Penile Calciphylaxis: Report of Two Cases
<p>Report two cases of patients with multiple comorbidities including chronic kidney disease (CKD) and renal replacement therapy who develop penile calciphylaxis and were taken to partial penectomy. Resulting in improvement of pain scores and necrotic lesions in penis.</p>
Objective
Report two cases of patients with multiple comorbidities including chronic kidney disease (CKD) and renal replacement therapy who develop penile calciphylaxis and were taken to partial penectomy. Resulting in improvement of pain scores and necrotic lesions in penis. Keywords: Penile Calciphylaxis; Case report; Calcificuremicarteriolopathy
Introduction
Calciphylaxis or calcific uremic arteriolopathy is a rare but life threating condition that is present in 1% of patients with chronic renal disease [1]. It´s presents as skin ulceration and necrosis that leads to significant pain in the affected area. The penis is an extremely rare site for calciphylaxis due to its rich blood supply. Histopathologic examination shows medial calcification and intimal proliferation of small arterioles and subcutaneous capilaries, leading to thrombosis and ischemic necrosis [2]. The first literature review involving the penis was in 1997 and included 10 cases. Up until 2007 38 cases have been reported with mortality rates of 64% 6 months after diagnosis [3].
The diagnosis of systemic calciphylaxis is an association of clinical features in patients with CRD who have painful genital ulcer with or without serum calcium elevation; some patients may have higher calcium phosphate levels (78.5 mg/dl) [4]. A wide variety of imaging studies have been suggested ranging from ultrasound to penile arteriography which aims to evaluate vascular permeability and associated perivascular deposits.
Case 1
Male patient 59 year of age with CKD stage 5 in renal replacement therapy 3 times a week, type 2 diabetes and arterial hypertension, presents with several weeks of painful white plaques on the glans associated with perilesional edema and very small areas of necrosis. Initial management is with a urinary catheter and daily bandage changes. 30 days after the initial consult the patient returns with a worsening clinical presentations consisting of increased pain scores, changes in skin coloration and increase of the necrotic area, because of the rapid progression of disease a partial penectomy is performed with satisfactory results and good postoperative course.


Case 2
Male patient, 62 years of age with CKD stage 5 in renal replacement therapy 3 times a week type 2 diabetes and arterial hypertension, is hospitalized in the context of a probable coronary syndrome. During which ulcerative lesions in the glans and balanopreputial groove appears, painful to touch with no appreciable smell of discharge with apparent necrosis. Because of the multiple comorbidities and findings in the physical examination microangiopathic lesions are considered and a penile vasculature doppler ultrasound is performed which reports calcific uremic arteriolopathy. In this patient medical treatment was considered because of his poor general state and high risk of complications. When medical treatment fails because of increasing pain scores and increased area of lesions, purulent discharge and extension of necrotic areas to the urethral meatus a partial penectomy is performed leading to diminished pain excellent postoperative evolution and improvement of lesions. The pathology specimens confirm penile calciphylaxis.


Discussion
Calciphylaxis was described initially by Bryant and White who describe an association between cutaneous gangrene and vascular calcification [2]. It typically presents with ischemic necrosis which involves areas with abundant adipose tissue like the anterior abdomen and back, buttocks and proximal extremities. It also may present in areas with little or no adipose tissue like distal extremities (digital ischemia of hands and feet) and very rarely the penis [1]. Patients with alterations in the calcium and phosphorus metabolism, type 2 diabetes and other metabolic pathologies are closely related. It is almost exclusive of patients with stage 5 CKD in some form of dialysis because of the resulting secondary hyperparathyroidism which in turn causes excessive calcification of small and medium caliber arteries and is considered the principal risk factor in developing the disease [4].
Normally the arterial supply of the penis is through the internal iliac artery and internal branches of the pudendal artery from which the common penile artery arises finalizing in the dorsal and cavernous arteries of the penis [2]. This extensive collateral supply protects the penis from ischemic gangrene unlike the heart and lower extremities. It is believed that isolated penile gangrene is a focal manifestation of diffuse arterial calcification observed in CKD which is further aggravated by type 2 diabetes when it is present. It is extremely rare as only 38 cases have been reported worldwide [3].
