Traumatic Renal Artery Injuries: A Comprehensive Case Study Analysis
Post-traumatic renal artery injury is a rare yet critical complication following trauma, potentially leading to severe renal damage and functional loss. We present three cases of post-traumatic renal artery injury resulting in renal ischemia due to late diagnosis. Of particular note is that the interval between the first patient and the third is only three months, occurring at a time when such lesions are rarely observed. These cases, all involving young male individuals, highlight the challenges of prompt identification and timely intervention in such injuries. Delayed diagnosis hampered attempts at surgical revascularization in all cases, and our hospital lacked resources for percutaneous revascularization procedures. Despite efforts to manage these injuries conservatively, the success rates of surgical revascularization have been limited, leading to recurrent thrombosis. This has prompted the medical community to reconsider the approach to managing these injuries, with emphasis on non-operative methods and less invasive alternatives, particularly in the presence of a functioning contralateral kidney. However, determining the optimal management strategy remains elusive due to insufficient evidence regarding the efficacy of various approaches. Urgent management of renal artery injuries aims to preserve kidney function and mitigate secondary complications, such as renovascular hypertension. Long-term follow-up revealed varying outcomes among these patients, emphasizing the complex nature of managing post-traumatic renal artery injuries.
Introduction
Post-traumatic renal artery injury is a serious complication that can lead to the loose of the renal function by nephrotoxic damage. Thus, rapid resuscitation and restoration of circulating volume are imperative for preventing ongoing renal ischemia. Injuries affecting the kidneys represent around 1% to 5% of all cases, with the majority attributed to blunt abdominal trauma, accounting for 80% to 90% of these instances [1, 2]. Young men, typically engaged in sports, motor vehicle accidents, assaults, or falls (average age of 30), show a higher prevalence of traumatic renal injuries [1, 3].
Specific data solely on post-traumatic renal artery injury might be limited, making the precise determination of its incidence challenging. It appears that this incidence varies between 0.05% and 0.08% [4, 5, 6]. Thus, the occurrence of post-traumatic renal artery injury poses a significant concern among trauma patients. Even the kidney’s recuperation post open repair ranges widely, from 40% to below 10%, and remains largely unsatisfactory [6], Swift identification and proper intervention play pivotal roles in preserving renal function and avoiding complications especially the risk of renovascular hypertension [5, 7].
We herein report three cases of renal ischemia due to post-traumatic injury to the main renal artery. Unfortunately, the diagnosis was late, at least 24 hours later. What is anecdotal, is that the interval between the first patient and the third is only three months, at a time when such lesions are rarely seen as described above.
Cases Report
Case 1
The first patient is a man of 22 years old victim of a workplace accident with the impact point at the lumbar region, resulting in polytrauma. Evacuated to our department 24 hours after the trauma, he was stable hemodynamically with normotensive values (120/65 mmHg). The physical examination revealed well scored patient, 15 on the Glascow Coma Scale (GSC), with diffuse abdominal sensitivity. The laboratory tests revealed a hemoglobin level of 12.5 g/dL, a white blood cell (WBC) count of 6300 cells/µL, a total prothrombin time (PT) of 80%, Platelet count of 314 mm3, Blood urea nitrogen of 0.45 g/L, and serum creatinine of 14.2 g/L. The abdominal contrast-non enhanced CT scan done 24 h before, revealed thrombosis in the three left renal arteries from 7 mm of their ostiums (likely occlusive dissection). This led to almost sub-total devascularization of the ipsilateral kidney (some residual upper polar parenchymal areas, approximately 5%, vascularized by small interlobar arteries Figures 1A-D with minimal and insignificant secretion and excretion (Figuress 1E & F). In addition, there was pancreatic fracture with a peripancreatic fluid infiltration and low- volume hemoperitoneum (Figures 2A & B).
