Clinical Repercussions of having Insight Regarding Human Uterine Innervation in Development of Innovative Treatment of Chronic Pelvic Pain Specifically in Incapacitating Pain Correlated with Endometriosis- A Short Communication
Having earlier reviewed pain correlated endometriosis here newer insight received in tackling these severe incapacitating pain which we encounter in routine practice for tackling patients impacted in view of their incapability of working. Recently Pinsard M, et al. conducted an experimental study. Where they dissected the pelvises of 4 human female foetuses into serial sections, followed by treatment with hematoxylin and eosin staining prior to immune staining. They detected nerves (S100 þ) and characterized the kinds of nerves. The slices derived had an alignment for the construction of a 3-dimensional (3D) model. On the constructed 3D model, the nerve fibers apparently possessed a centripetal path from the uterine serosa to the endometrium. Amongst the myometrium, enrichment of density of innervation was found. Endometrial innervation was scanty however was existent in the functional layer of the endometrium. In toto maximum abundance of innervation was existent in the supravaginal cervix and sparse in the body of the uterus. Innervation was laterally to the cervix adjacent to the parametrium and paracervix. Four kinds of nerve fibers were isolated: autonomic sympathetic (THþ), parasympathetic (VIPþ), and sensitive (NPYþ), (CGRP1þ) and (VIPþ). They were observed in the 3 parts and the 3 layers of the uterus. Thus concluding how a constructed 3D model of human uterine innervation model might yield a robust base for assessment of uterine innervation in pathologic situations, for finding newer therapeutic strategies. For gaining greater insight regarding the physiology of pain in pelvic pain pathological situations, like endometriosis, in which changes of uterine innervation have been emphasized, they conducted an anatomic & functional mapping of the macro & micro innervation of human uterus to provide a 3-D reconstruction model of uterine innervation. This would help us in planning innovative therapeutic strategies for incapacitating pain in endometriosis cases with repeated endometriosis surgeries& quality of life (QOL).
Introduction
Complicated benign pelvic diseases, for instance chronic pelvic pain, endometriosis, myomas as well as adenomyosis, are common in addition to possess the capacity of substantially impacting a woman’s quality of life [1]. Numerous studies point that they are correlated with uterine as well as pelvic innervation aberrations [2, 3, 4].
Tokushigue N, et al. [3] illustrated that patients with endometriosis possess an autonomic innervation of the superficial layer of the endometrium in contrast to control patients. Nevertheless, in a cohort of patients with myomas or adenomyosis, Zhang X, et al. [4] illustrated that just patients with pain were having innervation of the functional layer as well as significantly greater innervation of the myometrium. Moreover, Ellet L, et al. [5] illustrated that nerve fibers were existent in the endometrium of patients with in addition to without endometriosis in a cohort of patients with pain neuromas.
Additionally, Quinn MJ, et al. [2] described microneuromas within the myometrium in patients with chronic pelvic pain. These outcomes obtained point that uterine innervation is implicated in complicated benign pelvic diseases, in addition to specifically in nociceptive modes correlated with pelvic pain.
Nevertheless, scarcity of outcomes obtained have been revealed with regards to the distribution as well as particular nature of intrauterine innervation in the human and its association to uterine parts in addition to layers. Newer anatomic techniques, for instance immunohistochemistry, fluorochromes as well as computer-assisted anatomic dissection (CAAD) have been generated to study pelvic neuroanatomy recently with clinical along with surgical repercussions [6, 7].
Pelvic nerve supply distribution has been a topic with regards to evaluation for a long time duration. At the time of the part of the latter 19th century Jaboulay as well as Riggi independently provided further detailed neuroanatomic approaches with regards to surgical interference with pelvic autonomic nerves regarding relieving robust dysmenorrhea [8]. Despite the advancements made in scientific research we have not been able to gather knowledge in the context of pelvic nerve supply. We still lack insight with regards to pelvic nerve pathways in addition to their subsequent repercussions.
Pinsard M, et al. [9], for the first instance has given provision of a 3 three dimensional (3D) reconstruction model with regards to innervation of the uterus in case of a fetal model. This kind of studies might contribute to the understanding of the physiology of the pelvic pain correlated pathologies in addition to approaches with regards to advantageous treatment of these situations. Their objective was to study the functional anatomy of uterine microinnervation with a CAAD in addition to provision of an exhaustive 3-dimensional (3D) reconstruction to develop methodology regarding a clinical correlation for the practicing reproductive endocrinology & Infertility specialist (REI).
