Anti-GnRH Receptor Monoclonal Antibody, GHR106 is First-in-Class GnRH Antagonist
During the last decade, a monoclonal antibody, GHR106 was generated and characterized extensively biologically and immunologically. This antibody targets specific human pan cancer marker and is being evaluated for potential therapeutic applications in cancer immunotherapy and fertility regulations. GHR106 was generated against N1-29 oligopeptide located in the extracellular domains of human GnRH receptor found either in the anterior pituitary or in most of cancer cells. In vitro culture of cancer cells revealed that this antibody can induce apoptosis of cancer cells following 24-48 hours incubations. Anti-tumor activities of GHR106 were evaluated by typical nude mouse experiments in which the effective volume reduction of implanted tumor was observed. Humanized forms of GHR106 were made available in CAR (chimeric antigen receptor) T-cell constructs. GHR106 was shown separately to induce cytotoxic killings of cancer cells in vitro by releasing cytokines following incubations of tumor cells with CAR-T cell constructs. In addition, GHR106 also acts as GnRH antagonist by a specific targeting to pituitary GnRH receptor for reversible suppressions of reproductive hormones. These were demonstrated in “Proof of Concept” rabbit experiments. A single subcutaneous injection with 1-3mg/kg of GHR106 to rabbits of either sex could result in 60 to 90% reductions of gonadotropins, estrogen and/or testosterone over a period of one to two weeks. Based on these preclinical assessments, it can be concluded that GHR106 is restricted in tissue expressions and suitable for cancer immunotherapy. It can also act as long-acting GnRH antagonist to target specifically on GnRH receptor in anterior pituitary for numerous gynecological diseases including ovulation inhibition in IVF/ART, endometriosis-premenstrual syndrome, precocious puberty, uterine fibroids and/or polycystic ovarian syndrome.
Introduction
Origin of GHR106 Monoclonal Antibody
Since the development of hybridoma technology in 1975, numerous monoclonal antibodies were generated mainly from mice for numerous basic research and clinical applications [1, 2]. Compared to the polyclonal antisera, monoclonal antibodies are epitope-specific with defined binding specificity and affinity. Therefore, monoclonal antibodies have been the primary choices for studies of antigen and antibody interactions and for immunodiagnostic and immunotherapeutic applications in biosciences and biotech industry [3]. GHR106 is a monoclonal antibody generated from hybridoma following immunization with N1-29 oligopeptide as the immunogen corresponding to the main extracellular domains of human GnRH receptor [4]. GHR106 was found to be specific to GnRH receptor located in the anterior pituitary and on the surface of many types of cancer cells in humans. GHR106 was evaluated extensively and established as first-in-class GnRH antagonist for potential therapeutic applications in cancer immunotherapy and in fertility regulations [5, 6, 7].
Results and Discussions
GHR106 is Long-Acting GnRH Antagonist
As mentioned, GHR106 was generated against N1-29 oligopeptide corresponding to the extracellular domains of human GnRH (gonadotropin releasing hormone) receptor [4, 7]. During the last decade, this monoclonal antibody has been studied extensively. Besides anterior pituitary, human GnRH receptor is almost universally expressed on the surface of many cancer cells or in reproduction-related peripheral /gonadal tissues including ovary, testis, uterus and placenta [4, 7, 8]. Since two decades ago, expressions of human GnRH receptors in cancer cells were investigated by RT-PCR, indirect immunofluorescence staining and Western blot assays [8]. Among the cancerous tissues studied, the positive staining/expression rate are given as follows: breast (52%), ovary (78-80%), endometrium (77-100%), prostate (86-100%), kidney (80%), brain (43%) and pancreas (57%-
100%) [8].
