Isolated Renal Metastasis Mimicking Primary Renal Cell Carcinoma
The majority of isolated renal masses are found to be primary renal cell carcinoma. However, in some rare cases, such a presentation can reveal an underlying metastasis of an occult neoplasm elsewhere. We report here a case of papillary thyroid carcinoma that presented as an isolated renal mass in an 80-years-old woman with no history of thyroid cancer. The patient underwent a radical nephrectomy by laparoscopy after a negative extension work-up for a suspected primary RCC. Pathology later confirmed it as a metastasis of papillary thyroid carcinoma, prompting a thyroid biopsy, which came back positive. PET scan showed no other metastasis, prompting total thyroidectomy and adjuvant 200mCi of I131. As of today, she remains in complete remission. In the presence of a large isolated renal mass, clinicians should remain suspicious of potential metastatic disease as it can allow for early detection and management of the primary neoplasm
Introduction
In the contemporary setting of more accessible and affordable CT scans, incidental findings of renal mass have become increasingly prevalent [1]. Primary renal carcinoma represents the vast majority of isolated renal mass, while benign pathologies decrease in frequency as mass size increases. Nonetheless, metastases to the kidneys remain an important consideration in the clinician’s differential, representing up to 0.9%of cases. In some rare cases, it is the earliest and only manifestation of an occult primary neoplasm. In this case report, we describe a case of papillary thyroid cancer presenting as a solitary renal mass.
An 80-year-old woman presented with an asymptomatic cystic right renal mass, discovered incidentally during abdominal CT scan in the context of acute diverticulitis. Her medical history included a recent thyroiditis, chronic atrial fibrillation, coronary artery disease, pulmonary hypertension, diabetes, dyslipidemia, left Bell’s palsy and hypertension. She also had undergone total hysterectomy with bilateral salpingo-oophorectomy, right total knee replacement and bilateral blephonoplasty. The patient denied any tobacco use. She reported losing 10 kg in the last 2 months following her thyroiditis and acute diverticulitis.
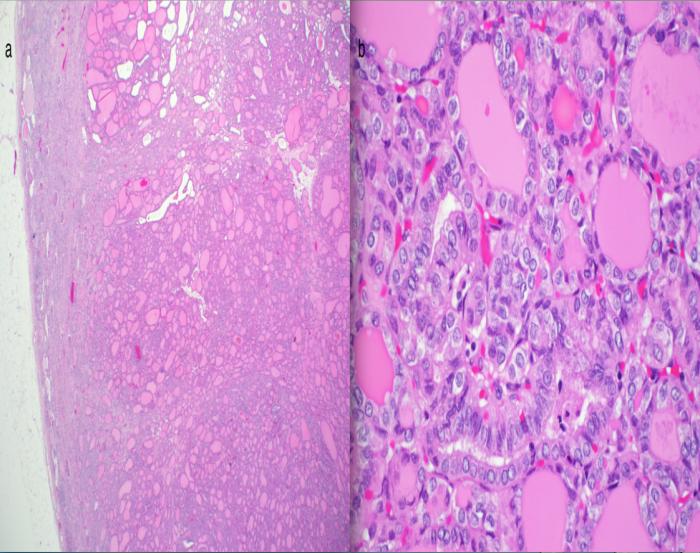
Her physical examination did not reveal anything significant, including no neck nodule according to her endocrinologist. A multiphasic CT scan revealed an isolated 4 x 4.2 cm complex cystic mass of the superior pole of her right kidney, suspicious of a primary renal cell carcinoma (Figure 1). The cystic component as well as the size of the lesion refrained us from opting for a biopsy. Laparoscopic radical nephrectomy was scheduled after a complete workup, including proper labs and imagery (thoracic CT/Chest X-Ray), which were normal. Surgery and her post-operative course were uneventful. Surprisingly, pathology revealed a follicular subtype of a papillary thyroid carcinoma. Thyroid-like primary renal carcinoma was also considered as a possible diagnosis. Immunohistochemical staining, with positive thyroglobulin and TTF-1, favored a tumour of thyroid origin (Figure 2).

The patient was directed to her ENT specialist. Upon further investigation, a 3.3 cm hypoechoic left thyroid nodule was found by ultrasound. Biopsy confirmed the presence of a papillary carcinoma of follicular variant. With a FDG PET scan negative for other metastasis, a total thyroidectomy was scheduled, which revealed 2 malignant nodules of well-differentiated papillary carcinoma of follicular variant without lymph-vascular invasion. Margins and lymph nodes were negative. Ten weeks later, the patient was treated with adjuvant 200mCi of I131. An I131 scintigraphy performed shortly after showed multiple abnormal capitation sites in the lungs and mediastinum. However further investigation of these sites by chest CT scan did not demonstrate any disease.
