How to Perform Perfect Nd: YAG Capsulotomy
Know the Indication Posterior capsular opacity (PCO) causing decreased vision and significant glare Know the Contraindications a) Corneal scars, irregularity, or edema: It precludes adequate visualization of the target aiming beam. b) The patient with poor fixation: There may be inadvertent damage to adjacent intraocular structures. c) Active intraocular inflammation
Know the Indication
Posterior capsular opacity (PCO) causing decreased vision and significant glare
Know the Contraindications
a) Corneal scars, irregularity, or edema: It precludes adequate visualization of the target aiming beam. b) The patient with poor fixation: There may be inadvertent damage to adjacent intraocular structures. c) Active intraocular inflammation
Technique
Dilation of the eye is optional. Be careful, capsulotomy in dilated eye may be eccentric when pupil changes to normal size later. a) Explain the patient procedure is painless and expect to hear the pop or click sound. b) Put a drop of Apraclonidine or beta-adrenergic blocking agent just before the procedure. c) Topical anesthesia is rarely needed. It is mandatory if the contact lens is to be used. Do not forget to put a coupling agent, 2%, or 2.5% hydroxypropyl methylcellulose while using contact lens. d) Adjustment of stool, table, chin rest, and footrest for optimal patient comfort, head strap to maintain forehead position. e) Preferably perform the procedure in a dark room. f) Ask the patient to see the fixation target, usually illuminated with the fellow eye, and keep the eye open. g) Make sure the laser beam is not in anterior focus. Fix the laser setting in posterior or neutral focus. h) Start with minimum energy 1-3 mJ. The laser settings actually depend on the density of the fibrous growth. i) Aim for 3-4 mm central capsulotomy to prevent glare in night and target excellent optics. j) Avoid extending the capsulotomy past the edge of the Opinion optic to avoid anterior migration of the vitreous.
Two Techniques
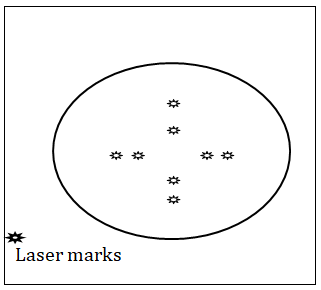
Cruciate Pattern: Begin at 12 o’clock in the periphery and progress toward 6 o’clock. Unless a wide opening has already developed, shots are then placed at the edge of the capsule opening, progressing laterally toward the 3 and 9 o’clock positions. Because the capsule flaps are still attached, this method tends to avoid the creation of free-floating capsular fragments in the vitreous. If needed, additional laser spots can be placed along the mid-position of these flaps to further expand the size of the central opening [1] (Figure 1).
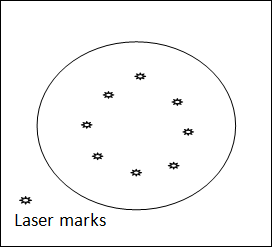
Circular Pattern: This involves using the YAG laser to create a circular pattern which then allows for around posterior capsular opening. The circular capsular cut-out can end up free-floating in the vitreous and can create a disturbing, large floater in the patient’s vision. If the circular opening is left intact at the bottom then the capsular flap will still be attached and will be less likely to cause a floater [2] (Figure 2).
Tips to Avoid Intraocular Lens (IOL) Pitting
a) Use minimum energy. b) Use contact lens, especially in dense posterior opacity. It also stabilizes the eye, improves laser beam optics, and facilitates accurate focusing. c) Try to avoid hitting the central area. d) Begin treatment at the areas of intraocular lens–capsule separation and cut across tension lines, characterized by its wrinkling nature. e) Use deep focus techniques: Focus the laser posterior to the capsule, which causes optical breakdown in the anterior vitreous. The shock wave radiates forward and ruptures the capsule. The breakdown threshold is higher in the anterior vitreous than at an optical interface so higher energy, usually a minimum of 2mJ, is required. f) Polymethylmethacrylate and Silicon IOL tend to have more pitting compared to Acrylic IOL.
Follow-up
Patients are usually put on topical steroids for inflammation at the discretion of the surgeon. Prescribe topical steroids for a week and ask for follow-up in a week for manifest refraction and assess the intraocular pressure and inflammation [3].
References
-
Saunders WB (1985) The Nd: YAG laser in ophthalmology: principles and clinical applications of photodisruption, Philadelphia.
-
(2020) Nd: YAG laser capsulotomy, Clinical education, Laser surgery education center, American Academy of ophthalmology.
-
Deepak R (2020) Nd: YAG laser capsulotomy, emedicine. medscape.com.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report