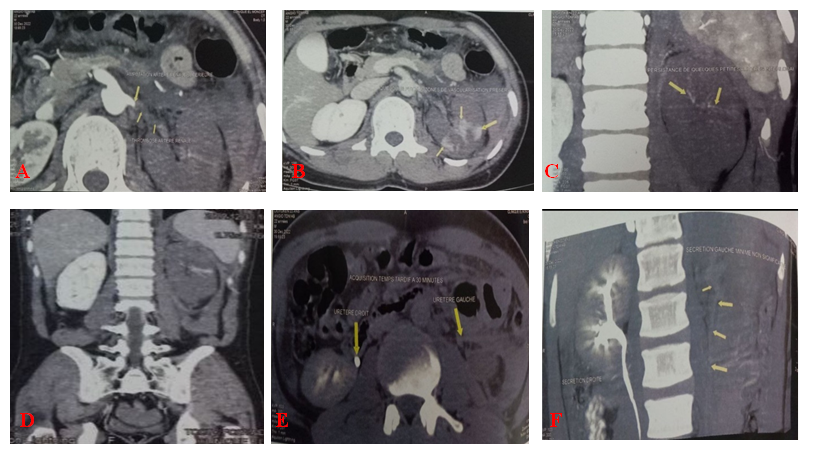
Figures 1A-D: Thrombosis of the left renal arteries with near-total devascularizaion of the kidney, E,F: Weak opacification of the left ureter.
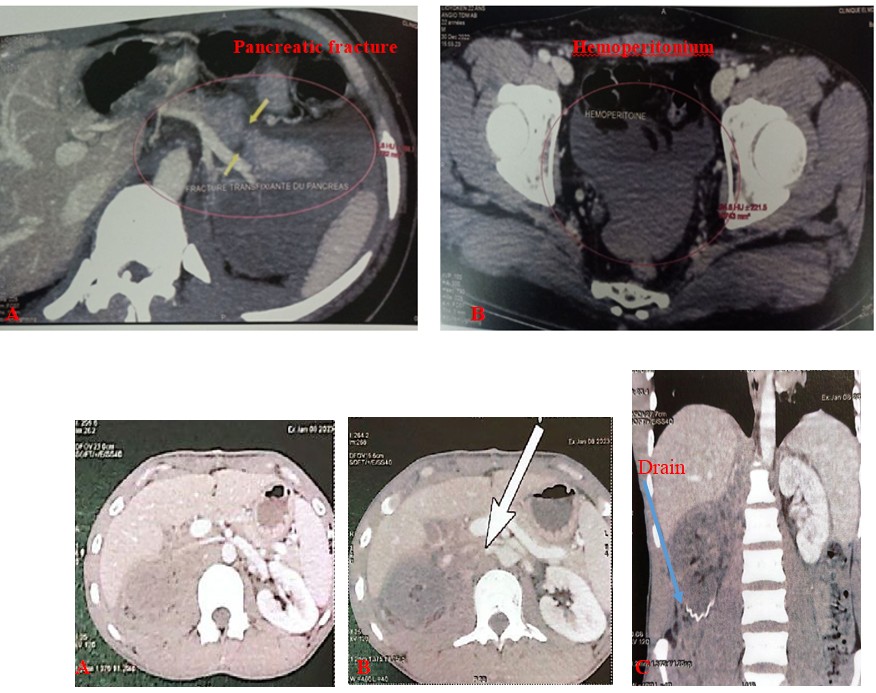
Figures 2A: pancreatic fracture, B: Hemoperitoneum.
The patient received an expectant approach for the urological lesion and subsequent drainage for the pancreatic lesion. After discharge, there was no follow-up urology consultation.
Case 2
The second patient, a 27-year-old man, was involved in a work-related accident, leading to the development of crush syndrome. He presented at the emergency department one week after the first patient. At the admission, the patient exhibited hypotension, with a blood pressure reading of 65/40 mmHg. Initial assessment showed a GCS of 15/15 with abdominal sensitivity. Laboratory tests indicated hematocrit level of 30.3%, with a hemoglobin level of 12.2 g/dL, a WBC count of 4.7×103 µL, and platelets at 362×103 mm3. His serum creatinine was 92 µmol/L. The patient received immediate and aggressive fluid resuscitation. Due to the persistent refractory shock even after resuscitation, an urgent admission to the operating room became necessary. The exploratory laparotomy revealed a bleeding vessel in the paracolic gutter that was easily manageable. Despite the presence of a retroperitoneal hematoma, the surgeon opted to explore solely the renal pedicle with a straightforward drainage, as the renal vessels appeared intact without evident injury. On the second day post-operation, an abdomen contrast-enhanced CT scan showed total ischemia in the right kidney, indicating what appears to be complete occlusion of the right renal artery (only the proximal portion is visible, while discreet opacification is observed in the renal vein, suggesting a potential vascular injury). Additionally, infiltration of perirenal fat was noted near the vascular pedicle, along the pericaval area, and adjacent to the diaphragmatic pillar (Figures 3A-C). Furthermore, the exam revealed a fracture in the left transverse processes of L1, L2, L3, and L4, along with a mid-portion fracture of the 8th right rib and a minor volume of right-sided pneumoperitoneum.
