Case Series of Peritoneal Tuberculosis with Three Different Presentations
Tuberculosis is an emerging medical challenge in each and every part of the world which affects all most all parts of the body even though the commonest presentation is pulmonary tuberculosis. Peritoneal tuberculosis will lead to fibrosis and scarring of the intra-peritoneal organs while producing ascites. This is a case series of peritoneal tuberculosis which presented in three different ways.
Introduction
Tuberculosis (TB) is a major health challenge with 10.6 million affected people across the globe in 2021. This is an increment of 4.5% compare to 2020 [1]. Highest prevalence of TB was reported from India (28%), Indonesia (9.2%), China (7.4%), Philippines (7.0%) and Pakistan (5.8%) [2]. Even though the pulmonary TB is the commonest form, prevalence of extra-pulmonary TB is rising throughout the world making a significant challenge to health sector. This is more common among females compare to males while the genital tract is being more vulnerable to the infection [3, 4]. Genital tract TB ultimately lead to scarring due to fibrosis of tube which ended up with tubal factor subfertility [5].
Miliary tuberculosis (MTB) is a result of wide spread dissemination of the mycobacteria throughout the body which accounts for 1-2% of all extra pulmonary TB [6]. Poor socio-economic status, female gender, immunosuppressed state, alcoholism and extremes of age are the risk factors for the MTB [7, 8, 9]. Bacilli enters into the peritoneal cavity through hematogenous spread from a lung focus or rarely through the diseased bowel to cause peritoneal tuberculosis (PTB) [10]. Risk factors for PTB are HIV infection, diabetes mellitus, treatment with anti-tumor necrosis factor (TNF) agents, ongoing peritoneal dialysis and hepatic cirrhosis [11]. Patient may present with pyrexia of unknown origin (PUO), abdominal distention due to ascites and abdominal pain [6].
Case 1
51-yeal old mother of three children, underwent total abdominal hysterectomy (TAH) and bilateral salpingectomy 8 months ago due to symptomatic fibroid uterus. The surgery was a straight forward one and there were no extensive tissue dissections. She had uneventful recovery after the surgery. Histology report confirmed the pre-operative diagnosis of fibroid uterus and excluded the malignancy. Her liver, renal and cardiac function were normal during the pre-operative investigations. She re-admitted to the ward, eight months later with one-week history of progressive abdominal distention, abdominal pain and feverish feeling. She had shortness of breath, but denied any history of chronic cough. She didn’t have loss of appetite, loss of weight, evening pyrexia or contact history of known TB infected person. Her urine output remained normal following the surgery.
Her abdomen was tense due to gross ascites even though there were no any significant tenderness. She didn’t have documented fever. She didn’t have cervical lymphadenopathy. Air entry of the bilateral lung fields were reduced.
Ultra sound scan (USS) of the abdomen confirmed the presence of gross ascites with diffuse omental thickening. There was no para aortic lymphadenopathy. Both ovaries were normal. There were no any abdomino-pelvic masses.
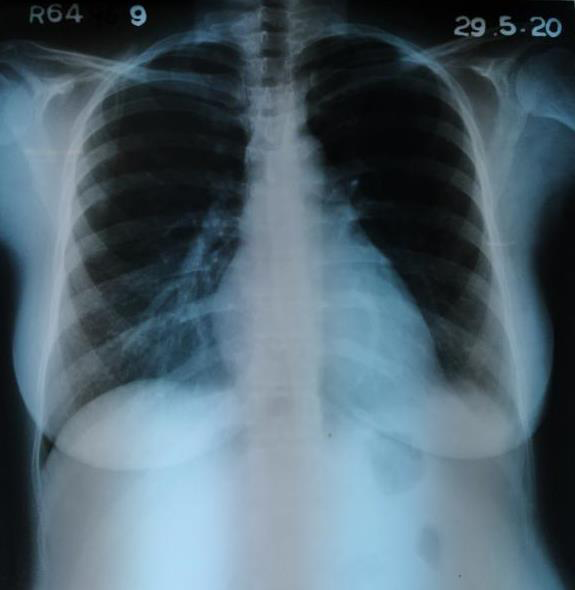
Her full blood count and C-reactive protein level were normal. Her chest X-ray showed bilateral mild pleural effusions (Figure 1). Summary of the investigation results are as follows (Table 1).

