Irregular Astigmatism Correction by Femtosecond Laser Arcuate Keratotomy in a Pediatric Patient
We report the case of a pediatric patient 3 years old that underwent refractive surgery for the correction of irregular astigmatism after penetrating trauma. A single arcuate keratotomy by femtosecond laser was performed for correcting corneal high order aberrations in the attempt to avoid penetrating keratoplasty and to treat amblyopia.
Introduction
In children [1] penetrating traumatic injury of ocular anterior segment represents the more frequent cause of non- congenital blindness. Corneal or scleral laceration, traumatic cataract, intraocular foreign body, vitreous hemorrhage, and prolapse of intraocular tissue are most frequent associated clinical conditions. Secondary corneal opacity often affects these patients, inducing significant visual loss and amblyopia in children. Actually acquired traumatic corneal scars after penetrating injuries represent a frequent indication for pediatric keratoplasty, for whom however it is note that corneal perforations determinates a poorest prognosis [2].
In this paper we report the case of a refractive surgery performed to correct irregular astigmatism induced by penetrating corneal trauma. The aim of the treatment was to avoid corneal keratoplasty and to limit visual deprivation amblyopia.
On 16th of February 2010 at 3 years old male child presented to Bambino Gesu Children’s Hospital of Rome, Italy, with diagnosis of penetrating trauma in right eye. Informed consent to all the procedures was collected and all experimental investigations followed the guidelines for experimental investigation with human subjects required by the institution. The study adhered to the Tenets of the Declaration of Helsinki.
During the emergency operation performed under general anaesthesia, the lens was removed because of anterior capsule opening and corneal irregular wound across the pupil was sutured by single 10.0 nylon stitches. Two months after, on the 16th of April 2010, an intraocular lens (IOL) was implanted into the sulcus. However, nevertheless contact lens wearing and left eye 6 hours daily patching, six months after IOL implantation Distance Corrected Visual Acuity (DCVA) was 0.2, Near Corrected Visual Acuity (NCVA)
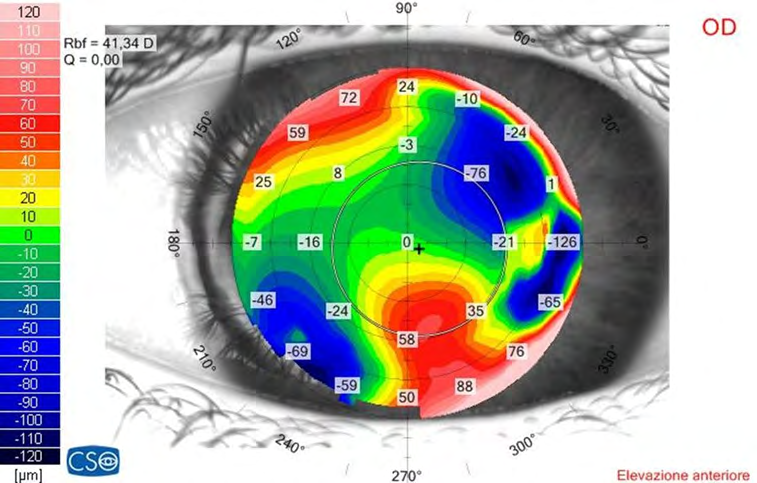
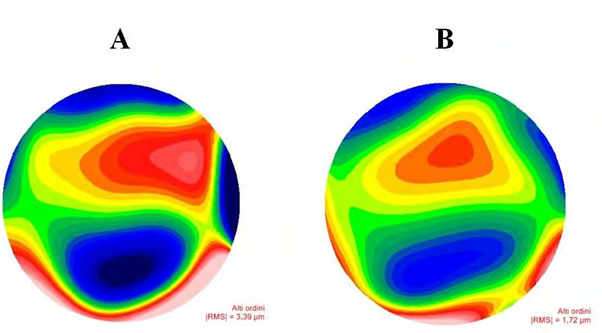
was Jaeger 5, refractive error was +7.0 sphere and -11.0 cylinder axis 85°, topographic astigmatism and corneal High Order Aberrations (HOAs) for 5.0mm pupil were respectively 12.0 diopters (axis 113°) and 3.99 µm. Left eye uncorrected visual acuity was 1.0. In right eye the elevation map showed a steeper inferior asymmetry into the optical zone produced by corneal scar, in the area corresponding to the inferior bow tie (Figure 1). The orthoptic evaluation showed eye suppression to worth lights test in right eye, corneal reflex well cantered, moderate exotropia at cover test and normal ocular motility. On the 12nd of October 2010 a single arcuate keratotomy (AK; 80° arc length, 80% corneal depth and 6.0mm optical zone) centred on the steepest meridian according to the elevation map was performed by the Intra Lase 60KHz femtosecond laser (Abbot Medical Optics). Because of the small eye diameter the docking procedure was performed without suction ring according to the technique previously described [3]. No intraoperative o postoperative complications occurred. The laser treatment reduced refractive astigmatism to 6.50 diopters and HOAs for 5.0mm pupil from 3.39µm to 1.72µm (Figure 2).
After femtosecond laser surgery the patient wore contact lens on right eye and continuously performed left eye 6 hours daily patching until he was 9 years old. DCVA, NCVA, corneal topography and aberrometry measured by Sirius Scheimpflug camera (CSO, Italy) were evaluated during 8 year follow up.
