A Study on the Fetomaternal Outcome in Cases of Previous Three Caesarean Section
Introduction: Caesarean section is the most common obstetrical surgery performed worldwide. Its incidence continuously rising. The rate of caesarean section is 24.4% in urban educated India. In our college LSCS rate of previous 5 years is 25.4%, amongst which 0.2% were previous three LSCS. Methodology: A retrospective observational study of 200 cases of caesarean deliveries from January 2010 to December 2017 in a tertiary care centre. Cases were divided in four groups such as first LSCS, second LSCS, third LSCS and fourth LSCS, each group contained 50 cases. Results: Patients were grouped as per number of caesarean deliveries. There is an increase in maternal morbidity with increase in the number of previous caesarean deliveries. There is increased morbidity in the form of adherent placenta, blood loss, bladder, ureter injury, intra-operative adhesions, scar dehiscence, need for ICU admission. Conclusion: Cases of previous 2 and previous 3 LSCS are bound to increase in near future, such cases need proper referral to tertiary care centre for proper management based on the risk of varied complications.
Introduction
A Caesarean section is performed when delivering by vaginal route is difficult or there is risk to the mother or child. The incidence of caesarean section is continuously rising, giving women the title of “previous LSCS“.
The advents of better anaesthesia, availability of improved surgical techniques and prophylactic antibiotics have made caesarean section a relatively safer and common procedure. Rise in prevalence of induced labour and obesity along with decrease vaginal deliveries in pre- eclampsia and concerns for pelvic floor injury are also responsible for this trend. The decision whether to perform a caesarean or not, is based on the individualized judgement of obstetrician [1].
On the other hand, the secondary rise in repeat caesarean delivery has been associated with an increase in severe complications particularly the complications of placentation like placenta praevia and placenta accreta which in turn increases the maternal morbidity & even mortality [2, 3].
Most of the women with first caesarean section require a repeat caesarean section in their next pregnancy. Hence it is not uncommon to find multipara with previous 2, previous 3 LSCS these days. The scarred uterus is at a high risk of scar dehiscence and rupture. Also, the complication of morbidly adherent placenta, adherent bladder, intraoperative adhesions make it a high risk surgery with complications of blood loss, need for blood transfusions, post operative extensive morbidity and even in some cases need for ICU admission.
However only a small number of studies have been conducted to assess the maternal and fetal risks and the complications associated with repeat caesarean section. Therefore we conducted this study
- To estimate Whether maternal morbidity is increased with increasing number of caesarean deliveries
- To determine the effect of increasing number of caesarean deliveries on fetal outcome
Methodology
200 cased of LSCS were studied in our hospital, The Cama and Albless Hospital which is a tertiary care centre located in South Mumbai, from January 2010 to December 2017.
We divided them in four groups based on the order of the number of previous LSCS, each group contains 50cases.
- Group1- 1st LSCS
- Group2- 2nd LSCS (i.e. previous 1 LSCS)
- Group3- 3rd LSCS (i.e. previous 2 LSCS)
- Group4- 4th LSCS (i.e. previous 3 LSCS) These Cases were reviewed on the basis of age, type of operation, no. of caesarean sections, time of hospitalization and intraoperative and postoperative complications. Women undergoing increasing number of caesarean deliveries were compared to those undergoing primary caesarean deliveries regarding Feto-maternal outcome and surgical complications. The entire data collected was analysed for type and incidence of preoperative, intraoperative and postoperative maternal & fetal complications.
Observations and Results
Table1 Shows age wise distribution of patients undergoing caesarean deliveries. Maximum number of patients undergoing 4th LSCS those are operated thrice previously were found in older age group of 30-34years.
| 1st LSCS | 2nd LSCS | 3rd LSCS | 4th LSCS | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 20-24 | 23 | 11 | 2 | 0 | ||||||
| 25-29 | 19 | 23 | 18 | 2 | ||||||
| 30-34 | 7 | 13 | 23 | 39 | ||||||
| >34 | 1 | 3 | 7 | 9 | ||||||
| Total | 50 | 50 | 50 | 50 |
Table 1: Age wise distribution of patients undergoing caesarean deliveries.