| Investigation | Results |
| White blood cells (WBC) | 7200/ul |
| Hemoglobin | 12.4g/dl |
| Platelet | 410000/ul |
| C-reactive protein | 4ng/ml |
| Blood urea, serum creatinine | Within normal range |
| Serum sodium, potassium and chloride | Normal |
| AST, ALT, ALP | Normal |
| Total protein | 7.0g/dl |
| Albumin | 3.2g/dl |
| Globulin | 4.0g/dl |
| Total and direct bilirubin | Normal |
| ESR | 54mm/first hour |
| CA 125 | 25 iu/ml |
| Dengue NS1 antigen | Negative |
| Dengue antibody | Negative |
| Blood picture | Reactive picture |
| Blood culture and urine culture | No growth |
| Ultra sound scan of the abdomen and pelvis | Gross ascites with thickened omentum |
| Echo cardiogram | Normal |
| Peritoneal fluid aspiration results | |
| WBC | 1200/ml |
| Mononuclear cells | 90% |
| Polymorphonuclear cells | 10% |
| Glucose | 53mg/dl |
| Lactic dehydrogenase | 360u/l |
| Protein | 5.59g/dl |
| Culture | No bacterial growth/ TB culture results pending |
| Results pending | |
| TB PCR (polymerase chain reaction) | Negative |
| Staining for acid fast bacilli (AFB) | |
| Mantoux test done | Positive |
| Chest X-ray | Bilateral pleural effusions |
| Sputum for AFB | Negative |
Table 1: Summary of the investigation results.
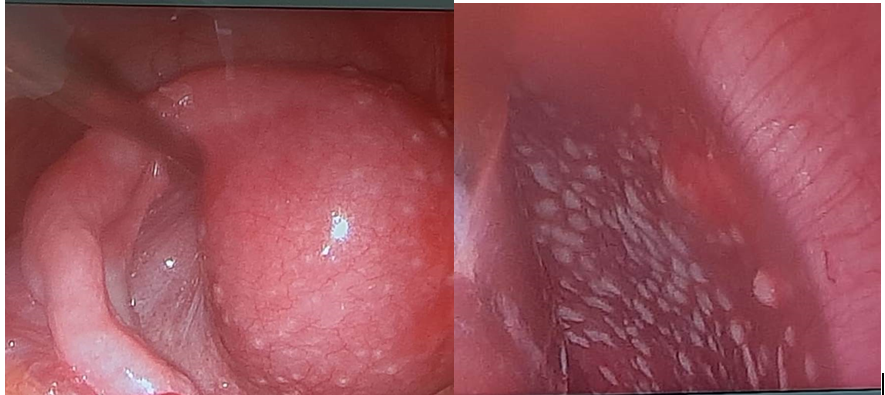
As all these investigation results pointed towards the diagnosis of PTB, decision was taken at the multi-disciplinary team meeting to go ahead with diagnostic laparoscopy. Laparoscopy confirmed the USS findings. Other than that, she had diffuse miliary deposits all over the peritoneum, omentum, bowel surface, liver surface, under surface of the diaphragm, bladder surface and pouch of Douglas (Figure 2).
