ICL Explant Due to Ocular Hypertension, Reduced Endothelial Cell Count and Anterior Sub Capsular Cataract Due to Patient Selection Error
Implantable Collamer Lenses (ICL) are phakic lenses that are implanted in the posterior chamber of the eye for the correction of myopia, hyperopia, and astigmatism in those patients who cannot undergo corneal refractive surgery, the main feature of the latest models. Of ICL is a hole in the optical center of the lens, which facilitates the natural flow of aqueous humor. Among the contraindications for ICL implantation are: Corneal pathologies, cataracts, glaucoma, retinal pathologies such as degenerations or detachments, diabetic retinopathy, patients allergic to collagen, pseudo-exfoliative syndrome, pigment dispersion syndrome, pupillary abnormalities, endothelial count less than 2000 mm2, uveitis, under 20 years of age or with unstable refraction. We present the case of a 24-year-old female patient who came to the clinic for refractive surgery due to high myopia, an ICL -18.00 D implant was proposed in the left eye. In the preoperative examinations: the UBM presented an iris plateau with multiple angle-closing cysts. In the optic nerve OCT she presents a moderate and severe decrease in nerve fibers and the visual field with PHG: outside normal limits, MD: -12.84 dB. After the postoperative period, the patient presented with ocular hypertension that was controlled with antihypertensive, he achieved IOP control a month after the operation, but after a few months postoperatively he presented a low endothelial cell count and an anterior sub capsular cataract, for which it was decided to explant the ICL. Finally, cataract surgery was performed and a monofocal IOL was implanted.
Introduction
Implantable Collamer Lenses (ICL) are phakic lenses that are implanted in the posterior chamber of the eye, they are made of collamer, a polymer of porcine collagen and hydroxyethyl methacrylate, it is used for the correction of myopia, hyperopia and astigmatism in those patients with moderate refractive errors and corneas who cannot undergo corneal refractive surgery [1]. The ICLs are designed to be implanted in the posterior chamber, between the iris and the anterior lens capsule, the haptics resting on the ciliary sulcus. These lenses are indicated for patients 21 to 45 years of age for the correction of myopia in patients with spherical equivalent (SE) ranging from -3.0 D to -20.0 D and for the correction of myopic astigmatism in patients with SE ranging from -3.0 D to -20.0 D with a cylinder from 1.0 D to 4.0 D1. A minimum true anterior chamber depth (ACD), measured from the corneal endothelium to the anterior surface of the lens of 2.80 to 3.00 mm, and an age-appropriate minimum endothelial cell density (ECD) are required for patients are suitable for the implantation of this type of lens [1, 2]. The ICL implant is not exempt from complications that must be treated in a timely manner; the risks are angle-closure glaucoma, progressive loss of endothelial cells, endophthalmitis and vitreoretinal complications [3]. The Vault is the distance between the posterior surface of the lens and the anterior surface of the lens, which must be measured periodically. A vault between 250 and 750 μm is considered safe. A low vault is related to the formation of anterior sub capsular cataracts and an excessive vault is associated with ocular hypertension and the development of glaucoma [4]. The FDA reported that approximately 6-7% of patients implanted with older ICL models developed anterior sub capsular cataracts beginning 7-10 years after surgery, but only 1-2% progressed to clinically significant cataracts [5]. The FDA reported endothelial cell loss related to ICL implantation to be 8.9% at 3 years and 7.7% at 5 years after surgery in patients with normal ACD [6]. One of the possible causes of early endothelial loss is corneal trauma during surgery, while phakic lenses made of silicone have been reported to cause greater endothelial loss those progresses over time [7].
