree of accuracy. Adiagnosis of duplex renal system should be entertained in the presence various ultrasonographic findings. Eccentric hydronephrosis on the upper pole of kidney is an important feature for diagnosis. Rarely the lower ureter that is draining lower pole can be dilated due to compression of upper ureter. Presence of ureterocele in duplex renal system is reported as 55% (6 of 11) by Vergani et al. [5]. In larger series in pediatric population it was reported as 47% [6]. The detection of an ureterocele is reported to be strongly associated with diagnosis of duplex kidney, with 26/30 (88%) prenatally detected ureteroceles subsequently found to be associated with a duplex system [8]. In our case ureterocele was present only on right duplex kidney and only this kidney was hydronephrotic. Despite the presence of double collecting systems and double intravesicale ureteral endings on bladder on left duplex kidney, that was not hydronephrotic. That was due to absence of ureterocele on this side. Dilated ureters are another sign for duplex renal system. Dilatation of ureter is due to either obstruction of flow or vesico-ureteral reflux. Most individuals with duplex kidney have no degree of renal impairment, and probably remain undiagnosed throughout life. Vesico-ureteric reflux is present in 70% of patients with duplex kidneys and present with infection in early neonatal life [8]. Reflux usually involves only the lower poleureter in 90% of cases, due to its laterally ectopic situation, with both poles involved in the remainder if the upper pole ureter is also laterally ectopic [14]. Stenosis due to an ureterocele will cause significant dilatation of the ectopic ureter with obstruction of the upper renal moiety in 85% of cases [15]. If the ureterocele protrudes into the urethra or lower urinary bladder, mechanical obstruction of the bladder neck may ensue, causing bilateral hydronephrosis [16]. Abnormal karyotype is not higher in this group compared to general population. In our case prenatal karyotyping is performed due to maternal anxiety and karyotype was normal. Prenatal diagnosis of duplex system is crucial for early intervention and prevention of complications. Recurrent urinary infections may cause renal impairment and chronic pyelonephritis. In females if upperpole ureter enters the urethra or vagina, they may be complicated by continuous dribbling incontinence, and may not be immediately recognized [17]. Postnatal, after evaluation by sonography and micturating cystourethrogram to identify the presence of vesico-ureteric reflux a 99mtechnetium-dimercaptosuccinic acid (99mTc-DMSA) or mercaptoacetyl-triglycine (MAG3) isotope imaging is required at 6–12 weeks of age to assess differential renal function in both moieties of the duplex kidney. During this period, infant should be maintained on prophylactic antibiotics to minimize the risk of ascending urinary tract infection [9].
Conclusion
Duplex renal system should be kept in mind when unilateral or bilateral hydronephrosis is detected. Prenatal diagnosis is so important for early intervention.
References
-
Stefos T, Plachouras N, SotiriadisA, Papadimitriou D, Almoussa N, et al. (1999) Routine obstetric ultrasound at 18–22 weeks: our experience in 7,236 fetuses. J Matern Fetal Med 8(2): 64-69.
-
Nation EF (1944) Duplication of the kidney and ureter: a statistical study of 230 new cases. J Urol 51: 456.
-
Privett JTJ, Jeans WD, Roylance J (1976) The incidence and importance of renal duplication. ClinRadiol 27(4): 521-530.
-
Glassberg KI, Braren V, Duckett JW, Jacobs EC, King LT, et al. (1984) Suggested terminology for duplex systems, ectopic ureters and ureteroceles. J Urol 132(6): 1153-1154.
-
Vergani P, Ceruti P, Locatelli A, Mariani E, Paterlini G et al. (1999) Accuracy of Prenatal Ultrasonographic Diagnosis of Duplex Renal System. Ultrasound Med 18(7): 463-467.
-
Jee LD, Rickwood AM, Williams MP, Anderson PA (1993) Experiencewith duplex system anomalies detected by prenatal ultrasonography. J Urol 149(4): 808-810.
-
Mackie GG, Stephens FD (1975) Duplex kidneys: a correlation of renal dysplasia with position of the ureteral orifice. J Urol 114(2): 274-280.
-
Privett JTJ, Jeans WD, Roylance J (1976) The incidence and importance of renal duplication. ClinRadiol 27(4): 521-530.
-
Whitten SM, Wilcox DT (2011) Duplex systems. Prenat Diagn 21(11): 952-957.
-
Weigert C (1877) Uebereinige Bildunsfehler der Ureteren. Virchows Arch Path Anat Physiol Klin Med 70: 490-501.
-
Meyer R (1946) Normal and abnormal development of the ureter in the human embryo – a mechanistic consideration. Anat Rec 96(4): 355-371.
-
Jee LD, Rickwood AMK, Williams MPL, Anderson PA (1993) Experiencewith duplex system anomalies detected by prenatal ultrasonography. J Urol 149(4):808-810.
-
Winters WD, Lebowitz RL (1990) Importance of prenatal detectionof hydronephrosis of the upper pole. AJR 155(1):125-129.
-
Kaplan WE, Nasrallah P, King LR (1978) Reflux in complete duplication in children. J Urol 120(2): 220- 222.
-
Mascatello VJ, Smith EH, Carrera GF, Berger M, Teele RL (1977) Ultrasonicevaluation of the obstructed kidney. Am J Radiol 129(1): 113-120.
-
Schoenecker SA, Cyr DR, Mack LA, Shuman WP, Lenke RR (1985) Sonographicdiagnosis of bilateral fetal renal duplication with ectopicureterocoeles. J Ultrasound Med 4(11): 617-618.
-
Ahmed S, Morris LL, Byard RW (1992) Ectopic ureter with complete ureteral duplication in the female child. J Ped Surg 27(11): 1455-1460.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’