Myomectomies of 65 Fibroids with Preservation of Uterus in a Nulligravida with Minimally Invasive Incision-A Rare Case with Review of Literature
Uterine fibroids are benign neoplastic growth arising from the myometrium, with estimated incidence being 20-40%. They are a major cause of morbidity in women of reproductive age group. The gold standard diagnostic modality for uterine fibroids appears to be gray-scale ultrasonography, with magnetic resonance imaging being a close second option in complex clinical circumstances. The management of uterine fibroids can be approached medically, surgically, and even by minimal access techniques. Here we are reporting a case of myomectomy with removal of 65 fibroids and conserving the uterus for future fertility.
Introduction
Uterine leiomyoma or fibroids are benign tumours of the uterus made up of smooth muscle and the extracellular matrix proteins collagen and elastin. They are exceptionally common in reproductive age group; the cumulative incidence of a diagnosis of fibroids in women aged 25 to 45 years is approximately 30percent. These leiomyomas undergo various kinds of degeneration. Degeneration in a leiomyoma is basically a result of loss of blood supply. Hyaline, cystic and fatty degeneration that occur in central areas are of no clinical significance and are caused by diminished vascularity in large fibromyomas [1].
Most of the fibroids remain asymptomatic. However they may present as Menorrhagia, Infertility, Recurrent pregnancy loses, Pressure symptoms, Lower abdominal pain, and backache. There are different management approaches for myomas. Surgical treatments for myomas tend to be invasive and expensive, but they are associated with better quality of life. Operative strategy of myoma is determined according to size, number, and location of the fibroids.
Fibroids represent the most common indication for hysterectomy, accounting for 30percent of hysterectomies in white women and over 50percent of hysterectomies in black women. The cumulative risk of a hysterectomy for fibroids for all women between ages 25 and 45 years is 7percent; for black women, the risk is as high as 20percent.
For women who need their fertility, despite the introduction of new surgical and non-surgical techniques, open myomectomy remains the most likely treatment option, as it appears to increase pregnancy rate for these women. There are also reports of successful pregnancies after multiple myomectomies. The aim of this case report is to show that multiple fibroids, as many as 65, can be effectively removed by following meticulous surgical steps of myomectomy.
Case Report
A, 42 years old nulligravida, came to our outpatient department with complaints of heavy menstrual bleeding since 2-3months. Patient also gave history of distension of abdomen over a period of 6 months. She was married since 4 years and had the complaint of infertility. On examination patient was vitally stable but clinically pale. Systemic examination was within normal limits. On per abdominal examination a mass of 24weeks arising from pelvis was felt. It was firm in consistency, with restricted sidewise mobility, irregular surface. On per speculum examination, cervix appeared taken up. On per vaginal examination mass of 24weeks arising from pelvis was palpated. Cervix was deviated to left side with boggy mass was felt in right fornix. Rest per abdominal findings were confirmed. After laboratory investigations, her haemoglobin was found out to be 6.2g%. Two pints of whole blood was transfused. Other laboratory investigations were within normal limits.
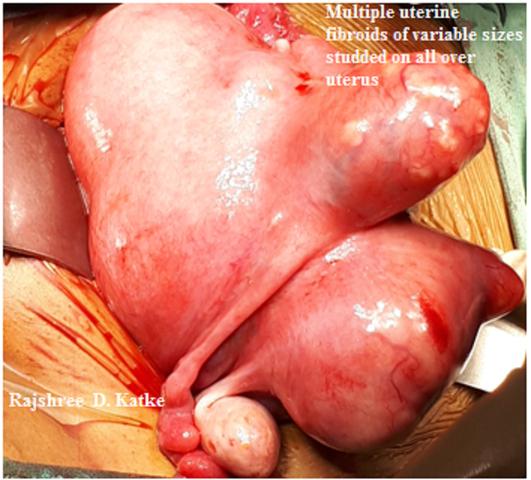
Patient was evaluated for the same. Her Ultrasound report suggested anterior and posterior wall multiple subserosal fibroids measuring 12.2 x10.2cms, 6x4.3cms and posterior submucosal fibroid of 4.1 x3 cm with many small posterior wall intramural fibroid. As the patient was nulligravida, she was posted for myomectomy, keeping the difficulties of multiple fibroids in mind with the consent of sos hysterectomy taken. Minimally invasive small pfannensteil’s incision was taken. Intra-operatively uterus was 24 weeks in size, distorted in shape, Rajshree DK. Myomectomies of 65 Fibroids with Preservation of Uterus in a Nulligravida with Minimally Invasive Incision-A Rare Case with Review of Literature. J Gynecol 2018, 3(3): 000162.
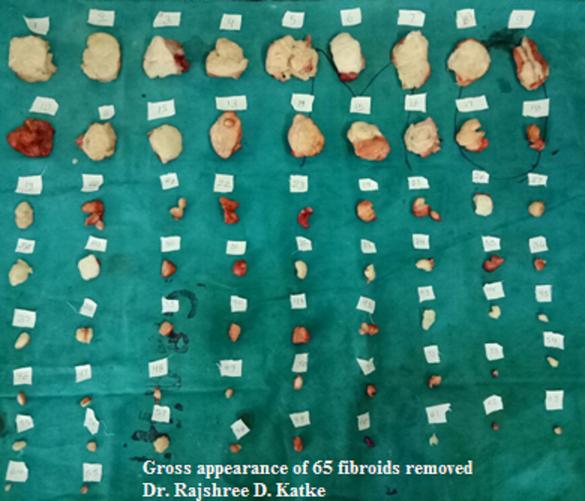
bosselated with multiple uterine fibroids (Figures 1-3). Some of them were very close to the fallopian tubes. Vasopressin infiltration was done. All myomas were removed with skillful surgical techniques with the help of bipolar and unipolar cauterization with 3 big fibroids, largest measuring 12x10cm and smallest measuring 1x1cm. Myomectomy was done with removal of 65 fibroids in total. Uterus was saved with great surgical expertise. Specimen sent for histopathology which was suggestive of removal of 65 myomas from uterus (Figure 4). Patient was transfused with 1 unit of blood intra- operatively. Patient withstood the procedure well with no intra or postoperative complications. Patient was discharged in healthy condition after complete suture removal.


