Limbal Relaxing Incisions in the Correction of Postoperative Astigmatism, in Eyes after Implantation of Various Types of Multifocal Spherical Lenses. Own Results
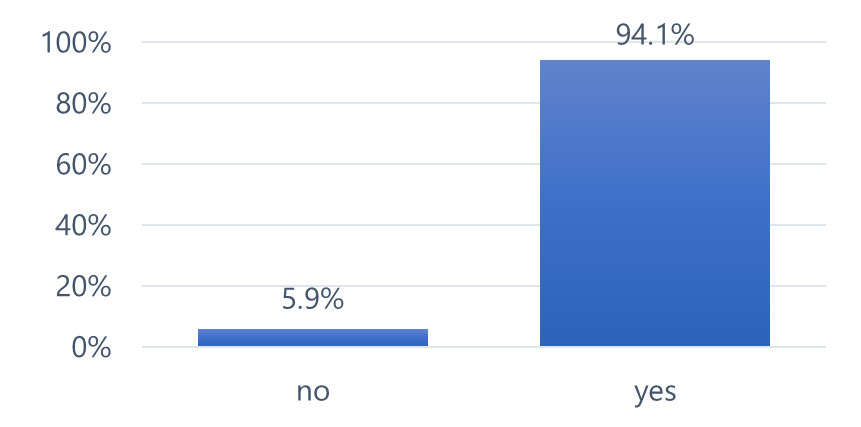
34 patients (34 eyes) who had previously undergone implantation of a multifocal spherical lens were treated for corneal astigmatism. In each case a Limbal Relaxing Incision was performed. Examinations using corneal topography showed the presence of astigmatism with an average value of 1.36 at the range of 0,63 to 2,61 dioptries. Only one patient had a corneal astigmatism value higher than 1.38 diopters. Patients, who complained of unacceptable, postoperative quality of vision and who did not achieve full distance visual acuity were qualified for the procedure. A reduction in the size of the astigmatism resulted in a subjective improvement in the quality of vision in practically 94% of cases and an improvement in distance visual acuity, by an average of 6.32 letters, measured on the logMAR chart. In the aforementioned case with corneal astigmatism of 2.61 diopters, the correction improved the vision to far distances by 20 letters.
Abbreviations
LRI: Limbal Relaxing Incisions; OCT: Optical Coherent Tomography; RLE: Refractive Lens Exchange; UBVA: Uncorrected Visual Acuity.
Introduction
Limbal Relaxing Incisions (LRI) are a well-established method for correcting small amounts of corneal astigmatism and have been in use for over 30 years [1]. However, the technique has its limitations, such as the maximum amount of astigmatism that can be corrected, which is no more than 3.0 diopters (Dcyl) [2]. The LRI procedure, which involves using a diamond knife, is not highly precise, mainly due to the technique used. The expected postoperative results are a combination of four factors: the size of astigmatism, the depth of the corneal incision, the extent of the incision, and the patient’s age. The depth of the peripheral corneal incision should be 90% of its peripheral thickness [2]. The thickness of the cornea is usually measured using Optical Coherent Tomography (OCT), a module for assessing the anterior segment of the eye. The location of the astigmatism to be corrected is determined by the steepest axis of the astigmatism. Since the choice of the measurement location depends on the person performing it, there is a risk that the measured corneal thickness may be subject to change.
The extent of the incision depends on the type of astigmatism. Astigmatism against the rule requires a larger incision range. The correction of astigmatism using an intraocular toric lens has also established rules. According
to some authors, a toric lens should be used when corneal astigmatism exceeds 0.5Dcyl [3]. Hayashi, analyzing a group of patients after implantation of multifocal diffractive lenses, emphasizes the need for astigmatism correction if its value exceeds 1.0 Dcyl [4].
Here, a question and a dilemma arise. When considering the above astigmatism values, do we take into account those generated by both the anterior and posterior surfaces of the cornea, or only by the anterior surface? Seyed-Farzad et al. indicate that the mean values of posterior astigmatism generated by the cornea range from -0.26 to -0.78 diopters [5].
Analyzing one of many of our own cases qualified for Refractive Lens Exchange (RLE) in which the anterior surface of the cornea generated astigmatism of 1,0Dcyl, the refractometry of the entire optical system showed astigmatism of 0,5Dcyl and the OCT of the posterior surface of the cornea showed a value of 0,5Dcyl, a dilemma arose: in the process of correcting the defect, would it make sense to use an intraocular spherical lens or a toric one?
Purpose
Evaluation of the effectiveness of corneal astigmatism correction performed in eyes in which a complex in structure, spherical intraocular lens was implanted. The astigmatism correction was carried out using the LRI technique.
