Bilateral Sclerochoroidal Calcifications: A Case Report
Purpose: The aim of this case report is to describe a rare condition of bilateral sclerochoroidal calcification Case Report: A 79 years old asymptomatic Caucasian female was referred to our Ocular Oncology Center of the Ophthalmic Surgery Department of Pisa on November 2021. She was in apparent good health. Funduscopic examination revealed yellowwhite irregular lesions in the supero-temporal quadrant of both eyes. Best-corrected visual acuity was 20/20. B-scan and A-scan ultrasound revealed hyper-echoic solid lesions with acoustic orbital shadowing measuring 1.5 mm in thickness and 4.6 mm in diameter, on average. Enhanced Deep Imaging Optical Coherence Tomography showed a scleral lesion compatible with the presence of deposition of calcium with Table Mountain and rolling pattern. Fluorescein angiography revealed hypofluorescence in the arterial phase and a mild hyper-fluorescence in the venous phase with persistent late staining. Indocyanine green angiography showed hypo-fluorescence at the early, middle, and late phases. Systemic investigation of calcium and phosphate metabolism was performed and the patient didn’t display any underlying systemic disorder. Conclusion: It is important to know and recognize this condition. Although most cases of sclerochoroidal calcifications may be idiopathic, systemic laboratory workup must be performed to exclude calcium-phosphate metabolic disorder that can be associated to these ocular signs. Given the rare possible development of choroidal neovascularization, regular imaging checkup is recommended.
Introduction
Sclerochoroidal calcifications is a rare, benign condition characterized by yellow-white flat or minimally elevated lesions typically located in the supero-temporal post- equatorial area or along the temporal arcades [1]. It is often discovered in older white asymptomatic individuals during a routine fundus examination. There is a slight female predisposition (approximately 60% of cases) [2]. The lesions are commonly symmetric and bilateral [3]. This condition can be idiopathic or associated to systemic calcium disorder [4]. Clinically, it can be mistaken for choroidal osteoma, choroidal metastasis, amelanotic choroidal nevus, choroidal lymphoma or choroiditis [5]. Fluorescein angiography, optical coherence tomography and ultrasonography may help in confirming the diagnosis. Clinical prognosis can vary depending on systemic associations. Visual prognosis is generally good even if in rare cases choroidal neovascularization (CNV) may occur [6, 7].
