Paratesticular Rhabdomyosarcoma: About 3 Cases and Literature Review
Paratesticular rhabdomyosarcoma is a rare and highly aggressive embryonal tumor in infancy and childhood. The tumor is intrascrotal, localized in the spermatic cord, the epididymis, or in the tunica vaginalis. Multimodality treatment should involve surgery, radiotherapy and chemotherapy, which are indicated according to risk groups. Prognosis is excellent for localized tumors, survival rates exceed 90%. We report three cases of embryonal paratesticular rhabdomyosarcoma treated in our institution.
Introduction
Rhabdomyosarcoma is a rare malignant mesenchymal tumor developed at the expense of connective tissues, of which the genitourinary localizations are among the most frequent [1]. They represent 10% of intra scrotal tumors in children. The embryonic variant is the most common [2]. The diagnosis is suspected by ultrasound and confirmed by pathological examination of the surgical specimen of the orchiectomy [3]. The prognosis is poor, and treatment relies on tripod surgery, chemotherapy and radiotherapy.
Observations
Case 1
Young man of 21 years old, without particular antecedents, consults for a large painless right mass evolving for approximately 4 months. Clinically, the scrotum was enlarged, with a mass apparently independent of the testis, hard in consistency, painless on palpation and without signs of inflammation (Figure 1). Ultrasound exam shows a large intrascrotal tissue mass of heterogeneous structure, echogenic, with small areas of necrosis, a pelvic MRI was done and revealed a heterogeneous mass of scrotal tissue infiltrating the scrotal skin, without invasion of the testes. The dosage of tumor markers (HCGt, AFP, LDH) was normal. The patient underwent inguinal tumerectomy, radio-chemotherapy followed by lumbar- aortic lymphadenectomy.

Case 2
18-year-old man, with no particular pathological history, consults for a left scrotal tumefaction that has been evolving for 7 months. Hormonal dosing was found to be normal. The ultrasound showed a tissue mass of 08 cm, pushing back the left testicle. The patient underwent an orchiectomy by the upper route that found paratesticular rhabdomyosarcoma. Adjuvant chemotherapy for 3 sessions after the surgical treatment was followed by lumbo-aortic lymph node dissection.
Case 3
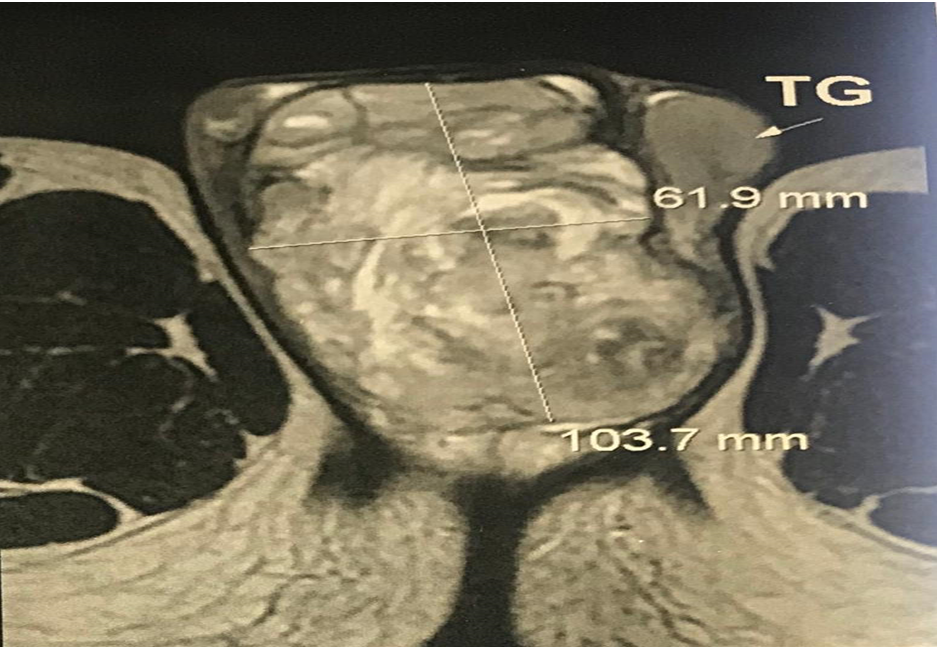
17-year-old patient, with no particular pathological history, consults for a large painless mass for a period of 8 months, gradually increasing in volume. Clinical examination reveals a hard, multi-lobed scrotal mass 10 cm in diameter. The ultrasound examination showed a large tissue mass, pushing outside the two testes. MRI shows a heterogeneous tissue process hyperintense in T2 in contact with the testis without any sign of invasion with the presence of inguinal lymphadenopathy Figure 2. The tumor markers were normal. A biopsy was performed objectifying a rhabdomyosarcoma. The patient received three courses of neoadjuvant chemotherapy followed by inguino-scrotal tumerectomy. Histological examination showed embryonic rhabdomyosarcoma with round cells from the paratesticular region.
Discussion
Paratesticular rhabdomyosarcoma can occur at any age, especially in children and young adolescents. There are two peaks of incidence between the ages of 2 to 5 years and adolescence [2]. Paratesticular location represents 7% of rhabdomyosarcomas, all locations combined [2, 3]. It develops from the mesenchymal tissues of the spermatic cord, epididymis and testicular tunics. The clinical discovery of paratesticular rhabdomyosarcoma is often incidental, revealing a painless intrascrotal mass [3]. In an acute bursa, diagnosis is sometimes difficult due to the presentation often confusing with testicular torsion.