Taking into account the present surgical treatments with regards to chronic pain, for instance 2 surgical strategies which therapeutically target nerve bundles; specifically presacral neurectomy as well as laparoscopic uterosacral nerve ablation (LUNA).
At the time of 1924 Cotte MG detailed the appropriate anatomical placement with regards to presacral neurectomy for achieving greatest outcomes obtained with regards to treatment of the pelvic pain in the midline [8]. Subsequently, there have been numerous studies which have detailed the pelvic autonomic nerves getting disrupted; nevertheless, the basic philosophy of the presacral neurectomy continues to be akin to that detailed by Cotte [8]. At the time of the performance of a presacral neurectomy, the superior hypogastric nerve plexus gets skeletonized at the triangle of Cote in addition to the resection of a portion of nerve fibers as well as ganglions existent in this region is attempted [8]. In case of patients having centralized pelvic pain, it has been illustrated that this strategy is efficacious in reduction of pain, dysmenorrhea in addition to dyspareunia [8, 10]. Nevertheless, with utilization of LUNA, the nerve pathways having placement at the uterosacral ligaments get interfered with. In a randomized controlled trial (RCT), conducted from 2009, patients undergoing LUNA did not reveal any enhancement of reduction of pain, dysmenorrhea in addition to dyspareunia in contrast to laparoscopy without pelvic denervation [11]. Conversely, in case of a RCT performed by Chen FP, et al. [10], the long term effectiveness of presacral neurectomy for dysmenorrhea was significantly greater in contrast to that of LUNA. Pinsard M, et al. [9], research might be yielding insight in the context of the reasons for variation in success rates with regards to these 2 strategies for pelvic denervation. Functional mapping of uterine innervation illustrated that the nerve fibers possessed a centripetal path having of the enrichment of innervation adjacent to the parametrium in addition to paracervix [9]. Their outcomes obtained in 2D models were as follows.
Uterine Innervation in the Human Fetal Models–2D Findings
The entry point of the uterine nerve fibers is lateral to the uterine isthmus as well as cervix. Nerve fibers arise directly from the inferior hypogastric plexus. Organization of uterine innervation. Uterine innervation is centripetal and runs from the uterine serosa to the endometrium (Figure 1).
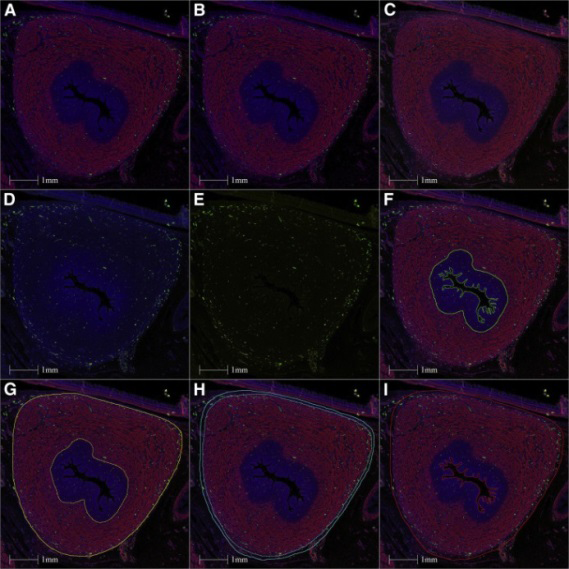
Figure 1: Courtesy ref no-9-Illustration of the use of immunofluorescence images to perform nerve quantification with the “HALO” software. Section of the uterine body treated with triple SMA-TH-NPY labeling, with DAPI. Each fluorochrome can be “switched off” or “switched on” depending on what we want to visualize. This illustration shows the centripetal disposition of the innervation of the uterus. (A) SMA + TH + NPY + DAPI. (B) SMA + TH + DAPI. (C) SMA + NPY + DAPI. (D) TH + NPY + DAPI. (E) TH + NPY. (F) Endometrial contouring. (G) Myometrium contouring. (H) Contouring of the serosa. (I) Contouring of the whole uterus. DAPI = 6-diamidino-2-phénylindole; NPY = neuropeptide Y; SMA = smooth muscle actin; TH = tyrosine hydroxylase.
