Challenging Ophthalmic Complications of Diabetic Hypertension
To report challenging ophthalmic complications in a diabetic-hypertensive patient. Diabetes is a progressive disease that adversely affects on multiple organ systems, with hypertension being a common comorbidity. The eyes, sometimes, are indicators of the systemic diseases like diabetes and hypertension. Both conditions adversely affect the macrovascular and microvascular systems. Systemic complications of these diseases are sometimes complicated and complex. In this case report, caroticocavernous fistula (CCF), pupil involving third cranial nerve palsy and clinically significant macular edema (CSME) coexisted in a single patient, presenting diagnostic and therapeutic challenges.
Abbreviations
CCF: Caroticocavernous Fistula; CSME: Clinically Significant Macular Edema; IVB: Intravitreal Bevacizumab; BCVA: Best Corrected Visual Acuity; CTA: CT Angiogran; BP: Blood Pressure; DR: Diabetic Retinopathy.
Introduction
Diabetes mellitus is an important problem that induces ernestful complications and it causes significant morbidity owing to specific microvascular complications such as retinopathy, nephropathy and neuropathy, and macrovascular complications such as ischemic heart disease, and peripheral vasculopathy [1].
Apart from poor glycaemic control, blood pressure (BP) has been shown to be an important risk factor for Diabetic Retinopathy (DR). Evidence from clinical trials has demonstrated beneficial effect of tight BP control on risk of DR in patients with diabetes and hypertension [2].
Not only is hypertension more common in patients with diabetes but also diabetes is also more common in hypertensives than in the general population. Therefore, there is a chicken-egg relationship between hypertension and diabetes. To this point, hypertension occurs in 50% to 80% of patients with type 2 diabetes, who make up over 90% of the diabetic population versus ≈30% of patients with type 1 diabetes who develop hypertension [3].
In adults, the most common causes of ocular motor palsy are aneurysm, microvascular disease (such as diabetes mellitus), and trauma. In patients with DM, ocular motor nerve palsy is a common cause of acquired diplopia and/ or ptosis. In diabetics, the calculated incidence of cranial nerves palsies is 5-10 times higher than in non-diabetics. Approximately 1-4% of diabetics have ocular motor nerves palsies during the course of the disease. In diabetic patients, ocular motor nerve palsies showed a propensity for the third and the sixth nerves, with relative sparing of the fourth. Type 2 DM patients with diabetic retinopathy were most frequently affected [4].
Caroticocavernous fistula (CCF) is an abnormal communication between the cavernous sinus and the carotid system. CCFs can be classified by etiology (traumatic vs spontaneous) and anatomy (direct vs indirect or dural). The dural CCF may be due to congenital arteriovenous malformation that develops spontaneously, often in the setting of atherosclerosis, systemic hypertension, or connective tissue disease. It consists of a communication between cavernous sinus and one or more meningeal branches of the internal carotid artery, external carotid artery, or both. The posteriorly draining dural CCF most commonly presents with cranial nerve palsies. The onset of the paresis is sudden, and only one of the ocular motor nerves is affected. The third nerve is most often affected, and the resulting paresis may be complete with involvement of the pupil or incomplete with or without pupil involvement. But almost all cases are associated with ipsilateral orbital pain [5].
Case Presentation
A 56 years old diabetic hypertensive lady presented with reduced vision right eye for two weeks. She denied any history of head or eye injury. The best corrected visual acuity (BCVA) was 6/9 in the right eye and 6/6 in the left eye.
Examination of the posterior segment of right eye revealed retinal hemorrhage, hard exudates and macular edema. The patient was diagnosed with Clinically Significant Macular Edema (Figure 1). She received intravitreal bevacizumab (IVB) (1.25mg/0.05 mL) administered at six- week intervals for three doses.

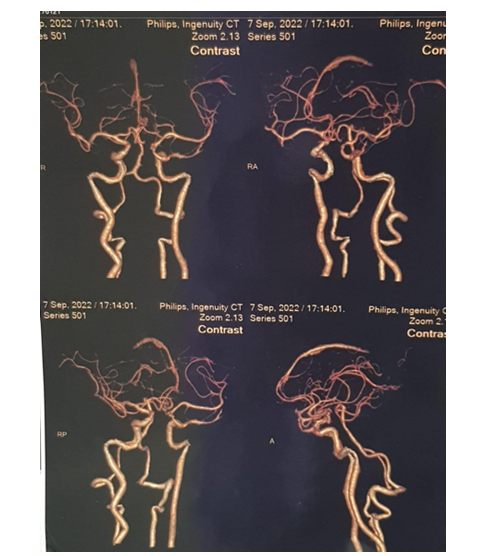
Four weeks after the third IVB dose, the patient developed pupil involving 3rd cranial nerve palsy on the right side. The right eye was deviated downward and outward, with a dilated pupil that did not react to direct light stimulus. Other cranial nerve functions were normal. A CT Angiogran (CTA) was performed to look for intracranial aneurysms, but no positive findings were detected (Figure 2). Patient was under observation and 3rd cranial nerve palsy recovered without any intervention.