Calciphylaxis is known by different names including calcific uremic arteriolopathy; it develops in 1-4% of patients with CKD. There are currently many theories explaining its pathogenesis in which secondary hyperparathyroidism, persistent elevation of seric phosphorus and the increase in the product of calcium- phosphorus play an integral part in the calcification, some patients have increased expression of osteopontin bone matrix protein by vascular smooth muscle cells that may initiate and potentiate vascular calcification [4].
Clinically it presents as severe livedo reticularis that progresses painful ischemic ulceration of the skin which is caused by the overlapping thrombosis of involved arteries, thus causing large areas of necrosis in a matter of days. Penile gangrene caused by calcifilax is has high mortality rate. Bacterial proliferation under the ulcer causing infection and sepsis thus explaining the high mortality rate (60-80%) associated with this pathology [1].
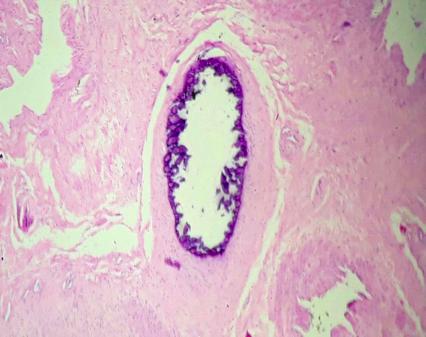
Within the radiological findings, the use of Doppler ultrasound can visualize hyperechogenicity of the walls of the cavernous arteries; a finding that indicates a calcification of the same, and no flow inside is detected [3]. These diagnostic aids can be useful and suggest the diagnosis, tissue biopsy remains the gold standard, where you can visualize affected areas with characteristic lesions of calcification of small vessels (capillaries, venules and arterioles), endovascular fibrosis, panniculitis (inflammation of subcutaneous fat) and consequent tissue necrosis, in addition to thrombosis, with obliterating vasculopathy being the main contributing factor to necrosis [2]. Treatment of calciphylaxis is generally unsuccessful and mostly supportive. Local care is very important to prevent the development of secondary infections, as well as the use of powerful analgesics for pain control. The use of drugs such as Cinacalcet as calcium-receptor stimulating agent, leads to a rapid correction of serum levels of calcium and phosphate, parathyroid hormone and alkaline phosphatase, being potentially valuable, particularly for those patients who are not candidates for parathyroidectomy [5]. The surgical treatment of necrotic lesions of the penis is also discussed. Wood et al recommended penectomy, while others believe that local wound care and debridement of lesions are sufficient. In the presence of infection, aggressive surgical treatment or penectomy is often required for any chance of survival. In a review, no statistically significant differences in survival were demonstrated between patients treated with penectomy (50%) and those treated with local treatment of wounds and bridges (32%). Whenever penectomy is considered in the non-infected patient, the psychological consequences of emasculation should be considered. Penectomy in the uninfected patient should only be considered in the presence of severe pain refractory to analgesics [3].
References
-
Bhatty TA, Riaz K (2009) Calciphylaxi smimicking penile gangrene: A Case Report. Scientific world journal 6(9): 1355-1359.
-
Bappa A, Hakim F, Ahmad M, Asirri A (2011) Penile gangrene due to calcific uremic arteriopathy. Ann Afr Med 10(2): 181-184.
-
Shiraki T, Lida O, Okamoto T, Ishihara T, Fujita M, et al. (2015) Usefulness of endovascular therapy for penile gangrene secondary to calciphylaxis: A case report. Ann Vasc Surg 29(7): 1451.e11-15.
-
Mayank M, Shrawam K, Arup K (2007) Penile gangrene in diabetes mellitus with renal failure: A poor prognostic sign of systemic vascular calciphylaxis. Indian J Urol 23(2): 208-210.
-
Zapata F, Del Rio D, Ruiz A (2013) Calcifilaxis: Reporte de un caso. Revista CES MEDICINA 27(2): 235-241.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report