Qualification for the LRI procedure included patients (eyes) for the following reasons:
- Dissatisfaction with the postoperative visual effect, including the quality of vision and distance visual acuity
- The presence of astigmatism generated by the anterior surface of the cornea ≥ 0,75Dcyl
- In one case, the procedure was performed in the eye where spherical multifocal lens was implanted in another center, despite the presence of corneal astigmatism at the level of 2.61D cyl.
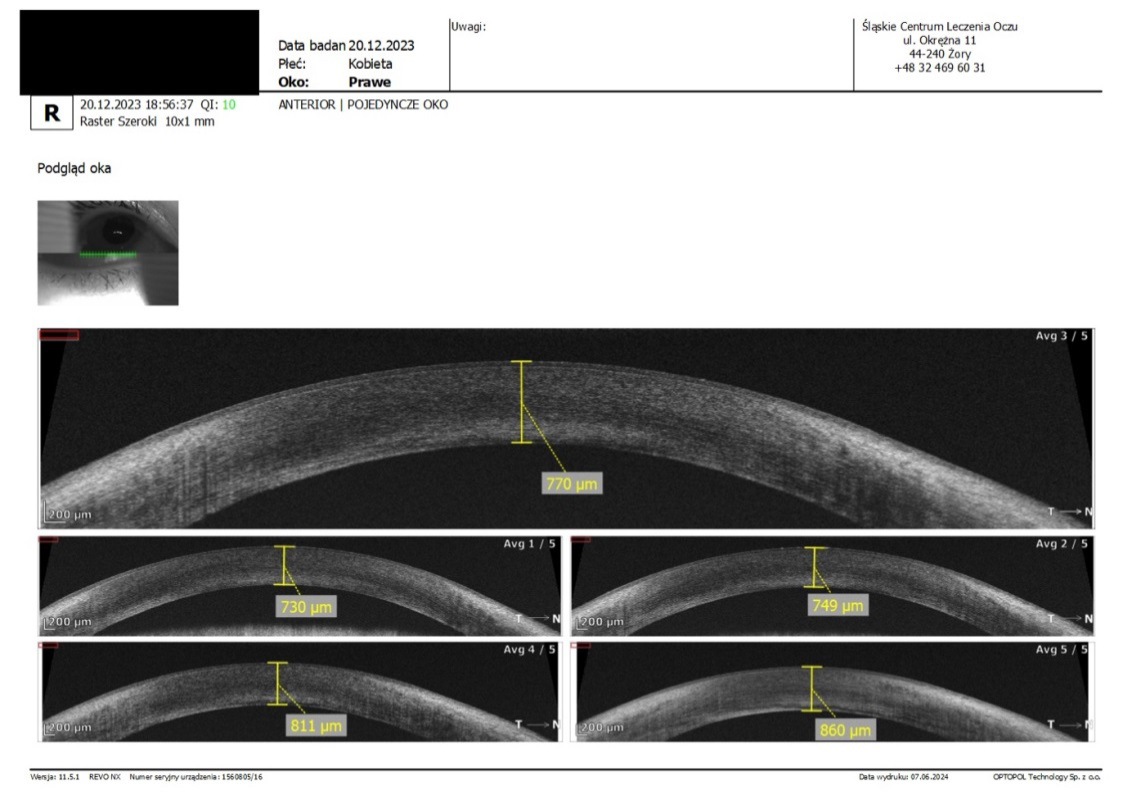
In each case, the selection of the intraocular lens for implantation involved an assessment of the size of the astigmatism using corneal topography and refractometry of the entire optical system, like also keratometry. In cases of doubt astigmatism size, another examination was performed to evaluate the value of the astigmatism on the posterior surface of the cornea. Usually it was the SD-OCT device module for assessing the parameters of the anterior segment of the eye, by Optopol Technology, REVO model. This device was also used to measure the thickness of peripheral cornea in location of the steep astigmatism (Figure 1).
If the anterior corneal astigmatism exceeded the value of 0,75Dcyl and the value of the astigmatism of the entire optical system (showed in refractometry) was the same, the eye was qualified for the implantation of a toric intraocular lens.
A corneal astigmatism value above 0,75Dcyl in eyes qualified for cataract removal always required the selection of a toric lens. In the case where the corneal astigmatism was within the range of 1.0-1.25Dcyl, but the value of the total astigmatism generated by the optical system of the eye assessed in the refractometry test did not exceed 0.75Dcyl, and the patient had never required astigmatism correction, an examination was performed to evaluate the value of the astigmatism on the posterior surface of the cornea. If the difference between the value of the anterior and posterior corneal astigmatism was not higher than 0.75Dcyl in eyes qualified for the RLE procedure, a spherical lens was implanted.
The diamond-tipped knife used during the procedure, thanks to the possibility of adjusting the size of the blade, allowed for a precise change in the depth of the cut.