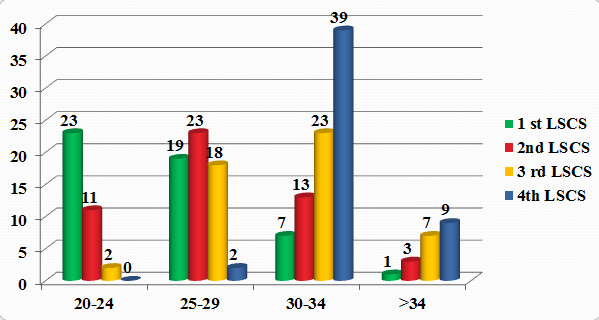
Graph 1: Age wise distribution of patients undergoing caesarean deliveries.
Maximum numbers of cases were unbooked. With increasing awareness among patients after previous surgeries due to counselling, more number of patients got registered in subsequent pregnancies to receive better health care (Table 2).
| Booked Cases | Unbooked Cases | |||
|---|---|---|---|---|
| 1st LSCS | 12 | 38 | ||
| 2nd LSCS | 23 | 27 | ||
| 3rd LSCS | 21 | 29 | ||
| 4th LSCS | 30 | 20 | ||
| Total | 86 | 114 |
Table 2: Booked cases verses unbooked.
When compared if the LSCS were done electively or in emergencies, maximum number of cases were found to be taken in emergencies, the incidence was significantly higher in women who had one previous CS when compared to group 3&4 (Table 3).
- 1st LSCS 2nd LSCS 3rd LSCS 4th LSCS
- Elective LSCS
- 4
- 9
- 21
- 32
- Emergence LSCS
- 46
- 41
- 29
- 18
Table 3: Type of LSCS.