Eight years after trauma, right eye refractive error was +1.0 sphere -6.50 cylinder axis 80°, DCVA was 0.6 and NCVA 1 Jaeger; the right eye suppression was observed both for distance and near vision, cover test revealed orthotropia to esotropia for near vision, and orthotropia for distance vision; ocular motility appeared normal again. HOAs for 5.0mm pupil as well as the refractive astigmatism amount resulted unchanged over time. Left eye uncorrected visual acuity remained unchanged too.
Discussion
In children ocular traumatic penetrating injuries are common cause of significant visual impairment and amblyopia [4]. Corneal wound across the pupil represents a poor prognostic factor because scarring and residual irregular astigmatism are correlated with unfavourable visual outcome [4].
Pediatric refractive surgery is actually performed in much selected patients. It is generally considered if neurodevelopmental disability determinates poor compliance with high refractive error correction, as well as in case of anisometropic amblyopia, when refractive correction and occlusive therapy do not induce visual acuity improvement [5]. In these last patients, moreover, the timing of treatment results crucial. In fact it is note that amblyopia could be reversed until the age of 8 to 9 years [5].
Some authors observed that AK performed with femtosecond laser was effective and predictable in reducing post keratoplasty high astigmatism [6, 7], decreasing complications including corneal perforation [7]. However few papers reported the application of femtosecond technology to pediatric corneal surgery [3, 8]. To our knowledge this is the first case reported on femtosecond laser AK in pediatric patients.
In this case report we propose the use of femtosecond laser for performing AK in order to correct irregular astigmatism induced by residual scar in central cornea after penetrating trauma (Figure 3). Since we observed a correspondence between topographic asymmetric bow tie and elevation map inferior steepening, we planned a single AK in the attempt to regulate corneal shape and to decrease corneal high order aberration amount. Nevertheless the young age of this patient, we considered topographic data reliable because of good correspondence of topographic astigmatism data with cycloplegic refraction data. It has been reported an association between the magnitude of induced anisometropia and interocular HOAs difference [9]. A greatest amount of corneal HOAs in amblyopic eyes suggest that non-rotationally symmetric aberrations may be induced by abnormal ocular development as reported in monocular deprivation paradigms of other animal species. Since asymmetric visual experience during development in amblyopic eye appears to be associated with asymmetries in HOAs [9], our findings confirm the possible role of HOAs in developing amblyopia and suggest that the high precision of femtosecond laser cutting could be considered also in the attempt to regulate irregular corneal shape.

We evaluated the opportunity to implant toric IOL, but in children a sulcus implanted IOL could be easily decentralised by fibrosis and, in any case, it cannot provide corrections of corneal HOAs that are responsible of amblyopia. Another possible surgical approach could be represented by penetrating keratoplasty, commonly indicated in children in case of acquired traumatic opacities [2, 10], but several authors reported a low prognosis rate for graft survival at 1 year [10], mainly in children less than 5 years old [11].
In conclusion, in selected pediatric patients affected by irregular astigmatism, femtosecond laser AK could improve amblyopia treatment and avoid more complex surgery as well as penetrating keratoplasty.
References
-
Segev F, Assia EI, Harizman N, Barequet I, Almer Z, et al. (2007) Corneal laceration by sharp objects in children seven years of age or younger. Cornea 26(3): 319-323.
-
Vanathi M, Panda A, Vengayil S, Chaudhuri Z, Dada T (2009) Pediatric keratoplasty. Surv Ophthalmol 54(2): 245-271.
-
Buzzonetti L, Petrocelli G, Valente P (2012) Big- bubble deep anterior lamellar keratoplasty assisted by femtosecond laser in children. Cornea 31(9): 1083-1086.
-
Hsing LC, Lan L, Yuh KL, Kuo LK, Ling YM (2009) Prognostic indicators of open globe injuries in children. Am J of Emerg Med 27(5): 530-535.
-
Stahl ED (2015) Pediatric refractive surgery: a 2015 perspective. Mo Med 112(3): 218-222.
-
Buzzonetti L, Petrocelli G, Laborante A, Mazzilli E, Gaspari M, et al. (2009) Arcuate keratotomy for high postoperative keratoplasty astigmatism performer with intralase femtosecond laser. J Refract Surg 25(8): 709- 714.
-
Han SB, Liu YC, Noriega KM, Mehta JS (2020) Application of femtosecond laser in anterior segment surgery. J Ophthalmol.
-
Buzzonetti L, Petrocelli G, Laborante A (2010) Anterior lamellar keratoplasty assisted by intralase femtosecond laser in a pediatric patient. J Pediatr Ophthalmol Strabismus 21: 47.
-
Vincent SJ, Collins MJ, Read SA, Carney LG (2012) Monocular amblyopia and higher order aberrations. Vis Res 66: 39-38.
-
Huang C, O‘Hara M, Mannis MJ (2009) Primary pediatric keratoplasty: indications and outcomes. Cornea 28(9): 1003-1008.
-
Buzzonetti L, Ardia R, Petroni S, Petrocelli G, Valente P, et al. (2016) Four years of corneal keratoplasty in Italian paediatric patients: indications and clinical outcomes. Graefes Arch Clin Exp Ophthalmol 254(11): 2239-2245.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report