Case Report
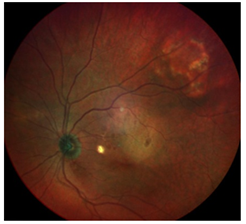
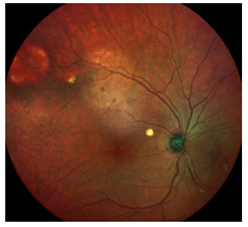
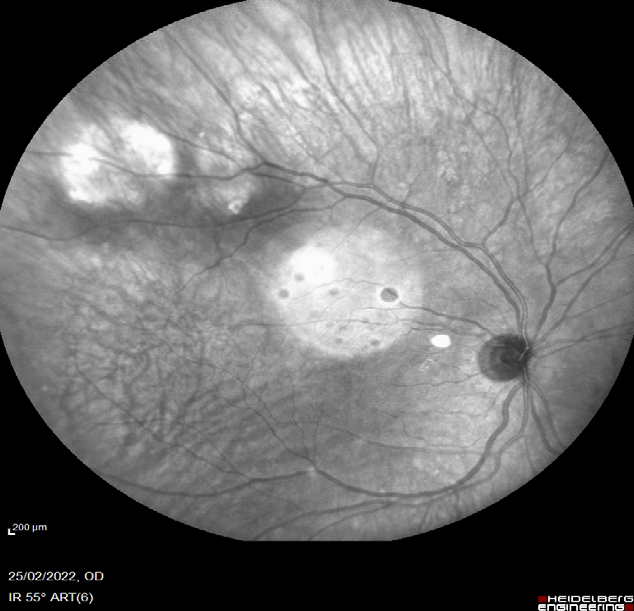
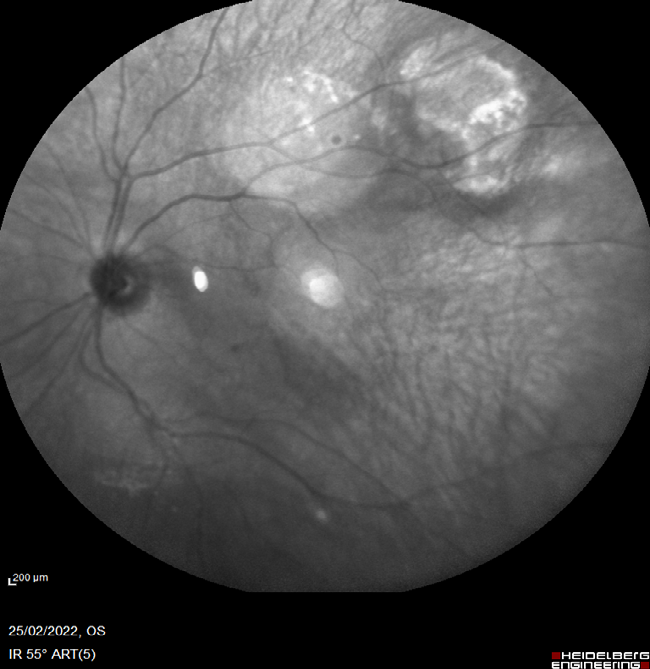
A 79 years old asymptomatic Caucasian female was referred to our Ocular Oncology Center of the Ophthalmic Surgery Department Pisa on November 2021. She was in apparent good health. Funduscopic examination revealed yellow-white irregular lesions in the supero-temporal quadrant of both eye (Figures 1 & 2).
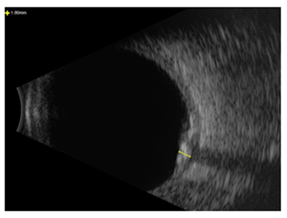
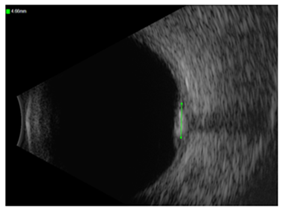
Best-corrected visual acuity was 20/20. B-scan and A-scan Standardized Echography was performed with a 20 and a 10 MHz probe and revealed hyperechoic solid lesions with acoustic orbital shadowing measuring 1.5 mm in thickness and 4.6 mm in diameter, on average (Figures 3 & 4).
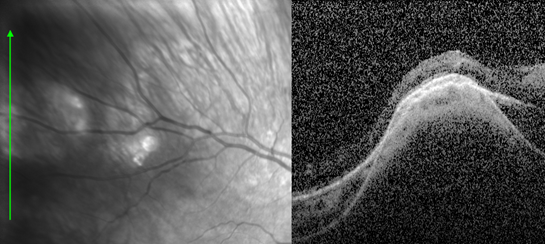
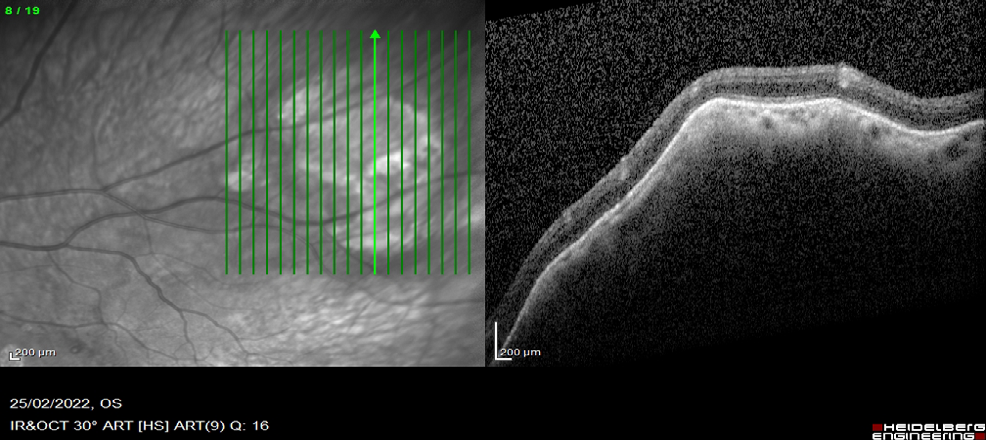
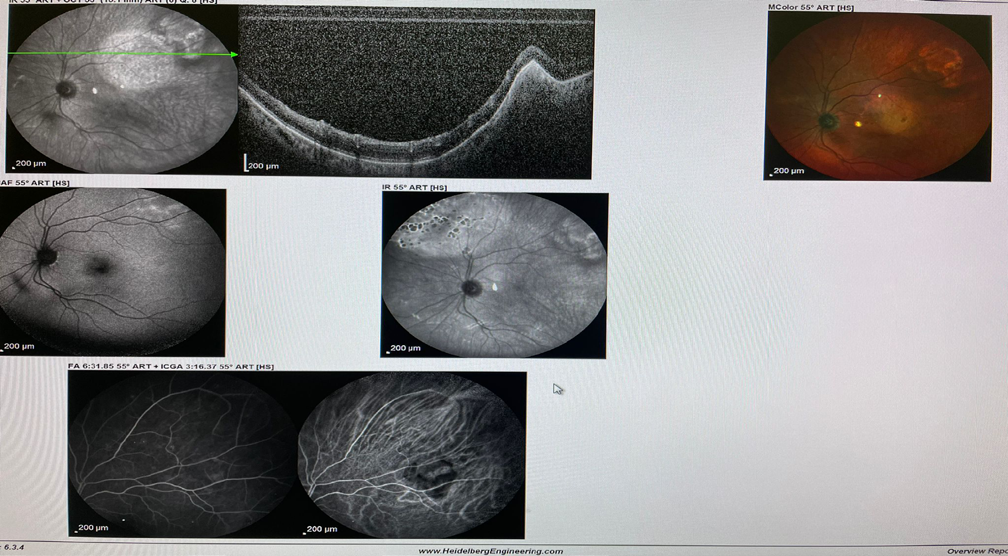
Enhanced Deep Imaging Optical Coherence Tomography (EDI-OCT) showed scleral lesion compatible with the presence of deposition of calcium with table mountain and rolling pattern (Figures 5& 6).
Fundus auto fluorescence showed hyper auto- fluorescence in the areas of the lesions annular pattern on the right eye and bright speckles on the left eye (Figures 7 & 8).

Fluorescein angiography revealed hypo fluorescence in the arterial phase, and a mild hyperfluorescence in the venous phase with persistent late staining. Indocyanine green angiography showed hypofluorescence at the early, middle, and late phases (Figures 9 & 10).
Systemic investigation of calcium and phosphate metabolism was performed and the patient didn’t display any underlying systemic disorder. The diagnosis of idiopathic sclerochoroidal calcification was made. At twelve month follow-up examination the lesions were stable with no lesion enlargement or decalcification or choroidal neovascularization.
Discussion