The most common preoperative complication was anaemia in all groups of study, maximum being in patients undergoing 4th caesarean delivery. Maximum number of patients required blood transfusion either preoperatively or postoperatively, which was not related to operative complications but was given because of preoperative anaemia (Table 4).
- 1st LSCS 2nd LSCS 3rd LSCS 4th LSCS
- Anemia
- (mild/moderate) 29(58%) 26(54%) 30(60%) 32(64%)
- Severe anaemia 5(10%) 6(12%) 5(10%)
- 5(10%)
- Placenta previa
- 1
- 0
- 3
- 2
- Placenta accreta
- 0
- 0
- 1
- 0
Table 4: Preoperative complications.
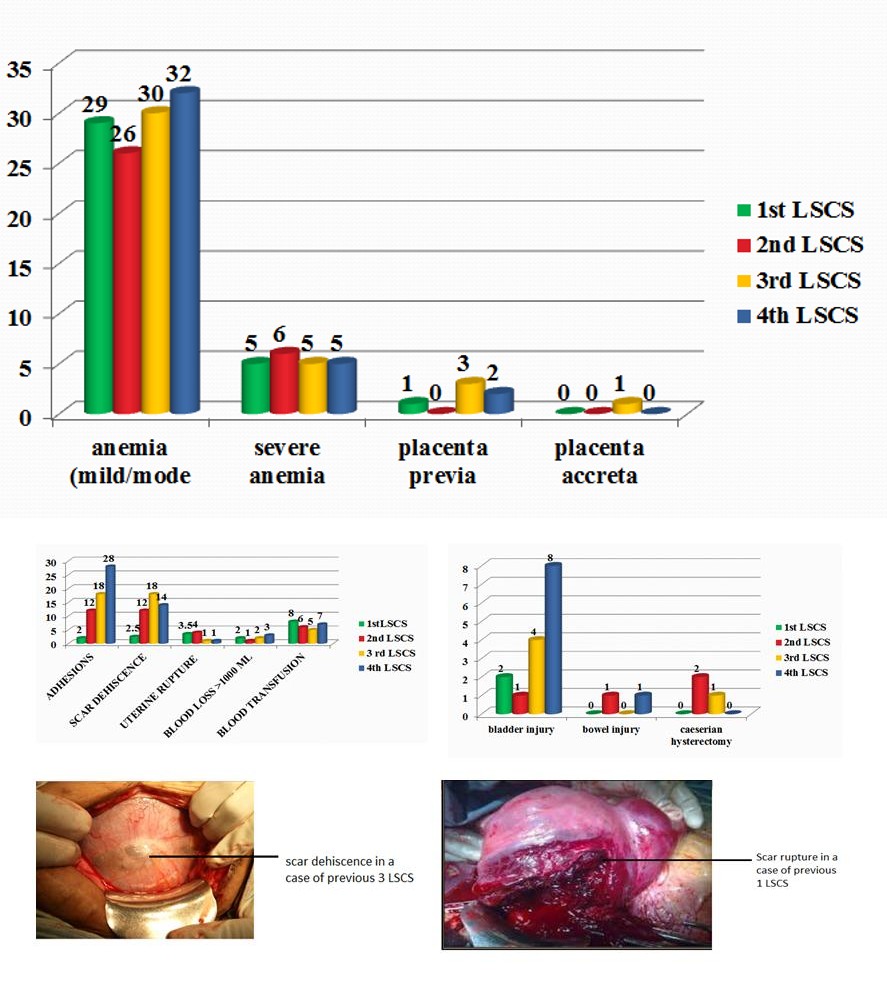
Graph 2: Preoperative complications.
The most common post operative complications are in decreasing order are anaemia, UTI, LSCS wound gape, due to prolonged need for catheterization (Figure 1).
Figure 1a: Intraoperative complication.
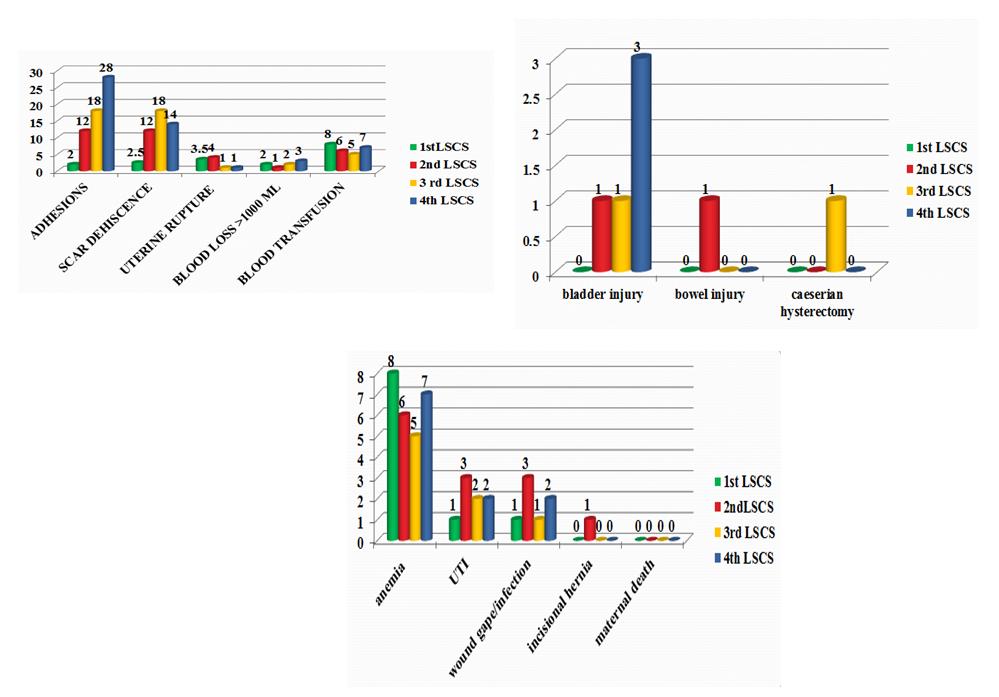
Figure 1b: Postoperative complications.
The average operative time increases with the order of number of previous LSCS, also does the post operative hospital stay.