During the process of removing the patient’s own lens, the main incision, with an average size of 2.2mm, was made in the steep axis of astigmatism in eyes where astigmatism was consistent with the rule. The axis of astigmatism was determined in the patient’s seated position, marking values of 0°-180° and then using the Tocular® lens with a scale, mounted in the Muller-Wedel microscope. In the case of astigmatism against the rule, the main incision was made on the border of the upper quadrants.
The types of spherical intraocular lenses implanted included 3-focal lenses with a concentric diffractive structure, a 3-focal lens with an asymmetrical structure, lenses with a “pure” EDOF (extended depth of focus) structure, and lenses with a combined structure of a 3-focal concentric lens with an EDOF structure. The choice of lens for implantation was determined by the structure of the eye, specifically the type of refractive error, pupil diameter, angles alpha and kappa. The procedure of LRI was performed in accordance with the NAPA (Nichamin Age- and Pachymetry-Adjusted) nomogram.
The study was conducted in accordance with the Declaration of Helsinki. The Bioethics Committee of the Medical Chamber of Silesia in Katowice, to which the assumptions of the article were presented, did not find it necessary to issue an opinion, due to the fact that the LRI procedure is a recognized method of correcting astigmatism, as is the implantation of multifocal lenses in eyes with diagnosed cataracts or unacceptable refractive errors (vision disorders). All surgeries and qualifying examinations were performed at the private medical center Slaskie Centrum Leczenia Oczu in Zory, Poland.
Results
Statistical Tests used. A significance level of p = 0.05 was adopted. The significance level is the maximum acceptable probability of error, which involves rejecting a true null hypothesis H0, which assumes that the groups being studied do not differ in terms of the characteristic of interest. This is therefore the degree of requirement at which a decision is made to reject or retain the hypothesis. According to the above, results of p < 0.05 will indicate the presence of significant dependencies between the variables. In order to examine the presence of a relationship between the variables, the Spearman’s rank correlation coefficient was used. The following hypotheses are assumed here:
- H0: there is no significant relationship between the variables
- H1 (alternative): there is a significant relationship between the variables.
The selection of tests was based on the distribution of the variables, which was verified using the Shapiro-Wilk test. In order to check for any significant difference between the measurements in the areas covered by the study, the non- parametric Friedman’s ANOVA test was used, where the following hypotheses are assumed:
- H0: the means are the same in the measurements
- H1 (alternative): the means are significantly different in the measurements.
The calculations were performed in the R statistical environment ver.3.6.0, the PSPP program, and MS Office 2019. In the statistical analysis of the obtained study results, the values of the best corrected visual acuity at a distance and near (BCVA) and the best visual acuity without correction (UBVA), as well as the values of corneal astigmatism in the corneal topography examination, which were performed before each surgical procedure, i.e. lens replacement and LRI procedure, were taken into account. In the postoperative analysis of the above results, the values obtained 4 weeks after the LRI procedure were included. Additionally, an analysis was performed of the correlation between the preoperative pupil diameter value and the postoperative UBVA value, obtained after the LRI procedure.
Characteristics of the Studied Group
In (Table 1), the number of people (eyes) is presented with a division into gender, type of lens surgery performed, preoperative visual acuity, and model of the implanted lens. Information concerning sex, number of cataract and LRI procedures, kind of refractive error, and all types of implanted intraocular lenses are also included.
| Sex | Numer of Eyes | % |
|---|---|---|
| female | 26 | 76,50 |
| male | 8 | 23,50 |
| Surgery Type | ||
| RLE | 24 | 70,60 |
| cataract | 10 | 29,40 |
| Preoperative Refractive Error | ||
| myopia | 26 | 76,50 |
| hyperopia | 8 | 23,50 |
| Intraocular Lens Model | ||
| Acunex Vario Max | 2 | 5,90 |
| Hanita Intensity | 6 | 17,60 |
| Liberty | 11 | 32,40 |
| M+Comfort | 1 | 2,90 |
| Panoptix | 3 | 8,80 |
| Soleko Evolve | 2 | 5,90 |
| Tecnis Symphony | 2 | 5,90 |
| Tecnis Synergy | 7 | 20,60 |
Table 1: The number of people (eyes) is presented with a division into gender, type of lens surgery performed, preoperative visua
Women made up over 76% of the assessed group, the RLE procedure was performed in over 70% of the eyes that underwent lens surgery, and 75.5% of the entire group were patients with preoperative myopia. The most frequently implanted lens was a model that combined a 3-focal diffractive design with an EDOF design.
Subjective Improvement in Vision
Only two patients (eyes) did not notice an improvement in the quality of their vision after undergoing the LRI procedure (Figure 2).