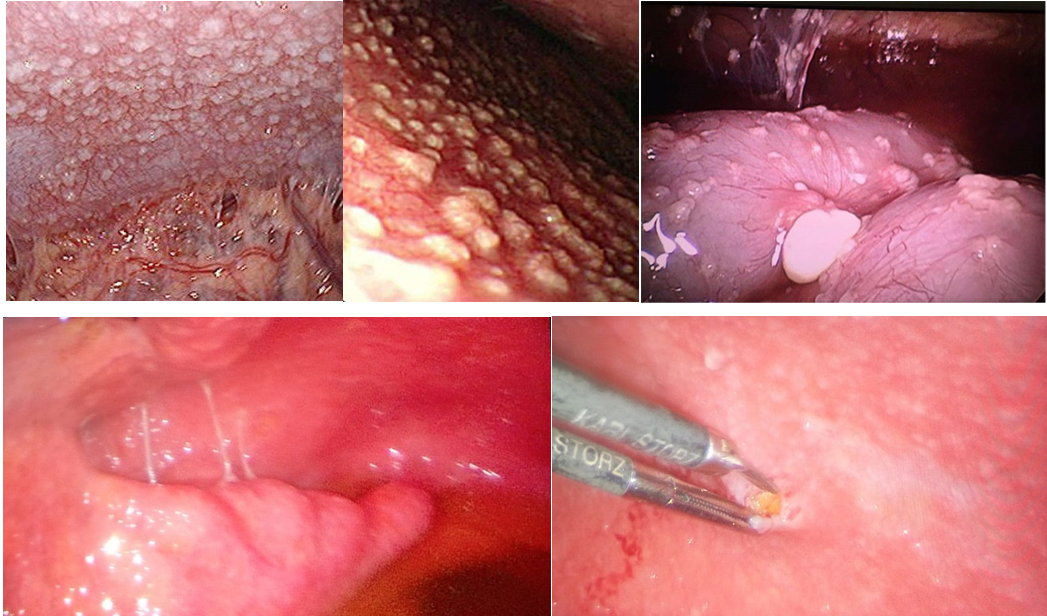
Multiple biopsies taken from the miliary deposits and sent for histology and TB culture. She was started on anti- TB therapy while confirmatory test results are pending. Her symptoms gradually settled. Her histology reports showed granuloma formation with central caseous necrosis suggestive of TB.
Case 2
25-year-old nulliparous lady presented with primary subfertility for 2 years. She got married 2 years ago and had tried for a baby from there onwards. She was otherwise healthy and had regular menstrual cycles without dysmenorrhea or menorrhagia. Her husband was a healthy person and they had regular vaginal sexual intercourse throughout their marriage life. She denied any history of dyspareunia, erectile dysfunction or premature ejaculation.
On examination she was a small built lady with a body mass index of 19kg/m2. She was afebrile. Her abdominal examination was unremarkable. Speculum examination revealed edematous and inflamed cervix. Bimanual examination was unremarkable. Retrospective questioning revealed that she had one episode of intermenstrual bleeding and post coital bleeding in last week which she neglected. She never had cervical screening before and denied any past history of sexual promiscuity.
Her husband’s seminal fluid analysis was normal. She had undergone three cycles of ovulation induction with timed sexual intercourse without any success. As she never had previous tubal patency assessment, she was agreed to undergo laparoscopy and dye test.
Laparoscopy revealed edematous and inflamed uterus and tubes with whitish papular plaques which suggestive of miliary tubercles. These miliary tubercles were present all over the pelvic organ surfaces, pouch of Douglas, bowel surfaces, liver surface, under surface of the diaphragm and parietal peritoneum. Small amount of straw-colored free fluid noted in pouch of Douglas. Dye test was not performed. Peritoneal fluid and multiple biopsies were taken from the miliary deposits. They were sent to TB PCR (polymerase chain reaction), culture, histology and direct smears for acid fast bacilli (AFB). Multiple punch biopsies were taken from the cervix and endometrial sampling was done. She had uneventful recovery following the surgery (Figure 3).
Retrospective inquiry revealed that she had generalize body weakness, lethargy, feverish feeling towards the latter part of the day and loss of appetite which she attributed for her stressful status due to recent changes in life style as a result of change in the job. She denied any past history suggestive of pulmonary TB or expose to a patient who had pulmonary TB. Examination did not elicit any signs of pulmonary TB.
Her chest X-ray was normal and three samples of sputum for AFB were negative. Her ESR (erythrocytes sedimentation rate) was 85mm for the first hour. Her Mantoux test was strongly positive. TB PCR came positive from all samples taken during the surgery. Histology revealed granuloma formation with caseous necrosis which suggestive of TB. Peritoneal fluid was negative for AFB. Her culture reports came later as positive for TB.
She was counselled regarding the findings and investigation results and she was started on anti-TB treatment. She had significant clinical improvement thereafter and she was advised to delay the pregnancy until she finishes the treatment course.