Previous LSCS cases mostly necessitates the use of higher transverse incision on the uterus due to firmly adherent bladder. Dense adhesions were separated by sharp dissection with great surgical skills in our institute, with minimal number of bladder injuries and almost negligible bowel injuries (Table 5).
| 2nd | 3rd | 4th | v | P | e | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | st LSC | S | |||||||||||||
| LSCS | LSCS | LSCS | alu | ||||||||||||
| Avg operative time | 45 min | 50.6 min | 63 min | 70 min | <0.05 | ||||||||||
| Avg Hospital stay(days) | 5 | 4 | 4.5 | 5 | >0.05 |
Table 6: Operative time & hospital stay.
As the order of number of LSCS increases, tubal ligation may not be possible due to intra-operative Adhesions. In our study, 22%-30% cases had scar thickness of less than 3mm at term. With increasing in the order of LSCS, caesarean section is commonly done at less than 37 completed weeks. Hence there is increase in fetal morbidity with view of less average fetal weight, low APGAR score and NICU admission (Table 6).
| TL | 2nd LSCS | 3rd LSCS | 4th LSCS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Done | 8 | 19 | 29 | ||||||||
| Not Done | 42 | 31 | 17 |
Table 5: TL done.
In our study, 22%-30% cases had scar thickness of less than 3mm at term.
With increasing in the order of LSCS, caesarean section is commonly done at less than 37 completed weeks. Hence there is increase in fetal morbidity with view of less average fetal weight, low APGAR score and NICU admission (Table 7).
| 1st | 2nd | 3rd | 4th | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P | valu | e | |||||||||||||
| LSCS | LSCS | LSCS | LSCS | ||||||||||||
| Avg GA | 39.3 | 38 | 37.3 | 37.1 | >0.05 | ||||||||||
| Preterm <37 wks | 1 | 2 | 1 | 3 | >0.05 | ||||||||||
| Birth Weight | 3.2kg | 2.8kg | 3.1kg | 2.6kg | >0.05 | ||||||||||
| Apgar <7 at 1 min | 4 | 3 | 0 | 1 | 0.05 | ||||||||||
| NICU Admission | 3 | 2 | 1 | 2 | >0.05 | ||||||||||
| Neanatal Death | 0 | 1 | 0 | 0 | >0.05 |
Table 7: Fetal Outcome.
Discussion
In our study, total 200 cases were included in 4 groups (50 cases in each group) with increasing number of caesarian deliveries.
These groups were compared on the basis of various factors like scar dehiscence/rupture, placenta previa, placenta accreta, intraoperative adhesions, injury to bladder/bowel/ureter, need of hysterectomy, blood transfusion, need of ICU admission, postpartum complications, fetal outcome etc. The incidence of anemia was comparable in each group.
- In group 1, 1 case had placenta previa;
- In group 2 none;
- In group 3, 3 cases had placenta previa and
- In group 4, 2 cases had placenta previa. Whereas placenta accreta was present in only 1 case of group 3.
The incidence of placenta previa was higher in women with previous caesarean section as compared to those with no previous uterine scar. There is a strong association between occurrence of placenta previa/accreta and increasing number of caesarian sections. This has been proved in multiple studies like Silver [4] and Qublan, et al. [5].
One of the studies done by Katke RD, showed increasing parity increases risk of placenta previa, Para 1 or more were 100% in scarred uterus and 72% in unscarred uterus [6, 7]. In the study it was found that the incidence of emergency caesarian sections were higher in group 1 & 2, and elective caesarian sections were higher in group 3 & 4.
In our study, on analyzing, the incidence of scar dehiscence and scar rupture, there correlation with the increasing number of caesarian sections was found to be statistically insignificant. This is in contrary to the study by Qublan, et al. in 2005 [5] which reported increase in the incidence of uterine scar rupture with increasing number of caesarian deliveries [4].
With the increasing number of caesarian sections, the occurrence of intraoperative adhesions increased. Most common adhesion was between uterus and bladder (dense) followed by uterus and bladder (loose), uterus and omentum, uterus and anterior abdominal wall and the least was between uterus and the bowel. With each successive caesarian delivery, the percentage of affected women and adhesion severity increases.
The study shows that the incidence of bladder injury increases with increasing incidence of caesarean deliveries. This is consistent with studies by Qublan, et al. in 2005 [5] and silver in 2006 [4]; risk of injury to bladder, bowel, ureter as well as risk of hysterectomies increase with subsequent caesarean sections as per most of the studies but in our study no such correlation was found [5]. It seems to be mainly because of the surgical expertise in a tertiary care centre like our institute.