Case Report
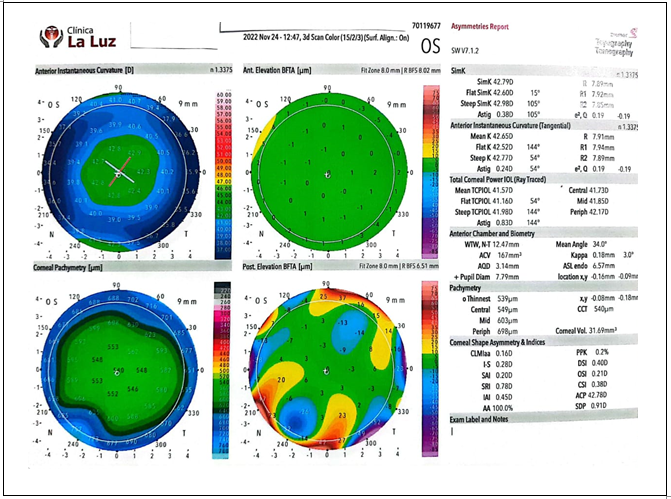
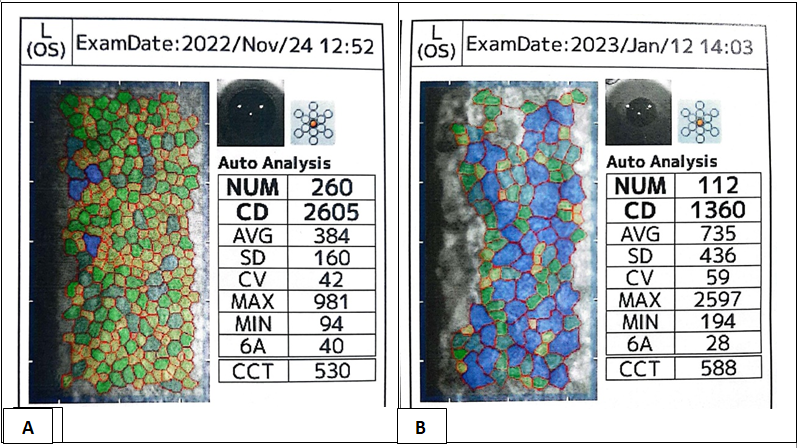
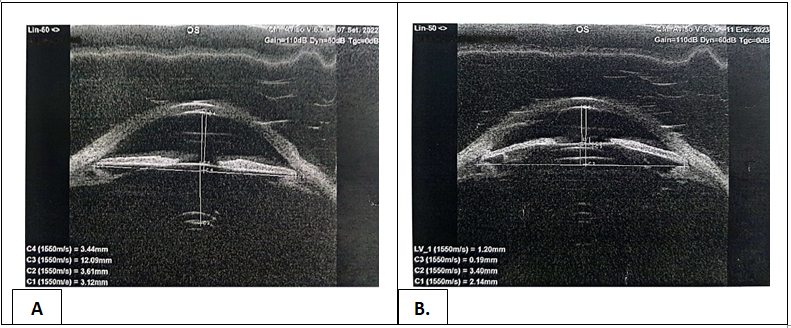
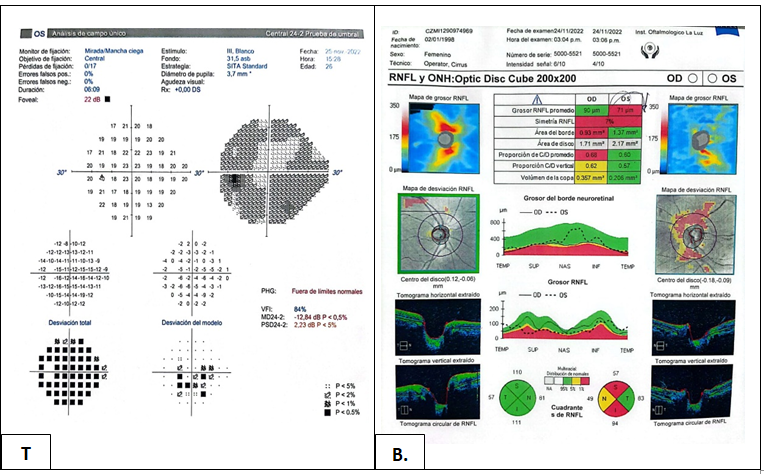
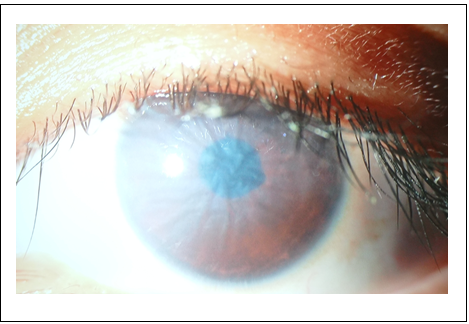
A 24-year-old female patient attends the Clinica La Luz for the first time in the ophthalmology area. The case complies with the Declaration of Helsinki. The ethics committee and the institutional review board of Clinica La Luz approved the case report, obtaining the written informed consent of the patient. Patient refers that she wants to stop wearing glasses. At the evaluation, she presented an uncorrected visual acuity (AVSC): Left Eye (LE) finger count (CD) 30 cm, corrected to LogMAR 2.1 and a visual acuity with correction (AVCC): 20/80 that corrected to LogMAR 0.6. His subjective refraction was OI: -19.00 -1.00 x 100°. On physical examination: clear cornea, formed camera, reactive pupil, clear lens in both eyes. IOP: 18/16, Fundus: cup: 0.6, oblique optic nerve, thinned retina, applied. High myopia is diagnosed, moderate amblyopia in the left eye (Figure 1). Femtolasik surgery is indicated in RE and ICL implantation in LE explaining to the mother and patient who eye is amblyopic, even so they agreed to proceed with surgery. Preoperative examinations: Specular microscopy: LE: CD: 2605, CV: 42, 6A: 40 (Figure 2A & 2B) UBM: Horizontal disposition of the iris and multiple cysts that close the angle in the temporal quadrant compatible with plateau iris in both eyes (Figure 3A & 3B). Computerized visual field LE 24/2: PHG: outside normal limits, MD: -12.84 dB (Figure 4A); OCT (optical coherence tomography) LE: RNFL: 71, severe decrease in RNFL in the upper and lower quadrants and moderate decrease in the nasal quadrant. (Figure 4B) Galilei corneal topography showed an AQD (measured distance from the corneal endothelium) of 3.14 mm.