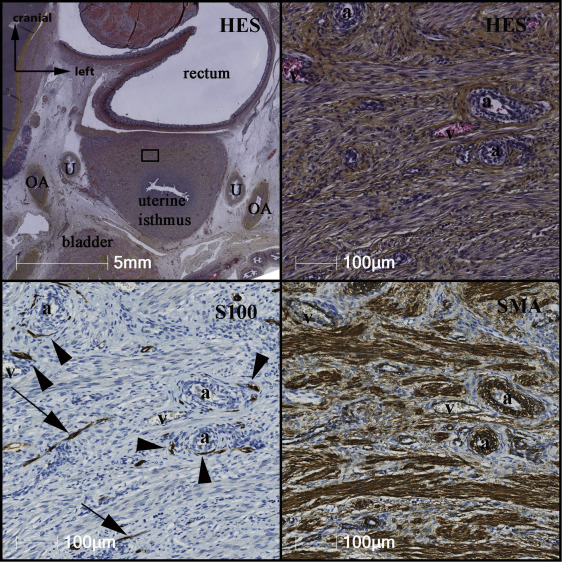
Figure 2: Courtesy ref no-9-Organization of nerve fibers within the myometrium on a cross-section at the uterine isthmus. Nerve fibers are preferably perivascular (black arrowheads), or they travel between muscle cells parallel to the axis of the muscular fibers (black arrows). a: arterioles. HES = hematoxylin eosin safran; OA = umbilical artery; SMA = smooth muscle actin; U = ureter; v = veins.
The uterine nerves infiltrate the myometrium in addition to their density diminishes on reaching the endometrium.
Myometrial innervation is dense (Figure 1) along with preferably perivascular, however further at certain instances perimuscular (Figure 2).
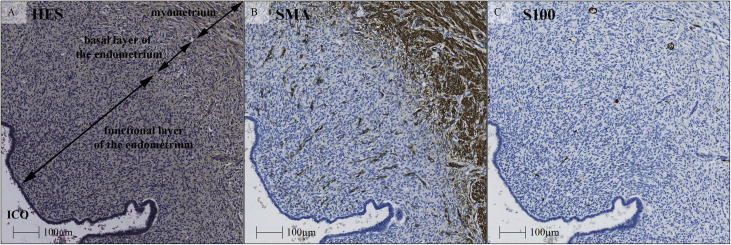
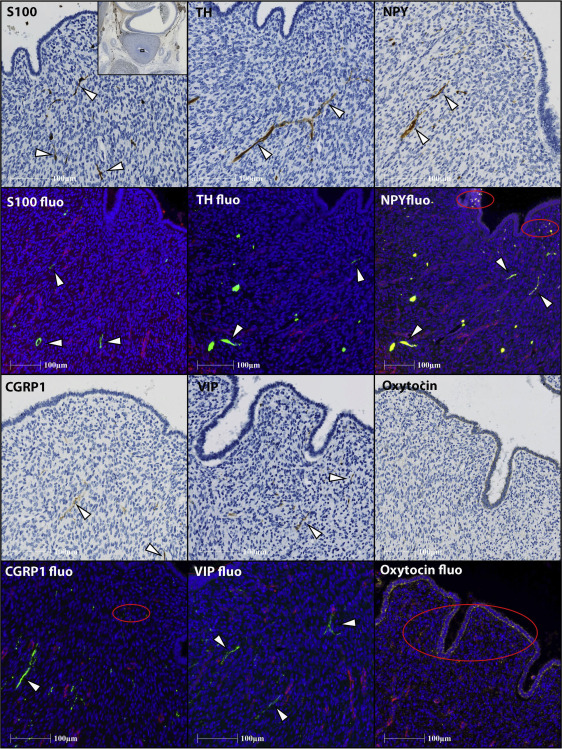
Uterine innervation generates a linear distribution amongst the myometrium. Despite the existence of endometrial innervation; however it is scanty. Pinsard M, et al. [9], found that amongst the nerves existent in all the layers of the endometrium they had a linear distribution amongst the functional layer of the endometrium (Figures 3 & 4).