Functional Studies of GHR106 Interaction with GnRH Receptor in Cancer Cells and Anterior Pituitary
During the past decade, our studies have been focused on the functional aspects of GHR106 binding to human GnRH receptor in vitro and in vivo [5, 9]. Through complete humanization of GHR106, the constant regions of IgG heavy chains and light chains were replaced with those of human origins [9]. Two humanized GHR106 were created, namely GHR106(hIgG1) and GHR106(hIgG4). For applications of cancer immunotherapy, the former with retained effective functions was used, whereas the later reveals only with the binding activities to human GnRH receptor for future drug development as GnRH antagonist. Both were shown to have affinity constant of 3±1nM and circulation half-life of 5±1 days in rabbits, but possibly up to 21 days in humans [9]. Dual functions of known human GnRH receptor are known to exist, depending on tissue origins [4]. GnRH receptor located in the pituitary is known to regulate or control the release of gonadotropins including LH and FSH upon the pulstetile binding interactions of GnRH released from hypothalamus [4, 5].
Proof of Concept Rabbit Experiments
GHR106 was shown to compete with native GnRH for the binding of GnRH receptor [4]. “Proof of concept” experiments in rabbits were conducted to demonstrate reversible suppressions of serum reproductive hormones upon a single subcutaneous injection of (1-3 mg/kg body weight) GnRH106(hIgG4) [10] to rabbits of either sex. Reproductive hormones including gonadotropins (LH) and estradiol (E2) or testosterone (T) were reduced to 80-90% of the normal levels for over a period of one to two weeks. These rabbit experiments to demonstrate reversible suppressions of reproductive hormones were graphically presented in (Figure 1A) and (Figure 1B), respectively. The results of this study revealed that GHR106(hIgG4) may be used as antibody- based GnRH antagonist with similar biological actions to those of decapeptide GnRH antagonist or oral used Elagolix [11, 12]. Therefore, the relatively long-half of this class of GnRH antagonist may be beneficial to the treatments of certain gynecological and fertility related diseases, which are caused by abnormal modulations of human GnRH receptor [1].
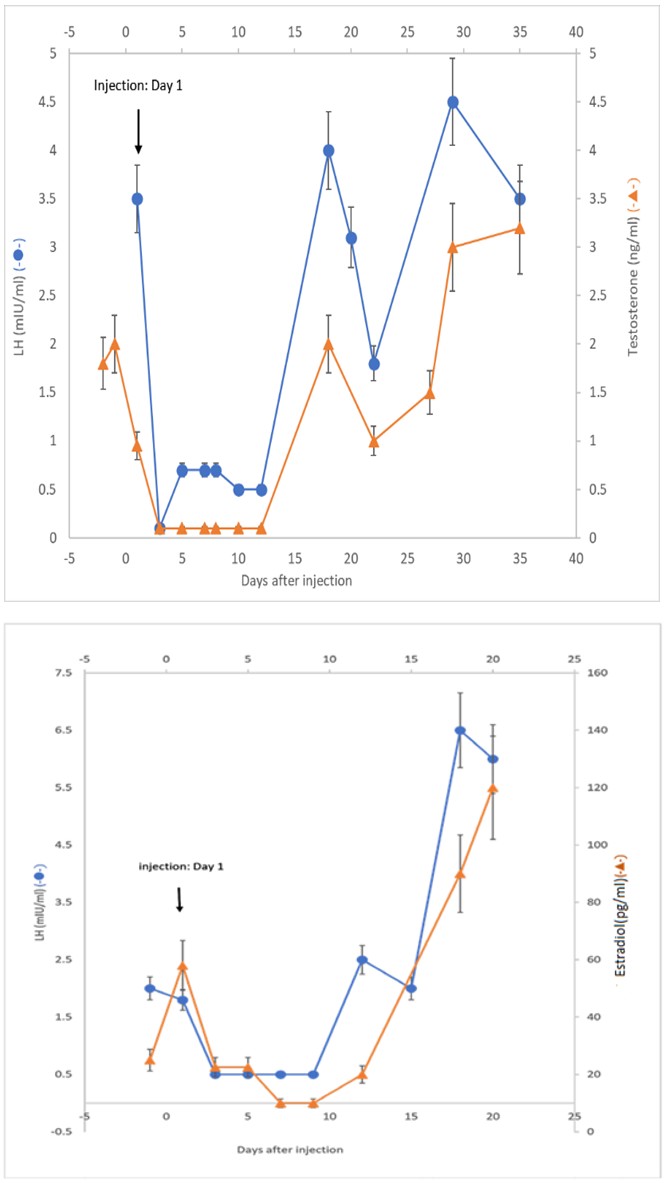
Figure 1A: Hormonal profiles (LH and Testosterone) upon a single sc injection of 3mg/kg of GHR106 (hIgG4).