She underwent refractive surgery with an ICL EVO Staar surgical -18.00 D implant in the LE. During the ICL implant, the lens came out in the wrong position, so maneuvers had to be performed to rotate the lens and place it in the proper position without complications. Postoperative day 1 with AVSC LE: 20/400 corrected to LogMAR 1.3, presenting with ocular pain and blurred vision. Bio microscopy revealed 3+ microcystic corneal edema, with Descemet folds, narrow chamber, intumescent iris, VH 1, non-reactive pupil, ICL could be seen in position. IOP: LE: 48 mmHg. Management was decided with IV mannitol (intravenous) 300 cc, Dorzolamide, timolol and brimonidine 1 drop every 12h for 1 month, Prednisolone 1% 1 drop every 6h in a reduction scheme for 1 month, Acetazolamide 250mg 1 tab vo every 8h for 3 days with Orange juice, citing it in 1 week. (Figure 5).
A week after the postoperative evaluation, IOP 23 mmHg, for which reason glaucoma consultation is requested for management. LE gonioscopy was performed: Shaffer 1 in the lower, nasal and temporal region, Shaffer 2 in the upper region. Dorzolamide, timolol and brimonidine are continued 1 drop every 12 hours. A control UBM was requested, which reported: narrow anterior chamber, VAULT 190 um, presence of plateau iris with multiple ciliary body cysts that contribute to angle closure. Six weeks after ICL implantation, biomicroscopy in the LE revealed a clear cornea, narrow chamber, VH1, reactive pupil, and LOCS III classification, sub capsular 2+. IOP: LE: 16 mmHg. A new specular microscopy examination was performed, which revealed a decrease in the endothelial cell count from 2,605 to 1,360 endothelial cells, with a variability coefficient of 42 to 59, for which ICL explant plus phacoemulsification with Acrysof IOL +2.00 D IOL was decided. At one month of follow-up RE that underwent femtolasik AVSC: 20/20 converted to logMAR 0.0 and in the LE: 20/50 that converted to LogMAR 0.4.