Figures 3A-C: Infiltration of perirenal fat, the vascular pedicle, the pericaval area, and adjacent to the diaphragmatic pillar.
One month later, another contrast-CT scan with angiography was performed revealing a complete occlusion of the proximal right renal artery (11 mm from the ostium), with devascularized non-functioning kidney. No retroperitoneal hematoma was observed (Figures 4A-D). He was reviewed at 3 months, 6 months, and then at 9 months with normal blood pressure.
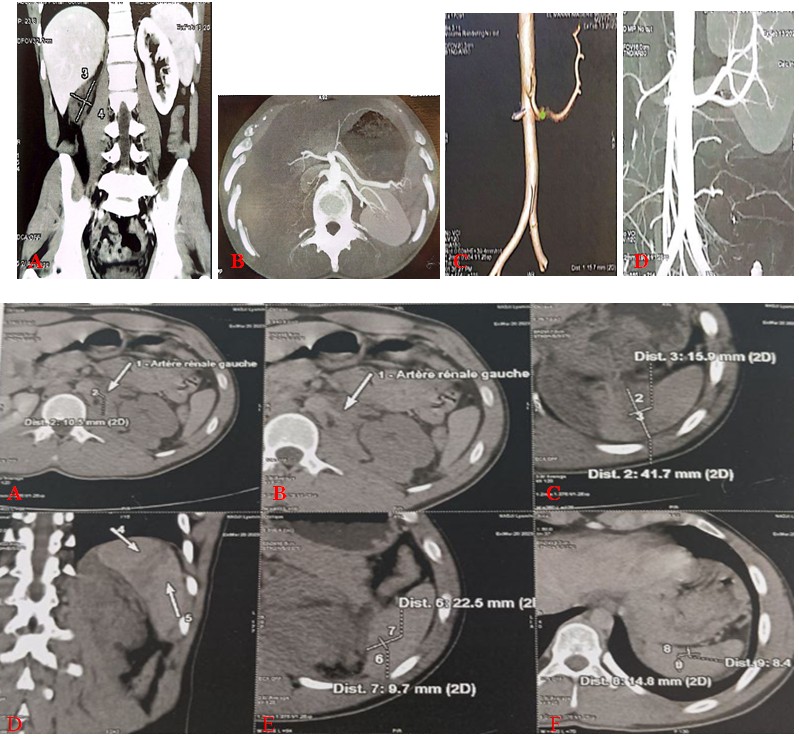
Figures 4A-D: Complete occlusion of the proximal right renal artery, with devascularized non-functioning kidney.
Case 3
The third patient, an 18-year-old male without any medical history, experienced a polytrauma following a road traffic accident and was admitted to our department 48 hours after the incident. Upon admission, the clinical examination indicated a conscious and cooperative patient with a GCS of 15/15. He presented cutaneous-mucosal pallor but maintained a preserved general condition. Hemodynamically, he presented a normal blood pressure of 120/70 mmHg, with no evident signs of hemorrhagic syndrome. The urinary catheter retrieved 900cc of slightly hematuric urine, with no further abnormalities detected during the remaining clinical examination.