Figure 1B: Hormonal profiles (LH and E2) upon a single injection of 3mg/kg of GHR106 (hIgG4).
Apoptosis of Cancer Cells Induced by GHR106 for Cancer Immunotherapy
Immunohistochemical staining studies of GHR106 revealed that greater than 90% of human cancer cell lines express surface GnRH receptor [5, 8]. By TUNEL assay, GnRH, Antide (a decapeptide GnRH antagonist) and GHR106 were shown to induce apoptosis of cancer cells to a similar extent.
However, GHR106 has much longer half-life than those of small molecules (e.g. Cerorelix, Elagolix or Relugolix) (days vs. hours). Furthermore, GHR106 was shown to induce complement-dependent cytotoxicity (CDC) reactions as well as other related effector functions to cancer cells in culture [5, 7]. Based on these in vitro functional studies, we believe that GHR106(hIgG4) can be an ideal long-acting GnRH antagonist with effector functions of cytotoxic activities to inhibit growth of cancer cells in vivo for broad applications in cancer immunotherapy.
Potential Therapeutic Applications of GHR106 Monoclonal Antibody
Following extensive preclinical studies of GH106 during the last decade, it was generally concluded that this antibody is a long acting antibody-based GnRH antagonist, compared to those of decapeptides and small molecules available in the market, such as Cetronelix and Elagolix [11, 12].
Basically, GnRH antagonists are primary used in the fields of cancer immunotherapy and fertility regulations. For antibody-based GnRH antagonist, establishment of certified stable permanent cell lines are required to produce this antibody for broad therapeutic applications following regulatory approval by FDA IND enabling within three years.
Cancer Immunotherapy with Applications of GHR106 CAR-T Cell Constructs
CAR-T (Chimeric antigen receptor-transfected T cells) technology has been evolved for new applications in cancer immunotherapy [13, 14]. CD19-CAR-T cells have been initially utilized in the therapeutic treatments of liquid tumors, such as those of blood cell origins [15, 16]. High degrees of remission rates (≥50-90%) were observed for various types of lymphomas following CD19-CAR-T cell treatments [13]. Therefore, GHR106 was introduced in the format of scFv- CAR-T cell constructs to target pan cancer biomarkers in cancer immunotherapy. GHR106(hIgG4) was introduced in a scFv (single chain variable fragments) CAR-T cell constructs for in vitro expansion and co-incubated with culturing cancer cells to induce cytotoxic killing of cancer cells (C33A- cervical origin) [13, 14, 15, 16]. The results of such model study are presented in (Figure 2) for demonstrations.
GHR106 is known to react with human GnRH receptor which is wide spready expressed on the surface of many cancer cells. Therefore, GHR106(hIgG4) may be potentially useful in clinical treatments of many different types of human cancer in various formats (naked, CAR-T or NK- CAR). GHR106 positively stains those human cancer of high incidence. These include those of cervix, endometrium, ovary, lung, breast, prostate and stomach which can predominate as much as 60% of the total clinical market of cancer ($500 billion USD per annum). Therefore, GHR106-based cancer immunotherapy may play a significant role in cancer therapy in the near future [7].