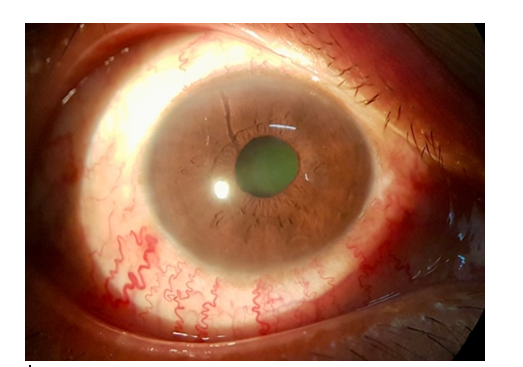
Six months later, she presented with proptosis and red eye in the same right eye. Cockscrew conjunctival vessels and axial proptosis were detected, leading to a clinical diagnosis of spontaneous caroticocavernous fistula (Figure 3).
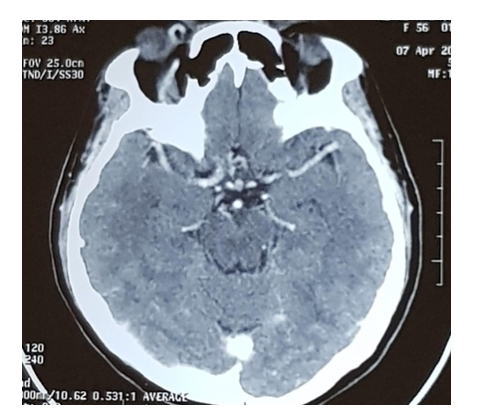
To confirm the diagnosis, CT (head and orbit) was performed and enlarged superior ophthalmic vein on right side was detected (Figure 4).
Discussion
This case presented initially with visual impairment from CSME in right eye. Subsequently, pupil involving third cranial nerve palsy occurred in her right eye. The most common cause of isolated third nerve palsy with pupillary involvement is an aneurysm in the posterior communicating artery [6]. Therefore, CTA was performed to find out the aneurysm, but none was detected. The patient was under observation and third cranial nerve palsy spontaneously recovered completely. She later presented with red eye, conjunctival cockscrew vessels and axial proptosis in the same eye. CCF was suspected and distended superior ophthalmic vein was detected on CT.
Causes of dural fistula includes hypertension and post- menopausal women are most commonly affected [7]. Our patient is post-menopausal hypertensive and diabetic woman with poor control of both diseases. All the vascular complications of diabetes and hypertension were developed sequentially in our patient, with the presentation being unusual as CCF features developed after spontaneous complete recovery of the third cranial nerve palsy.
Conclusion
Diabetes mellitus and hypertension are prevalent non communicable diseases. Strict control of both diseases is difficult for patients as they are chronic incurable diseases. Lack of patient awareness and barriers to accessing quality healthcare impede effective management in Myanmar. Ophthalmic complications would be preventable with proper control of diabetes and hypertension.
References
-
Sayin N, Kara N, Pekel G (2015) Ocular complications of diabetes mellitus. World J of Diabetes 6(1): 92-108.
-
Gurkirat SK, Bhupendra CP (2023) Carotid Cavernous Fistula. Stat Pearls Publishing, Treasure Island, Finland.
-
Jia G, Sowers JR (2021) Hypertension in Diabetes: An Update of Basic Mechanisms and Clinical Disease. Hypertension 78(5): 1197-1205.
-
Chebel S, Bouatay AB, Ammar M, Yahia SB, Khairallah M, et al. (2009) Diabetes mellitus-associated ocular motor nerve palsies. Neurosciences 14(4): 386-388.
-
Venkatesan PE, Gnanashanmugam G, Parimalam N, Pranesh MB (2015) Diabetes plus third nerve palsy not always diabetic third nerve palsy. J Postgrad Med 61(1): 50-52.
-
Kim YJ, Lee SY, Jung JH, Seo JH, Kim EG, et al. (2013) Case of Isolated Third Nerve Palsy with Pupillary Involvement Diagnosed with Cavernous Dural Arteriovenous Fistula. J Neurocrit Care 6: 126-128.
-
Henderson AD, Miller NR (2018) Carotid-cavernous fistula: current concepts in aetiology, investigation, and management. Eye (Lond) 32(2): 164-172.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report