Copyright© Rajshree DK.
Discussion
Leiomyomas arise from overgrowth of smooth muscle and connective tissue of uterus [2]. Myoma may be single or multiple. They develop most commonly in the uterine corpus and much less often in the cervix. The aetiology of leiomyomas in adolescents and adults is generally not Rajshree DK. Myomectomies of 65 Fibroids with Preservation of Uterus in a Nulligravida with Minimally Invasive Incision-A Rare Case with Review of Literature. J Gynecol 2018, 3(3): 000162.
well known but leiomyomas are supposed to grow more in response to both oestrogen and progesterone stimulation, so their prevalence increases throughout the reproductive years and markedly reduced after menopause [3, 4]. Higher concentrations of estrogen and progesterone receptors, as well as aromatase, have been observed in fibroids compared to normal myometrial tissue. Early menarche, exposure to exogenous oestrogen, obesity and pregnancy usually influence fibroid growth.
A genetic component has also been suggested in the pathogenesis of fibroids. High frequency mutations involving chromosomes 6, 7, 12 and 14 have been reported [5]. Many women don’t have any symptom. But when they do, they can often be in conjunction with other causes. Submucosal fibroids may alter the ability of uterus to control menstrual bleeding, leading to prolonged/heavy periods. They can also lead to infertility or miscarriages early in pregnancy. Intramural and Subserosal fibroids typically don’t cause heavy bleeding. However they can grow to the point that they can lead to pressure symptoms, like frequent urination, difficulty in bowel function, lower back pain etc.
The treatment for uterine leiomyomas depends on the patients age and family planning goals as well as tumour size and symptomatology. Asymptomatic leiomyomas can be kept under observation and regular evaluation is required for possibility of elimination of malignant transformation.
Management can be medical, surgical or by other minimally invasive techniques. Medical management consists of Combined Oral Contraceptives, Progestins, Mirena IUD, GnRH Analogues, Selective Estrogen Receptor Modulators, and Selective Progesterone Modulators etc. The minimally invasive methods include Uterine Artery Embolization, MRI guided Focussed Ultrasound Surgery, Radiofrequency Ablation.
Surgical treatments include myomectomy, myolysis and hysterectomy can be employed. Myomectomy is common procedure performed in the reproductive age group with symptomatic leiomyomas, it helps to preserve fertility and doesn’t interfere with hormonal functions and is associated with low recurrence rate [6]. Its approach can be an abdominal, laparoscopic, hysteroscopic, or vaginal. Like other pelvic surgeries, optimum exposure at the operative site is important for myomectomy. Pfannenstiel incision for small uterus and Maylard incision for uterine size that exceeds 12-week Copyright© Rajshree DK.
sized provides adequate exposure.
As more women delay their childbearing for various reasons, an increasing number of women request conservative surgery for fibroid to preserve their reproductive potential as in this case. But sometimes myomectomy may be difficult necessitating hysterectomy in about 1 to 4% due to some reasons related to their location, size and number of fibroid, and experience of gynecologic surgeon. This is much feared complication of myomectomy and affects both for the patient and attending gynecologist particularly when surgery is meant to improve patient’s fertility. Therefore, it is especially important that patient be informed of the possibility that intraoperative findings may contraindicate myomectomy and require that hysterectomy be performed instead.
In this case, even though there were many fibroids in this uterus, we able to remove 65 fibroids successfully. This might be possible through meticulous surgical steps of this procedure and decreasing blood flow to the uterus by taking different measures like use of uterine tourniquet and vasopressin. Tourniquets are safe and inexpensive to use and can be of great benefit when large or multiple intramural fibroid must be removed.
Rajshree DK. Myomectomies of 65 Fibroids with Preservation of Uterus in a Nulligravida with Minimally Invasive Incision-A Rare Case with Review of Literature. J Gynecol 2018, 3(3): 000162.
References
-
Katke RD (2014) Extreme Sequele of Cystic Degeneration of Huge Fibroids Mimicking Like Endometrioma in One Case and Ovarian Neoplasm in Two Cases. The Southeast Asian Journal of Case Report and Review 3(3): 764-779.
-
Katke RD (2016) Large (7.2 kgs) subserosal fibroid with monkenberg’s classification in a postmenopausal women: exremaly rare case with review of literature. Gynecol Obstet Case Rep 2: 2.
-
Lumsden MA (2013) Modern management of fibroids. Obstet Gynaecol Reprod Med 23(3): 65-70.
-
Fields KR, Neinstein LS (1996) Uterine myomas in adolescents: case reports and a review of the literature. J Pediatr Adolesc Gnecol 9(4): 195-198.
-
Ligon AH, Morton CC (2001) Leiomyomata: heritability and cytogenetic studies. Hum Reprod Update 7(1): 8-14.
-
Moroni RM, Vieira CS, Ferriani RA, Reis RM, Nogueira AA, et al. (2015) Presentation and treatment of uterine leiomyoma in adolescence: a systematic review. BMC womens Health 15: 4. Copyright© Rajshree DK.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’