Descriptive Statistics
In (Table 2), descriptive statistics are presented for the studied group of N = 34 people, including mean, minimum and maximum values, as well as median values of age, time between lens implantation and LRI procedure, pupil diameter, astigmatism values, visual acuity measurement results and the number of letters by which visual acuity improved.
| Variable | N | M | SD | Min | Maks | Me | |
|---|---|---|---|---|---|---|---|
| Age (years) | 34 | 49,12 | 8,49 | 32,00 | 70,00 | 48,50 | |
| time between lens exchange and LRI (months) | 34 | 9,62 | 9,27 | 1,00 | 31,00 | 5,00 | |
| total astigmatism of the eye before lens exchange (dioptries) | 24 | 0,59 | 0,14 | 0,25 | 0,75 | 0,50 | |
| corneal astigmatism before lens exchnage in CT (dioptries) | 34 | 1,14 | 0,37 | 0,31 | 2,61 | 1,12 | |
| corneal astigmatism before LRI in keratometry (dioptries) | 34 | 1,24 | 0,51 | 0,25 | 3,25 | 1,25 | |
| Value of corneal astigmatism before LRI in CT (dioptries) | 34 | 1,36 | 0,44 | 0,75 | 3,25 | 1,25 | |
| BCVA to far (logMAR) before lens exchange | 34 | 0,17 | 0,18 | 0,00 | 0,60 | 0,10 | |
| BCVA to near (Snellen) before lens exchange | 34 | 0,50 | 0,00 | 0,50 | 0,50 | 0,50 | |
| UBVA to far (logMAR) before LRI | 34 | 0,24 | 0,11 | 0,10 | 0,50 | 0,20 | |
| UBVA to near (Snellen) before LRI | 34 | 0,53 | 0,12 | 0,50 | 1,00 | 0,50 | |
| UBVA to far (logMAR) after LRI | 34 | 0,11 | 0,11 | 0,00 | 0,40 | 0,10 | |
| UBVA to near (Snellen) after LRI | 34 | 0,50 | 0,00 | 0,50 | 0,50 | 0,50 | |
| An improvement (number of gained letters) | 34 | 6,32 | 4,82 | 0,00 | 20,00 | 5,00 | |
| Value of corneal astigmatism after LRI (dioptries) | 34 | 0,59 | 0,26 | 0,25 | 1,50 | 0,50 |
Table 2: Descriptive statistics including mean, minimum and maximum values, median values of age, time between lens implantati
N - number; M - mean; SD - standard deviation; Min - minimum; Max - maximum; Me - median CT - corneal topography; BCVA - best corrected visual acuity; UBVA - uncorrected best visual acuity Table 2: Descriptive statistics including mean, minimum and maximum values, median values of age, time between lens implantation and LRI procedure, pupil diameter, astigmatism values, visual acuity measurement results and the number of letters by which visual acuity improved.
The average time that elapsed from the moment of the lens replacement procedure to the LRI procedure was almost 10 months, ranging from 1 to 31 months. One patient (eye) who did not have a toric lens implanted despite having a corneal astigmatism value exceeding 2,61Dcyl underwent the LRI procedure, achieving a maximum value of 0,75Dcyl, and the improvement in distance visual acuity was 20 letters (logMAR).
Importantly, the average value of astigmatism generated by the entire optical system before lens exchange was 0.59, within the range of 0.25 to 0.75 Dcyl. Considering only this value, practically every patient could have a spherical lens implanted. Corneal astigmatism in the topography examination increased after the lens replacement surgery, from an average value of 1.14 to 1.36 Dcyl, despite following the same rules in the range of corneal incision.
When evaluating the effects in such a specific situation as the condition after performing the LRI procedure in eyes with multifocal lens implantation, several hypotheses were adopted.
Hypothesis 1
There is a significant change between the BCVA for distance, evaluated before the procedures (lens exchange and LRI) and the UBVA value obtained 1 month after the LRI procedure.
In order to check for a possible significant difference between the measurements in the areas covered by the examination, a non-parametric ANOVA Friedman test was used, comparing the mean values in the individual measurements. The results of the Friedman test (repeated measurements) are presented in (Table 3).
| Descriptive Statistics | ||||||||
|---|---|---|---|---|---|---|---|---|
| Visual Acuity (logMAR) | χ2 | df | p | M | SD | Min | Maks | Me |
| BCVA before lens exchange | 23,80 | 2 | < 0,001 | 0,17 | 0,18 | 0,00 | 0,60 | 0,10 |
| UBVA before LRI | 0,24 | 0,11 | 0,10 | 0,50 | 0,20 | |||
| UBVA after LRI | 0,11 | 0,11 | 0,00 | 0,40 | 0,10 |
Table 3: The result of the non-parametric Friedman ANOVA test showed statistically significant differences (p < 0.05) between
χ2 - test statistic; p - statistical significance; M - mean; SD - standard deviation; Me - median; Min - minimum value; Max - maximum value Table 3: The result of the non-parametric Friedman ANOVA test showed statistically significant differences (p < 0.05) between visual acuity measurements.