Although occuring infrequently, rates of cystotomy and bowel injury are also increased. Also in the current study and in most other studies, the amount of blood loss, the need of blood transfusion, operative time, duration of hospital stay, postoperative complications; all these increase with the increasing number of caesarian deliveries.
Tubal ligation as a method of contraception was accepted by more cases in group 3 & 4. According to the present study, no significant difference was found in the Apgar score of delivered babies, NICU admissions, and perinatal morbidity in the 4 groups [8]. This is in agreement to various studies like Qublan, et al. [5], Rashid, et al. [8], Uygur, et al. in 2005.
As per the LSCS audit in a tertiary care centre Mumbai, a study done by Katke RD, the most common cause for NICU admission was LBW accounting for 30.6% cases followed by respiratory distress accounting for 27.3% [7]. When early perinatal morbidity compared with indication and high risk factor, they found neonatal morbidity is high in fetal distress, PROM, PIH, postdatism and multiple pregnancy group. So we suggest early intervention and effective management in these 5 groups can help in reducing perinatal morbidity and mortality thus reducing rate of LSCS in a primigravida.
Conclusion
The incidence of Caesarian section is increasing worldwide. Till now the incidence of higher order caesarians like previous 3 or 4 is low, but is bound to increase owing to the injudicious use of caesarian sections. Our study data shows a significant increase in maternal morbidity with an increasing number of cesarean sections.
Morbidity in the form of increased incidence of adherent placenta, increased blood loss, increased incidence of scar dehiscence/rupture, intraoperative adhesions, injury to bladder/ureter, increased requirement of hysterectomy, postoperative complications, requirement of ICU admissions, have been noted.
Primary prevention in the form of reduction in the rate of primi caesarean section must be done in order to prevent likelihood of placenta previa in scarred uteri. A meticulous approach is required in these cases as there is higher range of maternal morbidity and mortality.Such patients should be referred to tertiary care centres where good surgery expertise, intensive care units and good anaesthetic set up is available.
The emphasis should be on institutional delivery in a tertiary care centre with multidisciplinary care i.e. involvement of senior obstetrician, neonatologist, sinologist and haematologist. In cases of placenta previa or placenta accreta early diagnosis by ultrasound and planned delivery should be the goal. Many problems can be overcome by identifying the patient at risk, antenatal treatments of comorbidities (like anaemia), early admission, planned surgery and these patients should be delivered in well equipped centre with availability of neonatal unit, blood banks, and surgical expertise required. References
1. Katke Rajshree (2015) Changing Trends in Indications of Lower section Caesarean Section (LSCS) over a Decade in a Tertiary Care Centre: An Institutional Study. Journal of Radiology Case Reports.
2. Gilliam M, Rosenberg D, Davis F (2000) The
likelihood of placenta praevia with greater number of caesarean deliveries and higher parity. Obstet Gnecol 99(6): 976-980.
3. Gielchinsky Y, Rojansky N, Fasouliotis SJ, Ezra Y
(2002) Placenta accrete-summary of 10years: A survey of 310 cases. Placenta 23(2-3): 210-214.
4. Silver (2006) Multiple repeat caesarian deliveries.
Obstet Gynecol 107: 1-12.
5. Qublan HS, Tahat Y (2005) Multiple caesarian sections. The impact on maternal and fetal outcome. Saudi Med J 27(2): 210-214.
6. Katke RD (2016) Placenta previa: outcomes in scarred and unscarred uterus. Int J Reprod Contracept Obstet Gynecol 5(8): 2728-2732.
7. Katke RD, Zarariya AN, Desai PV (2014) LSCS audit in tertiary care centre in Mumbai: to study indications and risk factors in LSCS and its effect on early peri-natal morbidity and mortality rate. Int J Reprod Contracept Obstet Gynecol 3(4): 963-968.
8. Rashid M, Rashid RS (2004) Higher order repeat caesarian sections: how safe are five or more? BJOG 111(10): 1090-1094.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’