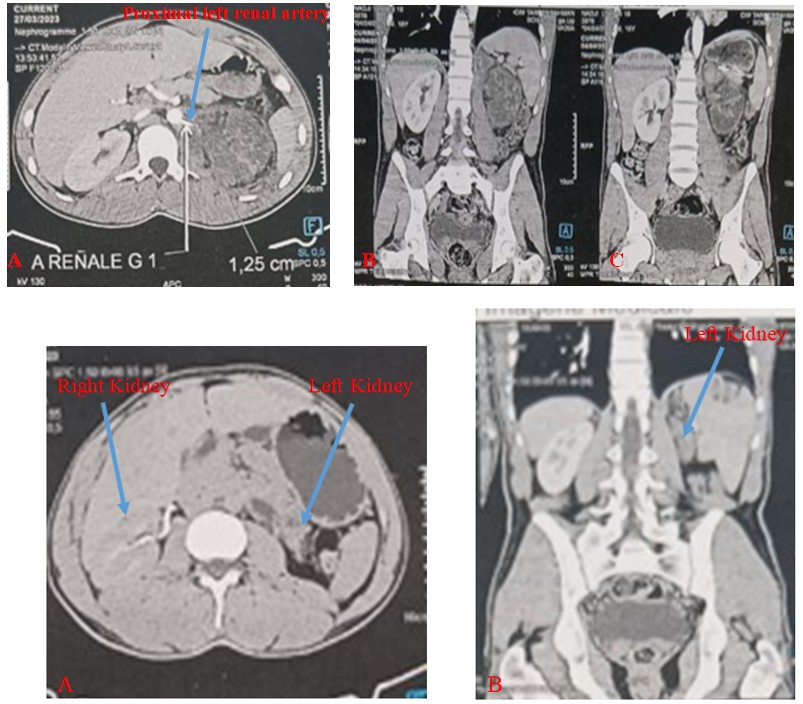
Figures 5A,B: Renal artery injury with devascularized left kidney, C-F: Multiples splenic injuries.
Laboratory investigations found a hemoglobin level of 11.5 g/dL, WBC of 5.1×103, PT of 85.67%. His blood urea nitrogen was 0.48 g/L, serum creatinine 13.2 g//L. The abdominal Contrast-non enhanced CT scan (done 24 h before) revealed an avulsion of the renal hilum (amputation of the renal artery) with a devascularized kidney without active bleeding (Figures 5A,B). Low-volume hemoperitoneum, left adrenal trauma with a non-recognizable adrenal gland submerged in a sizable hematoma extending from the adrenal space to the renal hilum, measuring 93mm*81mm*47mm. Mid-splenic fracture of 42 mm, lower pole laceration of 22 mm, and upper pole contusion focus of 15 mm with a layer of perisplenic hemoperitoneum (Figures 5C-F). Additionally, non-displaced fractures of the 9th, 10th, and 11th left ribs were identified. Given the absence of immediate indications for laparotomy, the patient, although hemodynamically stable, was admitted to the intensive care unit and received an expectant management.
A subsequent enhanced CT scan, conducted seven days later, showed essentially, no active bleeding (proximal portion of the left renal artery is visible), stabilization of splenic and adrenal gland lesions, with devascularized non- functional kidney (Figures 6A-C).
Figures 6A-C: Devascularized Kidney with artery injury.
Seven months later, another CT scan demonstrated the persistence of a non-functional small left kidney (Figures 7A & B). At the last 9-month follow-up, he maintained a normal blood pressure.
Figures 7A,B: small left non-functional kidney.
Discussion
Even with renal artery injury, the mortality rate directly linked to kidney injury alone is typically low and often stems from the extensive presence of accompanying injuries. Bergqvist, et al. [8] reported an overall mortality of 6.5%, with a specific mortality rate related to renal injury recorded at 1.7%. Other studies described a total mortality of 0.6% [8, 9].
Renal trauma is categorized into five grades, ranging from minor injuries (Grade I) to severe injuries with vascular involvement (Grade V) [9, 10, 11]. Hence, we report three cases of renal artery injuries managed in our department within a very short period (a time span of 3 months between the first and third cases), regarding a condition considered rare with an incidence approaching. Although renal trauma is relatively rare, occurring in 1.4% to 3.2% of trauma cases [12, 13] and reaching up to 5% in certain series [1, 2], arterial injuries, as a subset of these cases, account for 0.05-0.08% of all trauma incidents [4, 5].
However, recent series, as indicated by Sangthong, et al. have reported an incidence of BRAI ranging from 1% to 4% among all abdominal injuries, which relies on the criteria used for abdominal CT evaluation [5]. Notably, a surge in the number of BRAI cases became apparent starting in 2005, coinciding with the widespread adoption of the 16-slice CT scanner [14].