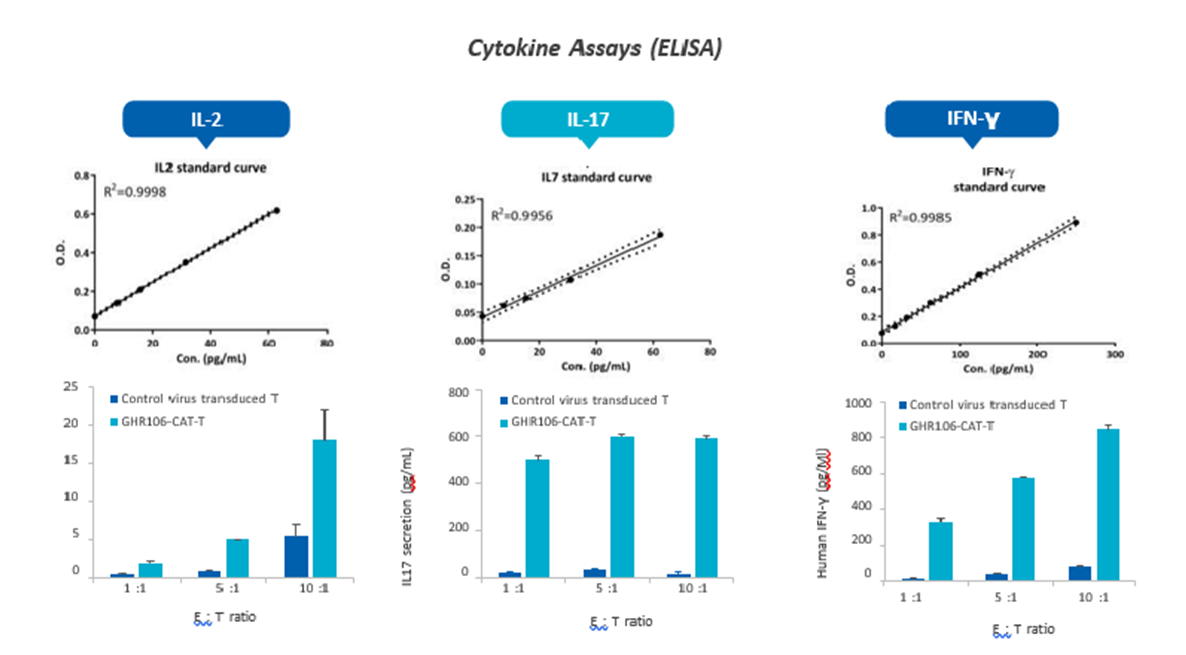
Figure 2: Demonstrations of the lysis of C33A cancer cells (T, target cells) upon co-incubation with hGHR106 (scFv-linked CAR-T cells (E, effector cells) similar to RP215-CAR-T constructs; the cytokine assays were performed with the established ELISA including IL-2 IL-IL7 and IFN-ꝩ. E/T ratios varied from 1:1, 5:1 to 10:1 respectively. Cytokine releases were shown to be GHR106-CAR-T cells dependent in all three cytokines, when compared to the negative control with virus-only-transduced T cells for co-culturing.
Clinical Applications of GHR106 as GnRH Antagonist for Fertility Regulations
Through “Proof of Concept” rabbit experiments, GHR106 has also been established as long-acting antibody-based GnRH antagonist (5-21 days half-life). This is in contrast to the currently available short acting GnRH antagonists (~ hours) of small molecular size such as Cetrorelix (decapeptide) and Elagolix (organic chemical) [11, 12].