Case 3
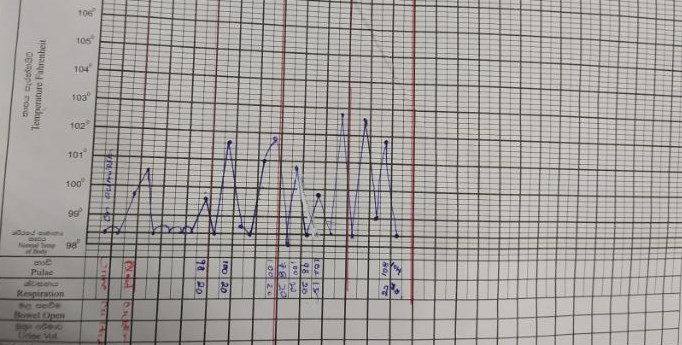
30-year-old lady who was a mother of 3-month- old, breast fed, vaginally delivered child presented with progressive abdominal fullness and intermittent fever for the last 2 months. She was apparently well up to fourth postpartum week until she notices gradually worsening abdominal fullness associated with intermittent fever, loss of appetite and loss of weight. She didn’t have any features suggestive of urinary tract, genital tract, respiratory tract or gastro intestinal tract infections. She denied any past contact history of TB. Her ovaries and uterus were said to be normal during antenatal ultrasonography. She didn’t have any significant past medical history even though she had undergone appendectomy five years ago. Her pregnancy and delivery were uncomplicated and her menstruation had not started. She denied any family history of malignancies.
Her abdomen was symmetrically enlarged and there were no organomegaly. She had flank dullness and shifting dullness which suggestive of ascites. Her pelvic examination was normal. She had been treated with multiple antibiotics during last few weeks without any clinical improvement (Table 2) (Figures 4 & 5).
| Her investigation results are as follows. | |||
| Investigation | Results | ||
| White blood cells (WBC) | 8830/ul | ||
| Hemoglobin | 10.4g/dl | ||
| Platelet | 479000/ul | ||
| C-reactive protein | 223ng/ml | ||
| Blood urea, serum creatinine | Within normal range | ||
| Serum sodium, potassium and chloride | Normal | ||
| AST, ALT, ALP | Normal | ||
| Total protein | 7.3g/dl | ||
| Albumin | 3g/dl | ||
| Globulin | 4.3g/dl | ||
| Total and direct bilirubin | Normal | ||
| ESR | 80mm/first hour | ||
| CA 125 | 285 iu/ml | ||
| Dengue NS1 antigen | Negative | ||
| Dengue antibody | Negative | ||
| Blood picture | Reactive picture | ||
| Blood culture and urine culture | No growth | ||
| Ultra sound scan of the abdomen and pelvis | Gross ascites with normal abdomino-pelvic organs. | ||
| Computerized tomography scan | Gross ascites and small pleural effusion | ||
| Echo cardiogram | Normal | ||
| Peritoneal fluid aspiration results | |||
| WBC | 1310/ml | ||
| Mononuclear cells | 90% | ||
| Polymorphonuclear cells | 10% | ||
| Glucose | 95mg/dl | ||
| Lactic dehydrogenase | 382u/l | ||
| Protein | 5.26g/dl | ||
| Culture | No bacterial growth/ TB culture results pending | ||
| Results pending | |||
| TB PCR (polymerase chain reaction) | Negative | ||
| Staining for acid fast bacilli (AFB) | |||
| Mantoux test done | positive | ||
| Chest X-ray | Normal | ||
| Sputum for AFB | Negative |
Table 2: Summary of the investigation results.
Multi-disciplinary team (MDT) meeting was arranged and decided to proceed with diagnostic laparoscopy as the possibility of peritoneal TB was high and results of confirmatory tests were pending while patient was suffering due to the symptoms. Diffuse, small (less than 1cm) whitish tubercles noted all over the parietal peritoneum, uterine surface, tubal surface, pouch of Douglas, bowel, liver surface and undersurface of the diaphragm during the diagnostic laparoscopy. Straw colored ascites was noted. Ovaries and other abdomino-pelvic organs didn’t demonstrate any features suggestive of malignancy. Multiple biopsies were taken from those lesions and sent for TB culture and histology.
These laparoscopy findings were discussed in detail during next MDT meeting and decided to treat as PTB and anti TB drug therapy was started. Her 3 months old baby was investigated by neonatology team for TB and found to be non-infected. Her fever settled after 48 hours of starting treatment and her all constitutional symptoms gradually settled. TB PCR was positive and histology confirmed the presence of granuloma formation with caseous necrosis which suggestive of TB. Her culture report came later as positive for Mycobacterium tuberculosis. She completed her treatment course and fully recovered from the disease.