Sclerochoroidal calcification is an uncommon benign condition that may have an idiopathic, dystrophic or metastatic pathogenesis [3, 8]. This condition is primary in 79% of cases and secondary in 21% [9]. Indeed dystrophic calcification can occur after chronic intraocular inflammation and ocular trauma [10]. In metastatic calcification the deposition of calcium in normal tissues is secondary to abnormal calcium-phosphorus metabolism displayed in chronic renal disease, hyperparathyroidism, hypervitaminosis D, hypophosphatemia and sarcoidosis [11, 12, 13]. Bartter’s syndrome and Gitelman’s syndrome are two rare conditions that can be associated with sclerochoroidal calcifications. Both are autosomic recessive renal tubular disorders of sodium-chloride transport. Bartter Syndrome generally occurs in childhood, with polyuria, polydipsia, vomiting and dehydration. These patients present hypokalemic metabolic alkalosis, increased potassium excretion, and normal-to-elevated levels of urine calcium excretion. The Gitelman syndrome is characterized by a later clinical presentation with fatigue, muscle weakness, and episodes of tetany. Hypocalciuria and hypomagnesaemia are the prominent features [14]. It is important to determine the presence of these diseases because electrolyte abnormalities and potential cardiac arrhythmias can be fatal without appropriate management [15]. Calcium deposition was shown to be confined to the sclera [16]. Hasanreisoglu, et al. has classified sclerochoroidal calcification into four categories based on enhanced depth imaging optical coherence tomography. According to anterior surface topography of the mass, they described four patterns: flat, rolling, rocky-rolling and Table Mountain [17]. Based on this classification in our case the lesions showed a rolling pattern with a thinning of the overlying choroid at the apex on the left eye and a table mountain with a preserved overlying choroid on the right eye. Choroidal neovascularization in rare cases may complicate the course of sclerochoroidal calcification as reported by Battaglia Parodi, et al. that recently described two cases treated by intravitreal injection [18]. In literature are described about 70 cases. It is possible that the pathogenesis is related to the retinal pigment epithelium compression and this can lead to the development of choroidal ischemia in the area of the lesions with subsequent development of choroidal neovascularization [19]. In our case no neovascularization was displayed.