The performed test showed the presence of statistically significant differences (p < 0.05) between the measurements in the range of visual acuity. In order to accurately determine between which groups the differences are significant, a post hoc Bonferroni test - pairwise comparison - was conducted. Its results are presented in (Table 4).
| Corneal Astigmatism | Corneal Astigmatism | p | |
|---|---|---|---|
| corneal astigmatism before lens exchange in CT | corneal astigmatism before LRI | < 0,001 | *** |
| corneal astigmatism before lens exchange in CT | corneal astigmatism after LRI | < 0,001 | *** |
| corneal astigmatism before LRI | corneal astigmatism after LRI | < 0,001 | *** |
Table 4: The results of the Bonferroni test for pairwise comparison of results of corneal astigmatism obtained before CT and befo
* p < 0,05; p < 0,01; * p < 0,001; p – statistical significance Table 4: The results of the Bonferroni test for pairwise comparison of results of corneal astigmatism obtained before CT and before and after LRI.
The Bonferroni test showed that the visual acuity before the LRI procedure was statistically significantly different (p < 0.05) from the visual acuity before the lens exchange and after the LRI procedure. Before the operation, it was on average M = 0.17 (SD = 0.18), before the LRI procedure M = 0.24 (SD = 0.11), and after the procedure M = 0.11 (SD =
0.11). It was therefore demonstrated that the visual acuity before the LRI procedure was statistically significantly (p < 0.05) worse than before the lens exchange and after LRI.
The hypothesis was accepted. Visual acuity values were presented on a box (Figure 3a) and line plot (Figure 3b)
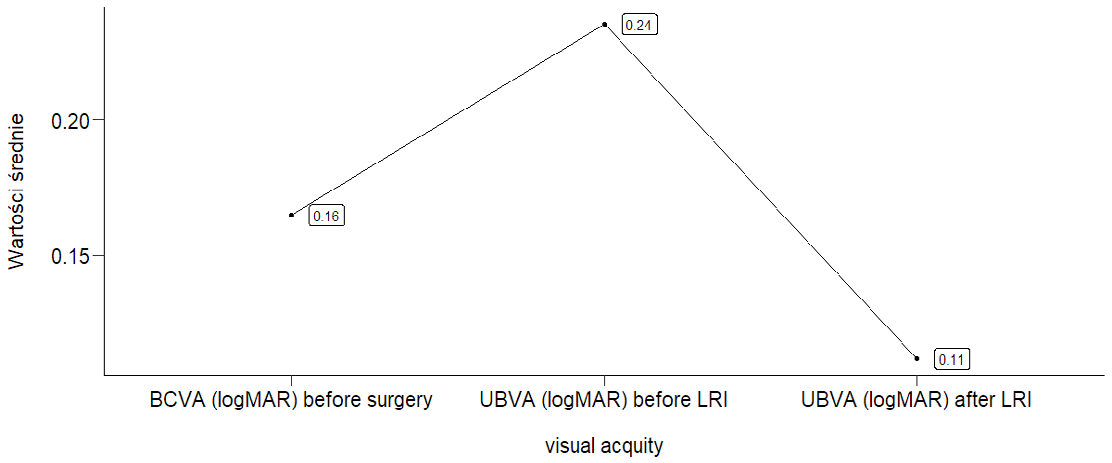
Figures 3: Graphical representation of distance visual acuity values obtained before the surgery (BCVA) and after the LRI procedure in the form of 3a) box plot and 3b) line chart. The improvement in vision after the surgery is statistically significant
Hypothesis 2
There is a significant difference between the value of astigmatism obtained before the lens exchange and LRI procedures, as assessed in corneal topography, and after the LRI procedure.
Descriptive statistics, including values of corneal astigmatism obtained before lens exchange and before and after LRI (Limbal Relaxing Incision), are presented in (Table 5).
| Descriptive Statistics | ||||||||
|---|---|---|---|---|---|---|---|---|
| Corneal Astigmatism | χ2 | df | p | M | SD | Min | Maks | Me |
| corneal astigmatism before lens exchange | 54,15 | 2 | < 0,001 | 1,14 | 0,37 | 0,31 | 2,61 | 1,12 |
| corneal astigmatism before LRI | 1,36 | 0,44 | 0,75 | 3,25 | 1,25 | |||
| corneal astigmatism after LRI | 0,59 | 0,26 | 0,25 | 1,50 | 0,50 |
Table 5: Values of corneal astigmatism obtained before lens exchange like also before and after LRI procedures The test showed th
χ2 - test statistic; p - statistical significance; M - mean; SD - standard deviation; Me - median; Min - minimum value; Max - maximum value.