Density of Nerves in the Uterus
Nerve density differed broadly amongst the varied parts of the uterus: having greater density at the cervix as well as lesser density in the uterine body (Figure 5). Nerves infiltrate penetrate the uterus at the uterine isthmus with maximum most of them further condensing around the cervix along with the others travelling up as well as down. Nerve density further differed among the variable uterine layers as detailed earlier as per the centripetal organization of uterine innervation. Its density is greater at the periphery amongst
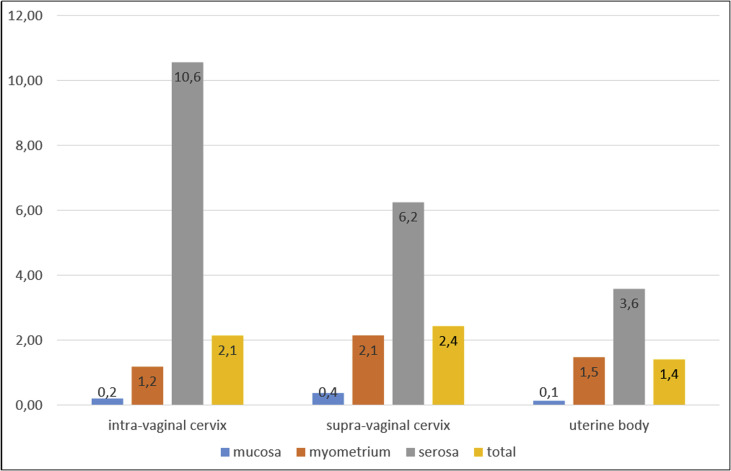
the serosa specifically laterally to the cervix adjacent to the parametrium as well as paracervix.
Uterine Innervation in the Human Fetal Models–3D Reconstruction of Fetal Uterine Innervation
Further they reconstructed a 3D uterine micro innervation model concentrating on the lower part of the uterus (Figure 6). Nerve fibers penetrate the uterus via the lateral edges of the uterine isthmus. Subsequently they then observed a centripetal path from the periphery (serosa) to the center (endometrium) with ascending fibers toward the cervix.
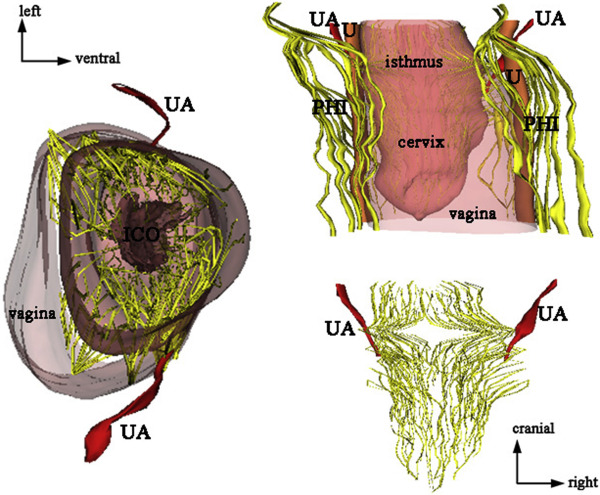
Figure 6: Courtesy ref no-9-Computer-assisted anatomic dissection of the uterine innervation shown in posterior and superior views. We focused our reconstruction on the lower part of the uterus, from the lower part of the uterine body to the tip of the cervix. It clearly illustrates the centripetal organization of the uterine nerve fibers, with fibers ascending to the uterine body, and descending to the cervix. ICO = internal cervical orifice; IHP/PHI = inferior hypogastric plexus; U = ureter; UA = uterine artery.
Thus it is sensible in attempting LUNA like methodology that disrupts the Frankenhauser plexus, would thus not be efficacious in contrast to the ones whose working is in the form of greater centralized nerve pathways for instance presacral neurectomy. On having greater insight with regards to placement as well as density of the nerves in the pelvis, greater adaptation of treatment is feasible with regards to these disorders.
Supracervical hysterectomy can be believed to be another instance of the manner this study possessed the capacity of explaining why such strategies not useful in endometriosis in view of this study has illustrated that the parametrium in addition to paracervix are the ones possessing maximum enrichment along with dense innervation, in contrast to that of the uterine body [9]. We have to acknowledge that of patients of endometriosis possess changed uterine as well as pelvic innervation [9].