Conclusion
It is important to know and recognize this clinical entity. Although most cases of sclerochoroidal calcifications may be idiopathic as in the patient described in this case report, systemic laboratory workup must be performed to exclude calcium-phosphate metabolic disorder or primary renal tubular hypokalemic metabolic alkalosis syndromes (e.g. Gitelman syndrome, Bartter syndrome) that can be associated to these ocular signs. Moreover, given the rare possible development of CNV, a regular imaging check-up is recommended.
Funding
None.
Conflicts of Interest
The authors declare no conflict of interest, financial or otherwise.
References
-
Cooke CA, McAvoy C, Best R (2003) Idiopathic sclerochoroidal calcification. Br J Ophthalmol 87(2): 245-246.
-
Thomson AC, Brown GT, Rodriguez AD, Hunter AA (2021) A case of extensive bilateral idiopathic sclerochoroidal calcification and review of the literature. Int Med Case Rep J 14: 749-755.
-
Shields JA, Shields CL (2002) CME review: sclerochoroidal calcification: the 2001 Harold Gifford Lecture. Retina 22(3): 251-261.
-
Shields CL, Hasanreisoglu M, Saktanasate J, Shields PW, Seibel I, et al. (2015) Sclerochoroidal calcification: clinical features, outcomes, and relationship with hypercalcemia and parathyroid adenoma in 179 eyes. Retina 35(3): 547-554.
-
Sivalingam A, Shields CL, Shields JA, McNamara JA, Jampol LM, et al. (1991) Idiopathic sclerochoroidal calcification. Ophthalmology 98(5): 720-724.
-
Bessette AP, Singh AD (2016) Multimodal imaging of choroidal neovascularization associated with sclerochoroidal calcification. Ocul Oncol Pathol 2(4): 234-238.
-
Jessen MG, Ali MH, Grewal DS (2019) Rare Complication of Sclerochoroidal Calcifications. JAMA Ophthalmol 137(1): 111-112.
-
Honavar SG, Shields CL, Demirci H, Shields JA (2001) Sclerochoroidal calcification: clinical manifestations and systemic associations. Arch Ophthalmol 119(6): 833- 840.
-
Shields CL, Hasanreisoglu M, Saktanasate J, Shields PW, Seibel I, et al. (2015) Sclerochoroidal calcification: clinical features, outcomes, and relationship with hypercalcemia and parathyroid adenoma in 179 eyes. Retina 35(3): 547-554.
-
Shields JA, Shields CL (1992) Osseous tumors of the uvea. In: Intraocular Tumors: A Text and Atlas, Philadelphia, Pa WB Saunders Co, pp: 265- 266.
-
Gartner S, Rubner K (1955) Calcified scleral nodules and hypervitaminosis D. Am J Ophthalmol 39(5): 658- 663.
-
Wong S, Zakov ZN, Albert DM (1979) Scleral and choroidal calcifications in a patient with pseudohypoparathyroidism. Br J Ophthalmol 63(3): 177-180.
-
Goldstein BG, Miller J (1982) Metastatic calcification of the choroid in a patient with primary hyperparathyroidism. Retina 2(2): 76-79.
-
Soriano JR (1998) Bartter and related syndromes: the puzzle is almost solved. Pediatr Nephrol 12(4): 315-327.
-
Fulchiero R, Mayer PS (2019) Bartter Syndrome and Gitelman Syndrome. Pediatr Clin North Am 66(1): 121-
-
Fung AT, Arias JD, Shields CL, Shields JA (2013) Sclerochoroidal calcification is primarily a scleral condition based on enhanced depth imaging optical coherence tomography. JAMA Ophthalmol 131(7): 960- 963
-
Hasanreisoglu M, Saktanasate J, Shields PW, Shields CL (2015) Classification of Sclerochoroidal Calcification Based on Enhanced Depth Imaging Optical Coherence Tomography “Mountain-Like” Features. Retina 35(7): 1407-1414.
-
Parodi MB, Arrigo A, Pina A, Calcafgno F, Antropoli A, et al. (2021) Choroidal neovascularization complicating sclerochoroidal calcifications Am J Ophthalmol Case Rep 24: 101235.
-
Mitamura M, Kase S, Ishida S (2020) Multimodal imaging in sclerochoroidal calcification: a case report and literature review. BMC Ophthalmol 20(1): 248.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report