All three of our patients were male, with an average age of 22.3 years, consistent with the predominant trend of younger males observed in most reported series. Chow, et al. reported a male-to-female sex ratio of 3.2:1 [14], while Petrone, et al. in their recent systematic review, found 75.3% of the patients to be male, with a mean age of 33 years [9].
Even with only three patients, two of them experienced injuries to the left kidneys. The left kidney is often observed to be slightly more susceptible to injury. Literature suggests a relative injury rate of 1.4:1 to 2:1 in favor of the left side compared to the right. Potential reasons for this include the shielding of the right renal artery by the inferior vena cava and duodenum, as well as its stabilization by the liver and duodenum [15].
It’s important to note, that renovascular injuries are frequently linked with concomitant injuries to non-renal organs, as observed in our cases and documented in other similar instances [9, 13, 15]. In our cases, we did not observe significant hemorrhage, and two cases had no hematuria. This might occur when renal artery injury leads to kidney devascularization through isolated intimal damage, causing thrombosis [15].
All our patients underwent a contrast-enhanced CT scan of the abdomen, which remains the gold standard for diagnosis [1, 3, 7, 15]. However, some authors propose considering contrast-enhanced ultrasound as the initial imaging modality in clinically symptomatic patients with minor blunt trauma and a negative extended focused assessment with sonography for trauma. Contrast-enhanced ultrasound could serve as an initial screening tool before resorting to a CT scan if the results are positive [16]. For hemodynamically unstable patients admitted urgently to the operating room, an intravenous urogram (IVU) might be considered. The objective is to analyze the morphological and functional aspects of both kidneys [17]. Unfortunately, for our patient operated on in an emergency, the IVU could not be performed due to an unsuitable operating table. What prompts the preoperative assessment is that nearly a quarter of post-traumatic renal injuries go unnoticed during emergency laparotomies [18, 19]. Moreover, the surgeon resorted to a manual palpation of the renal pedicle, which appeared intact. This is especially prominent in cases of arterial thrombosis, where patients might exhibit minimal or no retroperitoneal hematoma, an intact artery, and solely relying on palpation might lead to a missed diagnosis [20, 21].
In two cases, the absence of the cortical rim nephrogram sign, typically visible in devascularized kidneys, might not manifest in the acute setting [15, 22]. In our first case, there was approximately 5% of parenchyma, vascularized by small interlobar arteries.
Though CT scans remain the standard for overall renal injuries, arteriography stands as the gold standard for detecting renal artery injuries due to its dual advantage of injury identification and potential for endovascular interventions [23].
In our three cases, unfortunately, the diagnosis was delayed. As recognized, the most crucial aspect in preserving renal function is swiftly restoring blood flow. The ideal timeframe for revascularization remains a topic of debate and lacks clarity. While some authors propose a window spanning 6-12 hours, others have reported a narrower range of 3 to 4 hours [7, 15, 24], additional authors have suggested an attempt at revascularization before 20 hours of warm ischemia have passed [7, 25].
Moreover, even preserving renal function is more likely with a limited warm ischemic time, revascularization within four hours of warm ischemia doesn’t always guarantee optimal functional recovery [7, 26, 27]. Besides the duration until restoring blood flow to the primary renal artery, additional factors may influence renal function preservation. Notably, the presence of multiple thrombi in distal renal arteries. Illustrated in our first case, the estimated incidence of renal artery thrombosis following renal trauma is approximately 2% [28]. Delayed diagnosis dissuaded surgical revascularization attempts in our three cases, despite its minimal success rates, often resulting in recurrent thrombosis [5, 29]. Consequently, many surgeons refrain from this approach, especially when a functioning kidney is present on the opposite side [13, 15]. Recent studies have highlighted the potential of percutaneous revascularization using endovascular stenting for stable patients with unilateral renal artery occlusion [15, 23]. Unfortunately, our hospital lacks interventional radiologists for these procedures.
Determining the optimal management strategy remains challenging, as evidence is insufficient to identify subsets benefiting from open revascularization, endovascular therapy, or expectant management [23]. In a level 1 trauma center, Chow, et al. employed angiography and embolization in 34.3% of cases [14], while some advocate for open surgery in urgent scenarios.