From this we can attain greater insight with regards to leaving the cervix in case of patients of endometriosis in addition to pelvic pain who are undergoing hysterectomy might not be constituting the ideal procedure with regard to tackling pain. Actually, as per the personal experience of Nezhat CH&McGrail K patients of endometriosis who are undergoing supracervical hysterectomy do not apparently have that much significant relief of pain in contrast to those who are undergoing total hysterectomy (TAH) [12].
Noticeably, utilization of human fetuses was done by Pinsard M, et al. [9], in the form of the model in their studies which is believed to be a well acknowledged methodology with regards to asssessment of pelvic neuroanatomy. Nevertheless, the manner acknowledged by Pinsard M, et al. [9], themselves ,this does not aid in the probability of studying neurophysiological alterations caused by hormones [9]. Earlier work has corroborated the existence of ectopic endometrium in case of human female fetuses via autopsy evaluation [13]. Akin to the tissue evaluated by Pinsard M, et al. [9], via particular histochemical staining in addition to immunolabelling, the anatomic regions of the endometrial structures in the fetus have been illustrated tobe intricate to the posterior wall of uterus, posterior cul de sac as well as recto vaginal septum in addition to rectal tube as well as wall of uterus [13].
Conclusion
Considerable skill was illustrated by Pinsard M, et al. [9], in the utilization of advancements of software that by manipulation of two dimensional sections (2D) led to the production of a 3D model. A vista of probabilities have been introduced with this inclusive of probable mapping of endometriosis with staining for cancer antigen 125, cytokeratin 7 in addition to cluster of differentiation (CD) 10 along with estrogen in addition to progesterone receptor, an event which might be contributing in the corroboration of the hypothesis of embryonic cell remnants cited in the form of one of the etiologies of endometriosis [13].
Provision of a precious information to the paucity of the publications with regard to the neurological pathways of chronic pelvic pain has been attained by the authors. Furthermore, attractive is the advancements in the methodology yielded by this study specifically is the probability of the approaches for the adult neuroanatomy as posited by Pinsard M, et al. [9]. With regard to their future studies going in the depth of the insight attained over pelvic innervation, development of greater insight over present pathologies in addition to methodologies is attained.
Apparently this is the first study that has developed an exhaustive model in reference to uterine innervation in case of physiological situations with provision of a robust base regarding evaluating uterine innervation in case of pathological conditions. Restricted studies have detailed human uterine innervation so extensively. Pinsard M, et al. [9], have emphasized the strengths as well as restrictions of their study implicated in assessment, opening avenues with regard to the probability of conducting histological studies with the utilization of section dependent 3D models [12]. Having earlier reviewed pain correlated endometriosis with in capacitating pain here newer insight received in tackling these kind of severe incapacitating pain which we encounter in routine practice for tackling patients with repeated endometriosis surgeries& quality of life (QOL) impacted in view of their incapability of let alone attending professional work but were unable to even tolerate pain while resting with nothing working [14, 15, 16, 17].
Nevertheless, Pinsard M, et al. [9], research might be yielding insight in the context of the reasons for variation in success rates with regards to these 2 strategies for pelvic denervation. Functional mapping of uterine innervation illustrated that the nerve fibers possessed a centripetal path having of the enrichment of innervation adjacent to the parametrium in addition to paracervix, aiding in choice of strategy for relieving pain in such conditions once we have got insight of human uterine innervation innovative strategies to address them.
References
-
Pynnä K, Räsänen P, Sintonen H, Roine RP, Vuorela P, et al. (2021) The health-relatedquality of life of patients with a benign gynecological condition: a 2-year follow-up. J Comp Eff Res 10(8): 685-695.
-
Quinn MJ, Kirk N (2002) Differences in uterine innervation at hysterectomy. Am J Obstet Gynaecol 187(6): 1515-1520.
-
Tokushigue N, Morkham R, Russel P, Fraser IS (2007) Different types of small nerve fibres in eutopic endometrium and myometrium in women with endometriosis. Fertil Steril 88(4): 795-803.
-
Zhang X, Lu B, Huang X, Xu H, Zhou C, et al. (2010) Innervation of endometrium and myometrium in women with painful adenomyosis and uterine fibroids. Fertility and Sterility 94(2): 730-737.