Table 5: Values of corneal astigmatism obtained before lens exchange like also before and after LRI procedures The test showed the presence of statistically significant differences (p < 0.05) between the measurements in the range of astigmatism values. To accurately determine which groups, have significant differences, a post hoc Bonferroni test was conducted (Table 6).
| Corneal Astigmatism | Corneal Astigmatism | p | |
|---|---|---|---|
| corneal astigmatism before surgery in CT | corneal astigmatism before LRI | < 0,001 | *** |
| corneal astigmatism before surgery in CT | corneal astigmatism after LRI | < 0,001 | *** |
| corneal astigmatism before LRI | corneal astigmatism after LRI | < 0,001 | *** |
Table 6: The results of the Bonferroni test for pairwise comparison of results of corneal astigmatism obtained before CT and befo
* p < 0,05; p < 0,01; * p < 0,001; p – statistical significance Table 6: The results of the Bonferroni test for pairwise comparison of results of corneal astigmatism obtained before CT and before and after LRI procedure.
The Bonferroni test showed that the value of astigmatism was statistically significantly different (p < 0.05) in all measurements. Its value before lens implantation was M = 1.14 (SD = 0.37), before the LRI, M = 1.36 (SD = 0.44), and after it M = 0.59 (SD = 0.26). It was therefore shown that the value of corneal astigmatism was statistically significantly highest (p < 0.05) before the relaxing incision of the cornea, and statistically significantly lowest (p < 0.05) after the corneal incision procedure. The hypothesis was accepted.
Hypothesis 3
There is a significant correlation between the pre- operative pupil diameter and the post-operative UBVA to far distances (logMAR) in eyes that have undergone LRI procedure.
To analyze the probable correlation and assess the association between pupil size and postoperative uncorrected visual acuity (UBVA) to far distances, a Spearman correlation was used (Table 7).
UBVA to far (logMAR) after LRI
pupil size rho -0,059 p 0,742
- rho - Spearman correlation coefficient; p - significance level * p < 0,05; p < 0,01; * p < 0,001
Table 7: Analysis of the associations between pupil size and UBVA to far distances gained after LRI procedure.
No statistically significant correlation (p > 0.05) was found between the pupil diameter assessed preoperatively and UBVA after the LRI procedure. The mean pupil diameter value obtained in the study group was 4.8mm, with a range of 3.2mm to 5.7mm. The hypothesis was negatively verified, resulting in its rejection.
Visual Acuity to Near Distances
It was impossible to analyze changes in near visual acuity, as the same values were observed in all pre-implantation and post-relaxing incision observations (Figures 4 a & b).
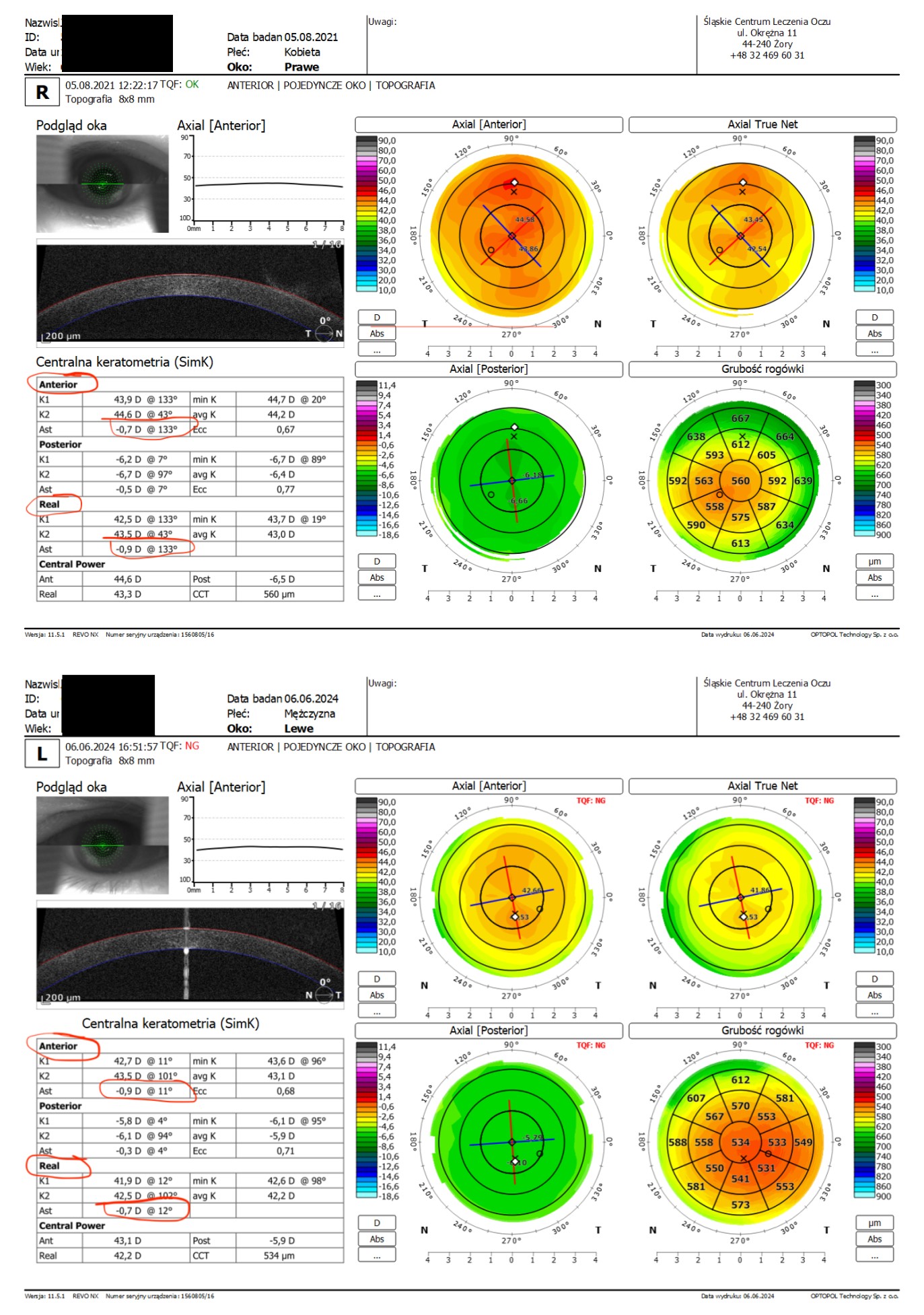
Figure 4a
Figure 4b
Figures 4: The result of the examination of the anterior and posterior curvature of the cornea in the range of its refractive power shows that: 4a) the posterior curvature causes an increase in the total value of corneal astigmatism 4b) the posterior curvature causes a decrease in the total value of corneal astigmatism. In both cases, the posterior surface of the cornea changes the astigmatism by only 0.2 diopters. The discussed values are marked with a red line. Own materials.
