A Rare Primary Renal Lymphoma with Liver and Adrenal Gland Metastasis: A Case Report
Extra-nodal lymphomas include about 25%–35% of non-Hodgkin lymphomas (NHL), with the most frequent sites being the skin, small intestine, and stomach. Renal involvement by a lymphomatous tumor is rare, the majority of these tumors are non- Hodgkin lymphomas and in more than 90% of cases this renal location is secondary. This neoplasm is frequently misdiagnosed initially as renal cell carcinoma. In this article we report a very unusual case of primary renal lymphoma (PRL) with hepatic and adrenal gland metastases in a 65-year-old woman.
Introduction
Renal adenocarcinoma represents the most common histological form of kidney cancer in adults. Renal involvement by a lymphomatous tumor is rare, the majority of these tumors are non-Hodgkin lymphomas (NHL) and in more than 90% of cases this renal location is secondary [1]. Lymphomas that occur outside the lymph nodes, known as extra-nodal lymphomas, constitute approximately 25%–35% of NHL. The skin, small intestine, and stomach are among the most common sites for these extra-nodal lymphomas [2].
One of the exceedingly rare primary sites for NHL is the renal region, constituting only 0.1–0.7% of cases, and diffuse large B cell lymphoma (DLBCL) representing the most dominant histopathological type [3]. This neoplasm is frequently misdiagnosed initially as renal cell carcinoma [1].
Patients with primary renal lymphoma (PRL) may present with nonspecific symptoms, such as abdominal pain, lower back pain, fever, hematuria. In this article we report a very unusual case of PRL with hepatic and adrenal gland metastases in a 65-year-old woman.
A 65-year-old woman, treated for hypothyroidism, presented with left flank pain without hematuria or fever. An abdominal ultrasound revealed a tissue mass on the upper pole of the left kidney, 12 cm long.
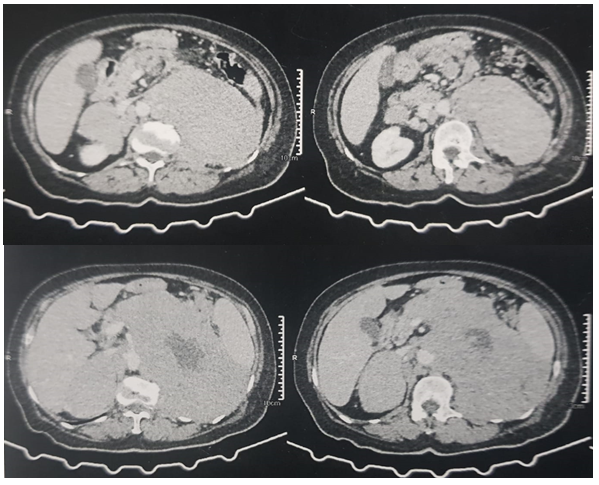
An abdomino-pelvic CT scan showed:
- A voluminous mass in the upper pole of the left kidney, estimated at 16.5 cm in height, 13.8 cm in transverse long axis and 15 cm in anteroposterior diameter, with endophytic and exophytic development, irregular contours, heterodense, heterogeneously enhancing after injection of contrast, delimiting a hypodense zone of central necrosis Figure 1.
- The left adrenal gland was not seen.
- A voluminous right adrenal mass, measuring 8.4 x5 cm.
- Hepatic nodule in segment VI of the liver, hypodense, non-enhanced after injection of PDC, measuring 10mm in diameter.
Laboratory work-up: methoxylated derivatives were normal, hemoglobin 12 g/dl, white blood cells 8000/mm3, platelets 320,000/mm3, the rest of the laboratory work-up was normal.
An echoguided left renal biopsy was performed; the histopathology and immunohistochemistry studies showed that the tumor cells expressed CD20 diffusely and homogeneously. CD3 marked the reaction lymphocytes. CD10 was negative. BCL6 marked 60% of the tumor cells. Ki67 showed an elevated proliferation index.
The decision of the multidisciplinary consultation meeting was to initiate chemotherapy according to the R-CHOP protocol. The patient died before starting chemotherapy due to respiratory distress.
Discussion
Lymphomatous involvement of the kidney is a rare occurrence. It is typically a result of direct extension from retroperitoneal lymph nodes or through the hematogenous route [1]. Primary renal lymphoma (PRL) is more common in men than women within an age range of 45-65 years, and bilateral renal involvement has been seen in up to 20% of patients [4].
The exact cause of PRL is unknown, as the kidney is an extranodal organ without lymphatic channels. There are several theories that attempt to explain the development of lymphoma in the kidneys. One theory proposes that PRL originates in the lymphatic vessels of the renal capsule and then spreads to the renal parenchym. Another possibility is the hematogenous spread of the disease, where the cancer cells travel through the bloodstream to reach the kidneys [3].
The symptoms of PRL are similar to other renal masses and include hematuria, flank pain, and a palpable mass on the flank or abdomen, our patient was suffering from abdominal pain. The CT scan findings, however, are not specific, making distinction much more challenging. Unusual abnormalities on a CT scan, such as hypovascularity, numerous renal nodules, homogenous renal enlargement without palpable mass, or bilateral renal mass, may be signs that a fine-needle renal biopsy should be performed prior to surgery [5].
Immunohistochemical analyses commonly reveal the presence of CD20, BCL6, and BCL3, which indicate B-cell proliferation in this context. The histological picture in primary renal non Hodgkin lymphoma is either a heavy interstitial infiltrate of lymphoma cells with an expanded interstitium, or glomerular infiltration which can be mistaken with a pseudo-proliferative glomerulonephritis [5].
The standard treatment regimen for PRL, especially the DLBCL subtype, typically includes Rituximab, Cyclophosphamide, Doxorubicin Hydrochloride, Vincristine Sulfate, and Prednisone (R–CHOP), often in conjunction with nephrectomy [5].
R–CHOP has shown better outcomes in terms of survival probability compared to CHOP alone [6]. However, the median survival for PRL is still relatively low, ranging from 1 to 2 years, underscoring the need for advanced treatment strategies [5].
Conclusion
- Primary lymphoma of the kidney is a rare tumor.
- Preoperative diagnosis remains difficult because radioclinical criteria are not specific.
- Chemotherapy represents the treatment of choice especially in high grade forms of malignancy.
References
-
Khader KEL, Sadiq A, Karmouni T, Ouali M, Hachimi M, et al. (2004) Primary renal non Hodgkin’s lymphoma. Prog Urol 14(1): 78-80
-
Lontos K, Tsagianni A, Msaouel P, Appleman LJ, Nasioudis D (2017) Primary urinary tract lymphoma: rare but Aggressive. Anticancer Res 37(12): 6989-6995.
-
Nasrollahi H, Eslahi A, Ahmed F, Geramizadeh B, Ansari M (2022) Primary diffuse large B cell lymphoma of the right kidney: a case report. Pan Afr Med J 42: 269.
-
Taneja A, Kumar V, Chandra AB (2020) Primary renal lymphoma: a population-based analysis using the SEER program (1973-2015). Eur J Haematol 104(5): 390-399.
-
Geramizadeh B, Shojazadeh A, Marzban M (2022) Primary renal non-Hodgkin’s lymphoma: a narrative review of literature. Urologia 89(2): 185-194.
-
Bokhari SRA, Inayat F, Bokhari MR, Mansoor A (2020) Primary renal lymphoma: a comprehensive review of the pathophysiology, clinical presentation, imaging features, management and prognosis. BMJ Case Rep 13(6): e235076.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report