Discussion
As this first patient presented following hysterectomy, possible occult urinary tract injuries should be excluded as they may present with free fluid in the abdomen. But in this case, she was totally normal after surgery for 8 months without any symptoms and she presented with an acute history. If a patient is having an undiagnosed urinary tract injury during a hysterectomy, she should be unwell after the surgery. Other thing is as ovaries were preserved during surgery, carcinoma of the ovary and primary peritoneal cancer should be born in mind even though ultrasonically ovaries were normal.
Generally speaking, the second patient’s diagnosis of PTB and genital tract TB was an incidental one. But this could have been detected earlier if she was conscious about the changes in her general health. Post-coital bleeding and intermenstrual bleeding she had could have alert the physician to find out about the cervical pathology. As she was in very young age, possibility of cervicitis is more than the possibility of malignant cause. Compare to other two cases she didn’t have gross ascites. This may be due to early incidental identification of the problem before she manifests the symptoms.
Diagnosis of the third patient is more challenging compare to the other two as she presented in her post- partum period with PUO (pyrexia of unknown origin). Physicians tend to think about obstetrics related causes for fever rather than general medical causes. Other fact is child screening is an essential part in the management of the third case as we don’t know the exact time of origin of this disease.
Generally speaking diagnostic laparoscopy played a crucial role in all these three cases to confirm the diagnosis while ultrasound scan and peritoneal fluid analysis (except in second case) support towards the narrowing down of differential diagnoses. All three cases highlighted the importance of the trial of anti TB therapy without waiting for the confirmatory test results. Following table shows a general comparison between these three cases of PTB (Table 3).
| Case 1 | Case 2 | Case 3 | |
|---|---|---|---|
| Presentation time and age | After an TAH | Incidental | Post-partum period after a vaginal delivery. (30 year) |
| (51year) | (25year) | ||
| Main symptoms | Abdominal distention | Primary subfertility | PUO and abdominal distention |
| Features of Pulmonary TB | Pleural effusions, Shortness of breath | No | No |
| Constitutional symptoms | Feverish feeling | Generalized body weakness, lethargy | Loss of appetite, loss of weight, PUO |
| Chest X ray | Pleural effusion | Normal | Normal |
| Mantoux test | Positive | Positive | Positive |
| ESR (mm/1st hour) | 54 | 85 | 80 |
| Sputum for AFB | Negative | Negative | Negative |
| Peritoneal fluid analysis | Supported in diagnosis. But culture negative. | Not done. | Supported in diagnosis. But culture negative. |
| Role of laparoscopy | Helped to confirm the diagnosis and allowed to take tissue samples | Helped to confirm the diagnosis and allowed to take tissue samples | Helped to confirm the diagnosis and allowed to take tissue samples |
Table 3: Comparison between three patients.
PTB contributes to 4.9% of extra pulmonary TB cases while being in the sixth commonest site to have extrapulmonary TB [12]. All these cases show the importance of taking a comprehensive history and examination in a patient without limiting to common possible diagnosis. Sametime it shows the importance of considering tuberculosis as a cause for gross ascites in a setting where the prevalence is high.
As only one third of PTB patients shows clinical and radiological signs of pulmonary TB (even though it is the commonest site), it becomes a diagnostic challenge to the physicians [13]. Even though it was not done in this second patient, peritoneal fluid analysis can support in the diagnosis of PTB as 68% of the patients are having lymphocytic predominant WBC containing (500-1500/mm3) ascites with protein contain >2.5g/dl [14]. Radiological findings of these PTB patients are lymphadenopathy (14-47%), loculated or localized ascites (36-67%) and peritoneal thickening (23-32%) [15]. Sensitivity of Ziehl-Neelsen stain of ascetic fluid (0-6%) and culture of the ascetic fluid (16-58%) can be increased by centrifuging the sample [10]. TB PCR from ascetic fluid has high specificity and low sensitivity. But Adenosine deaminase level in peritoneal fluid (>30iu/L) is highly suggestive of TB (sensitivity close to 100% and specificity 95%) [14]. Even though supporting in diagnosis, performing Mantoux test will not differentiate between latent TB and active TB. Even though the culture is the gold standard in diagnosing TB, negative culture will not exclude the disease. Consumption of prolong time for the reporting is the most problematic thing in culture. Value of laparoscopy come into the picture in these occasions which allows the physician to directly visualize the peritoneal cavity while allowing to obtain samples. Three different characteristic laparoscopic appearances are as follows [16].