-
Ellett L, Readman E, Newman M, McIlwaine K, Villegas R, et al. (2015) Are endometrial nerve fibres unique to endometriosis? A prospective case control study of endometrial biopsy as a diagnostic test for endometriosis in women with pelvic pain. Hum Reprod 30(12): 2808- 2815.
-
Timoh KN, Bessede T, Lebacle C, Zaitouna M, Martinovic J, et al. (2017) Levator ani muscle innervation: anatomical study in human fetus. Neurourol Urodyn 36(6): 1464- 1471.
-
Timoh KN, Moszkowicz D, Zaitouna M, Lebacle C, Martinovic J, et al. (2018) Detailed muscular structure and neural control anatomy of the levator ani muscle: a study based on female human fetuses. Am J Obstet Gynecol 218(1): 121.e1-121.e12.
-
Katz A, Nezhat CH (2013) Laparoscopic treatment of chronic pelvic pain. In: Nezhat C, et al. (Eds.), Nezhat’s video assisted and robotic assisted laparoscopy and hysteroscopy.4th(Edn.), Cambridge, Cambridge University Press, pp: 435-448.
-
Pinsard M, Mouchet N, Dion L, BessedeT, Bertrand M, et al. (2022) Anatomic and functional mapping of human uterine innervation. Fertil Steril 117(6): 1279-1288.
-
Chen FP, Chang SD, Chu KK, Soong YK (1996) Comparison of laparoscopic presacral neurectomy and laparoscopic uterosacral nerve ablation for primary dysmenorrhea. J Reprod Med 41(7): 463-466.
-
Daniels J, Gray R, Hills RK, Latthe P, Buckley L, et al. (2009) laparoscopic uterosacral nerve ablation for alleviating chronic pelvic pain: a randomized controlled trial. J Am Med Assoc 302(9): 955-961.
-
Nezhat CH, McGrail K (2022) Exploring fetal pelvic neuroanatomy:a deep dive into understanding nerve pathways, endometriosis and pain. Fertil Steril 117(6): 1289-1290.
-
Signorile PG, Baldi A (2020) The presence of endometriosis in the human fetus. In: Nezhat CH, et al. (Eds.), Endometriosis inadolescents: a comprehensive guide to diagnosis and management. Cham, Springer International Publishing, pp: 205-214.
-
Kaur KK, Allahbadia GN, Singh M (2017) Meeting the Challenges of Endometriosis Associated Pain-Newer Options for Future and Research Directions. Meeting the Challenges of Endometriosis Associated Pain-Newer Options for Future and Research Directions. BAOJ Bioinfo 2(1): 9.
-
Kaur KK, Allahbadia GN, Singh M (2016) An Update on Pathophysiology and Medical Management ofEndometriosis. Advances in Reproductive Sciences 4(2): 53-73.
-
Kaur KK, Allahbadia GN, Singh M (2020) Dilemna regarding preference of surgery or medical treatment in case of tubal blockade, endometriosis or adenomyosis and pelvic adhesion prevention once surgery is contemplated –a systematic review’’. Gynaecology, Andrology and Reproductive Medicine.
-
Kaur KK, Allahbadia GN, Singh M (2020) Management of Inoperable Recurrent Endometrioma Presenting as Severe Incapacitating Pain Following Leuprolide Acetate Depot by Aspiration, Recurring Again a 2 Yrs Subsequently for Sclerosing Therapy at Present: A Case Report. SunText Rev Case Rep Image 1(1): 107.
- Postpartum Maternal Mental Health - A Narrative Review
- Beta HCG in Cervico-Vaginal Secretion as a Predictor of Preterm Delivery
- Successful Management of Mid Trimester Foetal Death with Major Placenta Previa by Expectant Management Followed by Induction of Labour
- To Evaluate the Expression of Egr2 Gene in Term Low Birth Weight Newborns
- Impact of Maternal Obesity on Maternal and Foetal Outcomes: A Prospective Cohort Study from Northern India
- ‘’Benefit of Pulsatile GnRH Therapy in Treatment of Functional Hypothalamic Amenorrhea (FHA) and Congenital Hypogonadotropic Hypogonadism(CHH) in Infertile Patients Over Canonical Gonadotropins with IVF –A Short Communication’’