As a long-acting antibody-based GnRH antagonist, hGHR106 (IgG4) in humanized forms of IgG4 isotype was introduced [9]. Potential clinical market size for GHR106 (IgG4) as GnRH antagonist for treatments of major gynecological diseases can be as much as 35 billion USD per year globally. As long-acting GnRH antagonist, hGHR106 (IgG4) introduced in this review can be used for treatments of any of the following indications in gynecological diseases: (i) Inhibition of spontaneous ovulation in ART, (ii) Endometriosis, (iii) Uterine fibroids, (iv) Precocious puberty, (v) Premenstrual syndrome and/or (vi) Polycystic ovarian syndrome. Therefore, we believe that antibody-based long- acting GnRH antagonist can be a good alternative to currently available ones in the clinical market.
References
-
Kohler G, Milstein C (1975) Continuous culture of fused cells secreting antibodies of predefined specificity. Nature 256: 495-497.
-
Davis JM, Pennington JE, Kubler AM, Conscience JF (1982) A simple single-step technique for selecting and cloning hybridomas for production of monoclonal antibodies. J Immunol Methods 50(2): 161-171.
-
Jain M, Kamal N, Batra KS (2007) Engineering antibodies for clinical applications. Trends in Biotechnol 25(7): 307-316.
-
Lee CY, Ho J, Chow SN, Yasojima K, Schwab C, et al. (2000) Immunoidentification of gonadotropin releasing hormone receptor in human sperm, pituitary and cancer cells. Am J Reprod Immunol 44(3): 170-177.
-
Lee G, Ge B (2010) Growth inhibition of tumor cells in vitro by using monoclonal antibodies against gonadotropin-releasing hormone receptor. Cancer Immunol Immunother 59(7): 1011-1019.
-
Lee G (2018) A new monoclonal antibody-based biosimilar GnRh antagonist. J Clin & Experi Immunol 3: 1-3.
-
Lee G, Cheung AP, Ge B, Zhu M, Giolma B, et al. (2012) CA215 and GnRH receptor as targets for cancer therapy. Cancer Immunology and Immunother 61(10): 1805- 1817.
-
Nagy A, Schally AV (2005) Targeting of cytotoxic gonadotropin releasing hormone analogs to breast, ovarian endometrial and prostate cancers. Biol Reprod 73(5): 851-859.
-
Lee G, Huang C-Y, Ge B (2014) Two distinct humanized monoclonal antibodies for immunotherapy of ovarian cancer J. Cancer Sci and Therapy 6(4): 110-116.
-
Lee G (2022) “Proof of Concept” rabbit experiments demonstrating GHR106 (hIgG4) as GnRH antagonist. Int. J Zoo and Animal Biol 5(2): 1-9.
-
Ezzati M, Carr BR (2015) Elagolix, a novel orally bioavailable GnRH antagonist under investigation for treatment of endometriosis-related pain. Women’s Health 11(1): 19-28.
-
Osuga Y, Seki Y, Tanimoto M, Kusumoto T, Kudou K, et al. (2021) Relugolix, an oral gonadotropin-relating hormone (GnRH) receptor antagonist, in women with endometriosis-associated pain: phase 2 safety and efficacy 24-weeks results. BMC Women’s Health 21(1): 250.
-
Maude SL, Teachey DT, Porter DL, Group SA (2015) CD19-targeted chimeric antigen receptor T cell therapy for acute lymphoblastic leukemia. Blood 125(26): 4017-4023.
-
Yu S, Li A, Liu Q, Li T, Yuan X, et al. (2017) Chimeric antigen receptor T cell: a novel therapy for solid tumors. J Hemato Oncol 10(1): 78.
-
Posey AD, Schwab RD, Boesteanu AC, Steentoft C, Mandel U, et al. (2016) Engineered CAR-T cells targeting the cancer-associated Tn-Glycoform of the membrane Mucin MUC1 control adenocarcinoma. Immunity 44(6): 1444-1454.
-
Mirzaei HR, Rodriguez A, Shepphird J, Brown CE, Badie B, et al. (2017) Chimeric antigen receptor T cell therapy in solid tumor challenges and clinical applications Front. Immunol 8: 1850.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’