Current consensus suggests that open revascularization is not recommended if a functioning contralateral kidney exists [4, 12, 13, 14, 27]. Non-operative management remains important due to poor outcomes following urgent surgical revascularization, with an estimated preserved kidney rate of less than 20% [29]. Selective arterial embolization via angiography emerges as a less invasive alternative to laparotomy, boasting a success rate exceeding 90% [30].
Nine months post-injury during the follow-up, two patients did not require antihypertensive medication and had normal blood pressure readings. For the first patient, we did not receive any updates. Indeed, urgent management of renal artery injury is aimed at preserving kidney function and preventing renovascular hypertension, thereby reducing the likelihood of necessitating secondary nephrectomy [5, 12, 26, 29]. Haas, et al. reported Thirty-four out of 105 patients (32%) who did not undergo attempted revascularization experienced the onset of hypertension [12].
Conclusion
Post-traumatic renal artery injuries pose significant challenges in timely diagnosis and appropriate management, particularly given their rarity and potential for severe complications. The cases presented underscore the limitations in prompt identification and intervention, resulting in delayed attempts at surgical revascularization and highlighting the lack of available resources for alternative procedures in our hospital. The limited success rates of surgical revascularization and the associated risk of recurrent thrombosis have led to a reevaluation of the management approach, with a shift toward non-operative methods and less invasive techniques. However, establishing the optimal management strategy remains a challenge due to inadequate evidence on the effectiveness of different approaches. Urgent management aims to preserve renal function and prevent secondary complications, necessitating further research and standardized protocols to enhance outcomes in these cases. Long-term follow-up revealed varied outcomes, emphasizing the need for comprehensive management and continued monitoring in post-traumatic renal artery injuries.
Declarations
Acknowledgment
Not Applicable
Conflict of Interest
Not Applicable
Ethics Approval and Consent to Participate
Yes
Consent for Publication
Yes
Availability of Data and Materials
Yes
Competing Interests
No
Funding
No
Autours Contributions
NA
References
-
Ząbkowski T, Skiba R, Saracyn M, Zieliński H (2015) Analysis of Renal Trauma in Adult Patients: A 6-Year Own Experiences of Trauma Center. Urol J 12(4): 2276-2279.
-
Baghdanian AH, Baghdanian AA, Armetta A, Babayan RK, LeBedis CA, et al. (2017) Utility of MDCT findings in predicting patient management outcomes in renal trauma. Emerg Radiol 24(3): 263-272.
-
McPhee M, Arumainayagam N, Clark M, Burfitt N, DasGupta R (2015) Renal injury management in an urban trauma centre and implications for urological training. Ann R Coll Surg Engl 97(3): 194-197.
-
Bruce LM, Croce MA, Santoniello JM, Miller PR, Lyden SP, et al. (2001) Blunt renal artery injury: Incidence, diagnosis, and management. Am Surg 6: 550-554.
-
Sangthong B, Demetriades D, Martin M, Salim A, Brown C, et al. (2006) Management and hospital outcomes of blunt renal artery injuries: analysis of 517 patients from the National Trauma Data Bank. J Am Coll Surg 203(5): 612-617.
-
Owattanapanich N, Benjamin E, Lewis M, Cai J, Demetriades D (2021) Epidemiology and management of isolated blunt renal artery injuries. J Trauma Acute Care Surg 90(6): 1003-1008.
-
Kushimoto S, Shiraishi SI, Miyauchi M, Tanabe S, Fukuda R, et al. (2011) Traumatic Renal Artery Occlusion Treated with an Endovascular Stent-The Limitations of Surgical Revascularization: Report of a Case. Surg Today 41: 1020-1023.
-
Bergqvist D, Grenabo L, Hedelin H, Lindblad B, Mätzsch T (1983) Blunt renal trauma. Analysis of 417 patients. Eur Urol 9(1): 1-5.
-
Petrone P, Perez-Calvoa J, Brathwaitea CEM, Islamb S , K Josepha DA (2020) Traumatic kidney injuries: A systematic review and meta-analysis. Int J Surg 74: 13- 21.
-
Tinkoff G, Esposito TJ, Reed J, Kilgo P, Fildes J, et al. (2008) American Association for the Surgery of Trauma Organ Injury Scale I: spleen, liver, and kidney, validation based on the National Trauma Data Bank. J Am Coll Surg 207(5): 646-655.