Discussion
Thyroid metastasis to the kidney is a rare occurrence that is documented in less than 40 cases in the English literature [2]. Discovery of the primary thyroid cancer by an incidental detection of a kidney metastasis, such as in the case presented here, is an uncommon presentation, as most metastasis are found in the context of previously known thyroid cancer or full-blown multi-systemic metastatic disease [3]. In those rare patients where the kidney mass is detected first, they are either asymptomatic [4] or present with kidney-specific symptoms such as hematuria and flank pain [3]. Such presentation is of course also compatible with renal cell carcinoma [1]. In the present case, the patient was completely asymptomatic, with no history of kidney disease or previous cancer. She did present with thyroiditis one month before the detection of her renal mass, with a hypo echoic zone in the left thyroid. It is unclear whether this episode is related to her thyroid carcinoma, as thyroid cancer does not typically present with hyperthyroidism. The ENT doctor did not suspect the presence of a thyroid tumour due to this unusual presentation. Management of her renal mass, believed to be a primary renal cell carcinoma, was a radical nephrectomy. In the case of an isolated renal mass, such a management is adequate as it provides both treatment and definitive diagnosis [5, 6]. Complete resection of metastasis is also the recommended conduct in thyroid carcinoma with a solitary metastasis, as it provides a statistically significant increase in survival [7]. Pathology of the excised kidney was vital. It directed the diagnosis toward a thyroid carcinoma metastasis and prompted appropriate investigations. The main other differential diagnosis is thyroid-like follicular carcinoma of the kidney, which is an even rarer entity [2]. The treatment of the later- discovered thyroid primary tumour was standard, with total thyroidectomy and single dose radio-iodine. The final outcome is positive: as of today, the patient showed no signs of cancer spread and remains asymptomatic. The main purpose of reporting this case resides in alerting clinicians to this uncommon presentation. Even with less than 1% of kidney masses being metastasis, it remains an important diagnosis to consider as it allows early detection of the primary tumour. Other sites of origin, such as colon or bladder, have presented in the same fashion in the past [8]. FDG PET scan could help if the renal mass is thought to be secondary [6]. It is however not part of the routine evaluation of a renal tumour since sensitivity and specificity are low with renal carcinoma. Performing a mass biopsy would identify the presence of a metastasis and allow earlier control of the primary site as well as a planned management according to the appropriate diagnosis. However, if no other metastases were present, mass excision followed by a proper treatment of the primary site would be considered adequate management [7]. In summary, clinicians should maintain a high level of suspicion for any signs of another primary neoplasm in presence of an isolated renal mass, since solitary renal metastasis is a great mimicker of primary renal cell carcinoma.
References
-
Skinner DG, Colvin RB, Vermillion CD, Pfister RC, Leadbetter WF (1971) Diagnosis and management of renal cell carcinoma. A clinical and pathologic study of 309 cases. Cancer 28(5): 1165- 1177.
-
Wu WW, Chu JT, Nael A, Rezk SA, Romansky SG, et al. (2014) Thyroid-likefollicularcarcinoma of the kidney in a young patient withhistory of pediatric acute lymphoblasticleukemia. Case Rep Pathol 2014: 313974.
-
Falzarano SM, Chute DJ, Magi-Galluzzi C (2013) Metastatic papillary thyroid carcinoma to the kidney: report of two cases mimicking primary renal cell carcinoma and review of the literature. Pathology 45(1): 89-93.
-
Ruggiero FP, Frauenhoffer EE, Stack BC Jr (2005) Papillary thyroid cancer with an initial presentation of abdominal and flank pain. Am J Otolaryngol 26(2): 142-145.
-
Dechet CB, Zincke H, Sebo TJ, King BF, LeRoy AJ, et al. (2003) Prospective analysis of computerizedtomography and needlebiopsywith permanent sectioning to determine the nature of solidrenal masses in adults. J Urol 169(1): 71-74.
-
Ramdave S, Thomas GW, Berlangieri SU, Bolton DM, Davis I, et al. (2001) Clinical role of F-18 fluorodeoxyglucose positron emissiontomography for detection and management of renal cell carcinoma. J Urol 166(3): 825-830.
-
Shaha AR, Shah JP, Loree TR (1997) Differentiated thyroid cancer presenting initially with distant metastasis. Am J Surg 174(5): 474-476.
-
Patel U, Ramachandran N, Halls J, Parthipun A, Slide C, et al. (2011) Synchronous renal masses in patients with a nonrenal malignancy: incidence of metastasis to the kidney versus primary renal neoplasia and differentiating features on CT. AJR Am J Roentgenol 197(4): W680-686.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report