- substantial peritoneal thickening with dense adhesions that may extend to adjacent organs
- thickened peritoneum with yellow-white tubercles
- thickened peritoneum without tubercles If the diagnosis is not obvious with the available investigation results and clinical findings, trial of anti-TB therapy is justifiable in a case with high index of suspicion. In this case it was not so and anti TB therapy for twelve months will settle the problem.
Conclusion
Even though rare, peritoneal TB should be born in mind when dealing with a woman presented with gross ascites without any obvious evidence of liver or renal failure, as early diagnosis and proper treatment reduce the morbidity and mortality. Peritoneal fluid may assist in narrow down the differential diagnoses. Diagnostic laparoscopy plays a crucial role in diagnosis process. Trial of anti-TB therapy is a good option after discussion with expertise, which helps to prevent the delay in starting treatment.
Conflict of Interest
No conflict of interest.
Funding
No funding
Consent
Informed written consent obtained from the patient.
References
-
Kishwar N, Rauf B (2023) Role of genital tuberculosis in sub-fertile women. Khyber Med Univ J 15(1): 49-54.
-
WHO (2022) Global tuberculosis report 2022. World Health Organization, Geneva.
-
Tahseen S, Khanzada FM, Baloch AQ, Abbas Q, Bhutto MM, et al. (2020) Extra pulmonary tuberculosis in Pakistan - A nation - wide multi center retrospective study. PLoS ONE 15(4): e0232134.
-
Mehraj J, Khan ZY, Saeed DK, Shakoor S, Hasan R, et al. (2016) Extrapulmonary tuberculosis among females in South Asia-gap analysis. Int J Mycobacteriol 5(4): 392- 329.
-
Tzelios C, Neuhausser WM, Ryley D, Vo N, Hurtado RM, et al. (2022) Female genital tuberculosis. Open Forum Infect Dis 9(11): 1-10.
-
Walawe Nayaka S (2023) Late Postpartum Pyrexia and Ascites Due to Peritoneal Tuberculosis. Journal of Women Health Care & Gynecology 2(2): 1-5.
-
Webster AS, Shandera WX (2014) The extrapulmonary dissemination of tuberculosis: A meta-analysis. Int J Mycobacteriol 3(1): 9-16.
-
Peto HM, Pratt RH, Harrington TA, LoBue PA, Armstrong LR, et al. (2009) Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006. Clin Infect Dis 49(9): 1350-1357.
-
Abad CLR, Razonable RR (2018) Mycobacterium tuberculosis after solid organ transplantation: A review of more than 2000 cases. Clin Transplant 32(6): e13259.
-
Uygur-Bayramicli O, Dabak G, Dabak R (2003) A clinicaldilemma: abdominal tuberculosis. World J Gastroenterol 9(5): 1098-1101.
-
Alexandre AT, Raimundo S, Pinto C (2017) Peritoneal tuberculosis - A rare diagnosis. Rev Port Pneumol 23(3): 172-173.
-
Peto HM, Pratt RH, Harrington TA, LoBue PA, Armstrong LR, et al. (2009) Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006. Clin Infect Dis 49(9): 1350-1357.
-
Mimidis K, Ritis K, Kartalis G (2005) Peritoneal tuberculosis. Ann Gas-troenterol 18(3): 325-329.
-
Sanai FM, Bzeizi KI (2005) Systematic review: tuberculous peritonitis--presenting features, diagnostic strategies and treatment. Aliment Pharmacol Ther 22(8): 685-700.
-
Kedar RP, Shah PP, Shivde RS, Malde HM (1994) Sonographic findings in gastrointestinal and peritoneal tuberculosis. Clin Radiol 49(1): 24-29.
-
Bhargava DK, Shriniwas, Chopra P, Nijhawan S, Dasarathy S, et al. (1992) Peritoneal tuberculosis: laparoscopic patterns and its diagnostic accuracy. Am J Gastroenterol 87(1): 109-112.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’