Discussion
Regarding the obtained results, it is worth discussing certain issues. One of them is the presence of to high as expected corneal astigmatism after lens exchange and its negative impact on vision. Despite the use of certain criteria for toric lens implantation in the studied group, postoperative astigmatism should be small enough to not have a negative impact on postoperative vision. However, the study results showed that it did have such an effect.
Furthermore, its value in the corneal topography examination increased after the lens replacement surgery. A two factor most likely contributed to this: the incorrect location of the main incision relative to the steep axis of astigmatism (despite its selection in the confrontational examination) and the failure to consider the possibility of an increase in its value due to the presence of astigmatism against the rule.
Therefore, it is better to adopt a general principle that astigmatism generated by the anterior surface of the cornea with a value of ≥ 0.75Dcyl should be corrected with the use of intraocular toric lens in every case of replacement, i.e., removal of the natural lens.
It should also be noted that multifocal lenses may slightly reduce the quality of vision in certain lighting conditions or when performing tasks that require very fine visual acuity, such as reading small print [6, 7]. This effect, in combination with unwanted corneal astigmatism, increases the negative postoperative effect. There is a positive and at the same time negative correlation between the decrease in visual acuity and the increase in the size of astigmatism after lens replacement surgery.
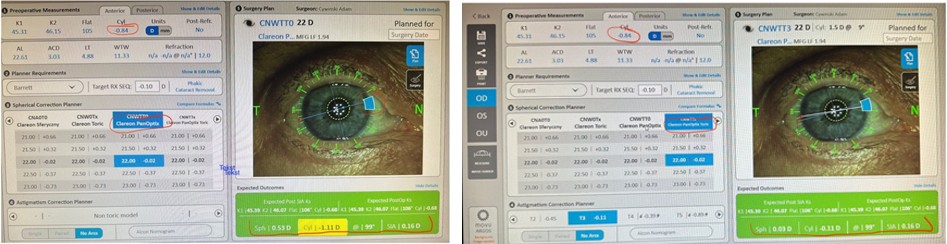
Several factors may influence this result, including removal of the natural lens, improper selection of the intraocular lens, i.e., a spherical model instead of a toric one, or the size and location of the corneal incision. It is worth mentioning that the main incision itself, depending on its size and location, may reduce or increase postoperative astigmatism [8, 9, 10]. Below samples of the two situations. .0 When qualifying for the selection of the appropriate lens model, devices that allow for preoperative simulation- planning of the main incision location gain importance (Figures 5 a & b).
Figure 5a Figure 5b
Figures 5: Two variants in the range of intraocular lens selection and the predicted postoperative refractive error after implantation of 5a) spherical lens and 5b) toric lens. The discussed values, including the type of lens and the predicted postoperative refractive error, are marked with a red line. Own materials.
Such preoperative simulation is even more significant when dealing with astigmatism that does not comply with the rule. In the studied group, a statistically significant improvement in visual acuity and quality of vision was achieved after LRI surgery. This result may indicate an inaccurate type of implanted lens, but also the need for a more precise selection of the main incision location.