The testicular examination should be bilateral and careful. It eliminates the main causes of painless large bursa including hydrocele, cord cyst, epididymitis or inguino- scrotal hernia which could lead to detrimental delay in diagnosis. The paratesticular site of the tumor is difficult to determine by palpation of the scrotum [4], the test is being difficult to identify.
Testicular ultrasound is performed first, making it possible to objectify the intrascrotal mass, developed at the expense of the testicular envelopes. The testicle is most often intact [1]. This examination shows a mass of tissue density, heterogenic, intrascrotal, and developed at the expense of the testicular envelopes. The testicle is most often normal. If the ultrasound confirms the presence of a tumor, the dosage of seric markers (α-fetoprotein, total HCG, carcinoembryonic antigen) must be carried out before any treatment. In the case of embryonic tumors, the tumor markers are usually normal. Diagnostic confirmation is then based on pathological examination of the inguinal orchiectomy piece, revealing rhabdomyoblasts that characterize the rhabdomyosarcoma [3].
Distant extension is done through the lymphatic and hematologic route. The retroperitoneal lymph nodes represent the first lymph node relay [5]. Lumbo-aortic lymph node involvement is reported in 26% to 43% of cases. The lung, liver and bone are the most common sites of metastasis [4]. Thoraco-abdominal-pelvic scanography contributes to the assessment of the distant extension of the disease. It makes it possible to explore the pelvic and lumbo-aortic lymph node areas, to look for hepatic and / or pulmonary metastases [6]. Bone scintigraphy looks for secondary bone locations [2]. MRI is useful in cases of significant locoregional extension to better appreciate the relationship of the tumor to the pelvic organs [7]. FDG (fluorode-soxyglucose) PET scans are used in the assessment of the extension of sarcomas in adults, but their use is very limited in the pediatric population [3]. A few pediatric publications have provided a better appreciation of the locoregional lymph node extension and the detection of occult metastases with PET scans [7].
The early diagnosis and surgical treatment are essential for the prognosis [2]. The therapeutic strategy is defined in agreement with the patient and his parents on the basis of an opinion delivered in multidisciplinary consultation. The treatment is surgical, combined with chemotherapy and / or radiotherapy. The orchiectomy is inguinal with first ligature and upper ligature of the spermatic cord. The value of systematic lymph node dissection has been very controversial since the publication of SIOP [8]. Para- aortic lymph node dissection does not seem necessary in localized forms [5]. Wienerm, et al. [9] reported 14% of histological lymph node involvement in patients without signs of radiological involvement, while 94% of patients with large lymphadenopathy on CT had histological lymph node metastases after retroperitoneal lymphadenectomy. The considerable morbidity of lymph node dissection must be weighed against the risk of recurrence. In this case, multidrug therapy makes it possible to eradicate the occult metastases. It is indicated for all prognostic groups with a significant improvement in the probability of overall survival and progression-free survival. Radiotherapy, which is not systematic, is used as a therapeutic complement on residual focus in advanced forms, on retroperitoneal lymph nodes or on metastases, especially pulmonary ones. The IRS recommends irradiation of the lumbar-aortic and iliac chains for stage 2, 3 and 4 tumors at a rate of 40 to 50 Gy over five to six weeks [10].
Conclusion
Testicular rhabdomyosarcoma is a rare tumor and a therapeutic and diagnostic emergency. Its management is multidisciplinary. Localized forms have a favorable prognosis and mul-timodal treatment leads to excellent survival rates based on the combination of chemotherapy, radiotherapy and surgery.
References
-
Cawson RA (1995) Soft tissue tumors. In: Enzinger FM, et al. (Eds.), Mosby, St Louis, £160. 3rd (Edn.), European Journal of Cancer Part: B Oral Oncology 31(6): 405.
-
Dasgupta R, Rodeberg DA (2012) Update on rhabdomyosarcoma. Semin Pediatr Surg 21(1): 68-78.
-
Faurea A, Diakite ML, Panait N, Chaumoitre K, Rome A et al. (2012) Paratesticular rhabdomyosarcoma in children: A scrotal Emergency. Arch Pediatr 19(12): 1340-1344.
-
Slama A, Jaidane M, Ben Sorba N (2000) Le rhabdomyosarcome paratesticulaire. Prog Urol 10: 1232-1234.
-
Reeves HM, MacLennan GT (2009) Paratesticular rhabdomyosarcoma. J Urol 182(4): 1578-1579.
-
Rodeberg D, Paidas C (2006) Childhood rhabdomyosarcoma. Semin Pediatr Surg 15(1): 57-62.
-
Tateishi U, Hosono A, Makimoto A, Nakamoto Y, Kaneta T, et al. (2009) Comparative study of FDG PET/CT and conventional imaging in the staging ofrhabdomyosarcoma. Ann Nucl Med 23: 155-161.
-
Mody RJ, Bui C, Hutchinson RJ, Yanik MD, Greg A, et al. (2010) FDG PET imaging of childhood sarcomas. Pediatr Blood Cancer 54(2): 222-227.
-
Wiener ES, Lawrence W, Hay D, Lobe TE, Andrassy R, et al. (1994) Retroperitoneal node biopsy in paratesticular rhabdomyosarcoma. J Ped Surg 29(2): 171-177.
-
Meza JL, Anderson J, Pappo AS, Meyer WH (2006) Analysis of prognostic factors in patients with nonmetastatic rhabdomyosarcoma treated on intergroup rhabdomyosarcoma studies III and IV: the children’s oncology group. J Clin Oncol 24(24): 3844-3851.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report