Discussion
Kato, et al. reported that the ideal vault is 250 to 750 μm. Poor vault (<250 μm) increases the risk of anterior sub capsular cataract whereas excessive vault (>750 μm) is associated with chamber angle closure, pupillary block, pigmentary glaucoma, and corneal edema [4]. In the case presented in the postoperative UBM, it was evidenced that the vault was 190 μm, which is outside the safety margin; this would be the cause of why the posterior sub capsular cataract was formed. Fernandez, et al. reported that elevated intraocular pressure and secondary glaucoma account for 4.4% of postoperative complications after ICL implantation [8]. Gharaibeh, et al. [9] reported on a 27-year-old patient who developed iris and ciliary cysts after ICL implantation. They suggested that the iris and ciliary cysts originated from corneal or conjunctival epithelial cells that were implanted into the iris during surgery or migrated into the iris through the surgical wound postoperatively [9]. In the preoperative UBM, a horizontal disposition of the iris and anteriorization of the ciliary body were evidenced, in addition to multiple cysts that closed the angle, for which reason it was thought that this was the cause of the increase in IOP and angle closure.
Kocova, et al. [10] reported that cataract is one of the common complications after ICL implantation, and early cataract after ICL implantation is mainly related to surgical trauma, while late cataract is mainly related to contact between ICL and the crystalline. The most common type of ICL-associated cataract is anterior sub capsular cataract (SCA) [10]. The patient developed an anterior sub capsular cataract 6 weeks after ICL implantation. Niu, et al. reported that according to the FDA the ECD loss related to central whole ICL implantation is 8.9% at 3 years and 7.7% at 5 years after surgery in patients with normal ACD [6]. One of the possible causes of early endothelial loss is corneal trauma during surgery, while phakic lenses made of silicone have been reported to cause greater endothelial loss those progresses over time [7]. During the surgical act, the ICL was implanted in an incorrect position, so maneuvers had to be carried out and the ICL rotated in the anterior chamber. According to studies, it is reported that ocular trauma in the surgical act is the factor that would be related early loss of endothelial cells.
Conclusion
This case report concludes the importance of an adequate evaluation and selection of the patient with a preoperative UBM to rule out pathologies that could alter the ICL implant after the postoperative period, as happened in our case.
Acknowledgments
The authors thank the patient for her acceptance with the informed consent, to carry out the realization of this case.
Disclosure
The authors report no conflicts of interest in this work.
Conflicts of Interest
No
References
-
Wannapanich T, Kasetsuwan N, Reinprayoon U (2023) Intraocular Implantable Collamer Lens with a Central Hole Implantation: Safety, Efficacy, and Patient Outcomes. Clin Ophthalmol 17: 969-980.
-
Kamiya K, Shimizu K, Igarashi A, Kitazawa Y, Kojima T, et al. (2018) Posterior Chamber Phakic Intraocular Lens Implantation in Eyes with an Anterior Chamber Depth of Less Than 3 mm: A Multicenter Study. Sci Rep 8(1): 13322.
-
Chuck RS, Jacobs DS, Lee JK, Afshari NA, Vitale S, et al. (2018) Refractive Errors & Refractive Surgery Preferred Practice Pattern®. Ophthalmology 125(1): P1-P104.
-
Kato S, Shimizu K, Igarashi A (2020) Assessment of low- vault cases with an implantable collamer lens. PLOS ONE 15(11): e0241814.
-
Steinwender G, Tigka KV, Shajari M, Kohnen T (2017) Anterior sub capsular cataract caused by forceful irrigation during implantation of a posterior chamber phakic intraocular lens with a central hole. J Cataract Refract Surg 43(7): 969-974.
-
Niu L, Miao H, Han T, Ding L, Wang X, et al. (2019) Visual outcomes of Visian ICL implantation for high myopia in patients with shallow anterior chamber depth. BMC Ophthalmol 19(1):121.
-
Shaaban YM, Badran TAF (2020) Three-Year Effect of Phakic Intraocular Lenses on the Corneal Endothelial Cell Density. Clin Ophthalmol 14: 149-155.
-
Fernandes P, Meijome JMG, Costa DM, Blasco TF, Jorge J, et al. (2011) Implantable Collamer Posterior Chamber Intraocular Lenses: A Review of Potential Complications. J Refract Surgery 27(10): 765-776.
-
Gharaibeh A, Liehneova I, Mojzis P, Ziak P, Alio JL (2020) Iris and ciliary body cysts and phakic intraocular lenses. Eur J Ophthalmol 30(5): 974-977.
-
Kocova H, Vlkova E, Michalcova L, Motyka O (2017) Implantation of posterior chamber phakic intraocular lens for myopia and hyperopia - long-term clinical outcomes. J Fr Ophthalmol 40(3): 215-223.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report