The lack of influence of the pupil diameter size on the achieved visual acuity would seem unrealistic, since in the studied group, the range of pupil diameter values was from 3.2mm to 5.7mm. However, it should be mentioned that patients were “matched” with lens models based on the eye structure. Some of them, such as the Liberty® model from Medicontur® give favorable postoperative results in the range of distance and near vision, despite the presence of a wide pupil [11].
When analyzing the values of postoperative astigmatism of the entire optical system, it should be noted that lenses with a complex structure can also generate “artificial” astigmatism, which is shown by devices used in refractometry measurement [12]. Correction of such artificial astigmatism is therefore pointless. It is better to focus on correcting corneal astigmatism.
Conclusions
Corneal astigmatism generated by the anterior surface, with an average value of 1.36 D cyl, was found after the implantation of a spherical multifocal lens and has a negative impact on both the quality of vision and visual acuity.
Using the technique of Limbal Relaxing Incision, a reduction of corneal astigmatism by an average value of 0.77 Dcyl was achieved, which in consequence allowed to obtain an average value of 0.59 Dcyl.
The reduction of corneal astigmatism allowed for a subjective improvement in the quality of vision in over 92% of patients and a statistically significant improvement in distance visual acuity from an average value of 0.24 to a value of 0.11, assessed on logMAR charts.
The obtained results suggest that the choice of a toric intraocular lens should be made when the value of corneal astigmatism, generated by its anterior surface, is at least 0.75Dcyl. The lack of influence of the pupil diameter on the visual acuity obtained after the LRI procedure resulted from the fact of the proper selection of the multifocal lens model in relation to the structure of the eyeball.
Acknowledgments
The authors express their gratitude to all those who contributed to the creation of this article, including: technicians who performed the examinations, optometrists who prepared patients for the examination, the statistician who conducted the statistical analysis, and all other unnamed individuals.
References
-
Nichamin LD, Steinert RF, Wallace III RB (2009) Corneal Relaxing Incisions cover stories | cataract and refractive surgery today.
-
Nichamin LD (2014) Limbal Relaxing Incisions: A Practical Guide. SLACK Incorporated.
-
Villegas EA, Alcón E, Artal P (2014) Minimum amount of astigmatism that should be corrected. Journal of Cataract & Refractive Surgery 40(1): 13-19.
-
Hayashi K, Manabe S, Yoshida M, Hayashi H (2010) Effect of astigmatism on visual acuity in eyes with a diffractive multifocal intraocular lens. J Cataract Refract Surg 36(8): 1323-1329.
-
Mohammadi SF, Khorrami Nejad M, Hamidirad M (2019) Posterior corneal astigmatism: a review article. Clin Optom (Auckl) 11: 85-96.
-
Al-Shymali O, McAlinden C, Barrio JLAD, Canto-Cerdan M, Alio JL (2022) Patients’ dissatisfaction with multifocal intraocular lenses managed by exchange with other multifocal lenses of different optical profiles. Eye Vis (Lond) 9(1): 8.
-
Vega F, Alba-Bueno F, Millán MS, Varón C, Gil MA, et al. (2015) Halo and Through-Focus Performance of Four Diffractive Multifocal Intraocular Lenses. Invest Ophthalmol Vis Sci 56(6): 3967-3975.
-
Chen JS (2019) Effect of corneal incision location on astigmatism after cataract surgery. Journal of Cataract and Refractive Surgery 45(1): 75-80.
-
Wei YH, Chen WL, Su PY, Shen EP, Hu FR (2012) The influence of corneal wound size on surgically induced corneal astigmatism after phacoemulsification. J Formos Med Assoc 111(5): 284-289.
-
Piao J, Joo CK (2020) Site of clear corneal incision in cataract surgery and its effects on surgically induced astigmatism. Sci Rep 10(1): 3955.
-
Cywinski A, Bazgier P (2024) Liberty® by Medicontur, a Complex in Structure, Hydrophilic Intraocular Lens in the Correction of Eyes with Preoperative Myopia. Austin J Clin Ophthalmolol 11(1): 1173.
-
Cywinski A, Bloch D, Lubczyk A (2022) Assessment of the Value of Astigmatism Generated by Two Models of Spherical Multifocal Lenses: Panoptix® by Alcon® and Acunex® Variomax® by Teleon® using the Toric Alignment Check Module of the Itrace Analyser. Open Access Journal of Ophthalmology 7(2): 1-10.
- Screening of Hospital Staff During World Glaucoma Week in a Tertiary Eye Care Centre
- Angioid Streaks with Macular Neovascularization: Clinical Insights from Two Cases
- Giant Kissing Naevus: An Oculoplastic Challenge
- Why Freedom of Vision Should Not Cost the Freedom of Feeling - LASIK in the Climate of Change
- Asymmetric Optic Nerve with Small Disc and Large Cup: A Rare and Challenging Case of Unilateral Optic Nerve Hypoplasia
- Large Angle Exotropia in a Child: A Case Report