-
Buckley JC, McAninch JW (2011) Revision of current American association for the surgery of trauma renal injury grading system. J Trauma 70(1): 35-37.
-
Haas CA, Spirnak JP (1998) Traumatic renal artery occlusion: a review of the literature. Tech Urol 4: 1-11.
-
Santucci RA, Wessells H, Bartsch G, Descotes J, Heyns CF, et al, (2004) Evaluation and management of renal injuries: consensus statement of the renal trauma subcommittee. BJU Int 93(7): 937-954.
-
Chow JD, Thompson KJ, Hartman JF, Wright ML (2009) A 10-year review of blunt renal artery injuries at an urban level I trauma centre. Injury 40: 844-850.
-
Ahmed Z, Nabir S, Ahmed MN, Al Hilli S, Ravikumar V, et al. (2016) Renal Artery Injury Secondary to Blunt Abdominal Trauma – Two Case Reports Zahoor. Pol J Radiol 81: 572-577.
-
Comune R, Grassi F, Tamburrini S, Liguori C, Tamburro F, et al. (2023) Traumatic segmental renal infarction due to renal apical artery thrombosis by minor blunt abdominal trauma: the role of CEUS. Journal of Ultrasound 26: 939-944.
-
Morey AF, Mcaninch JW,Tiller BK, Duckett CP, Carroll PR (1999) Single Shot Intraoperative Excretory Urography For The Immediate Evaluation of Renal Trauma. J Urol 161(4): 1088-1092.
-
Lock JS, Carraway RP, Laws HL (1985) Proper management of renal artery injury from blunt trauma. South Med J 78(4): 406-410.
-
Stables DP, Fouche RF, Niekerk JPDVV, Cremin BJ, Holt SA, et al. (1976) Traumatic renal artery occlusion: 21 cases. J Urol 115(3): 229-233.
-
Cass AS, Bubrick M, Luxenberg M, Gleich P, Smith C (1985) Renal pedicle injury in patients with multiple injuries. J Trauma 25(9): 892-896.
-
Bertini JE, Flechner SM, Miller P, Ben-Menachem Y, Fischer RP (1986) The Natural History of Traumatic Branch Renal Artery Injury. J Urol 135(2): 228-230.
-
Harris C, Zwirewich CV, Lyburn ID, Torreggiani WC, Marchinkow LO (2001)CT findings in blunt renal trauma. Radiographics 21(suppl 1): S201-214.
-
Beyer C, Zakaluzny S, Humphries M, Shatz D (2017) Multidisciplinary Management of Blunt Renal Artery Injury with Endovascular Therapy in the Setting of Polytrauma: A Case Report and Review of the Literature, Ann Vasc Surg 38: 318.e11-318.e16.
-
Cass AS (1989) Renovascular injury from external trauma. Urol Clin North Am 16: 213-220.
-
Frassinelli P, Pasquale MD, Reckard C, Goodreau J, Sherwin G (1997) Bilateral renal artery thrombosis secondary to blunt trauma: Case report and review of the literature. J Trauma 42: 330-332.
-
Flugsrud GB, Brekke M, Roise O (2005) Endovascular stent in the acute treatment of blunt renal arterial injury. J Trauma 59(1): 243-245.
-
Knudson MM, Harrison PB, Hoyt DB, Shatz DV, Zietlow SP, et al. (2000) Outcome after Major Renovascular Injuries: A Western Trauma Association Multicenter Report. J Trauma 49(6): 1116-1122.
-
Kang KP, Lee S, Kim W, Jin GY, Na KR, et al. (2008) Renal infarction resulting from traumatic renal artery dissection. Korean J Intern Med 23(2): 103-105.
-
Haas CA, Dinchman KH, Nasrallah PF, Spirnak JP (1998) Traumatic renal artery occlusion: A 15-year review. J Trauma 45(3): 557-561.
-
Nuss GR, Morey AF, Jenkins AC, Pruitt JH, Dugi DD, et al. (2009) Radiographic Predictors of Need for Angiographic Embolization After Traumatic Renal Injury. J Trauma 67(3): 578-582.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report