Kimura’s Disease: A Rare Disorder
Kimura's disease is a rare disorder characterised by single or multiple soft tissue masses, cervical lymphadenopathy, peripheral eosinophilia and raised serum IgE levels. Histopathologically, it consists of hyperplasia of the lymphoid tissue with well-developed lymphoid follicles, marked lymphocyte (eosinophil) infiltration, proliferation of thin-walled capillary venules, and varying degrees of fibrosis. The etiology remains unknown. Treatment usually ranges from observation & follow-up of mild & symptomatic cases to conservative surgical approach, medication & radiotherapy in symptomatic & recurrent cases.
Introduction
Kimura’s Disease is a chronic inflammatory disorder with unknown etiology and pathogenesis. It is a benign disease with an indolent course, slowly increasing over months or years. Principally, it involves lymph nodes and subcutaneous tissue of head and neck region. Thus, it is often associated with regional lymphadenopathy. The classical triad of Kimura’s disease include single or multiple painless, slowly enlarging soft tissue masses, associated lymphadenopathy and peripheral eosinophilia, raised ESR & serum IgE. Here, we report of a rare case of the disease in a young male patient. Clinical Case A 28 year old man presented to the outpatient department with a painless, gradually progressive swelling behind his left ear since 7 years. He did not give history to fever, loss of appetite or any other constitutional symptoms. Physical examination revealed a 10 cm X 8 cm smooth, non-tender left post-aural swelling. It was compressible, and had a doughy consistency. Overlying skin appeared to be involved on account of hyper pigmentation. (Figure 1) Laboratory investigations revealed haemoglobin of 14 gm%, WBC count of 8,000 (Neutrophils: 34%, Lymphocytes: 40%, Eosinophils: 26%). Total IgE levels were 1500 IU/ ml (normal values <1.5-378.0). Serum electrolytes, liver and renal function tests were within normal limits.

A contrast-enhanced CT scan was done. It was suggestive of abnormal soft tissue at the skull base on the left side, extending from post auricular region and reaching caudally into the upper cervical region. There was loss of fat planes between the lesion and parotid gland and also with the sternocleido mastoid muscle. There was no bony erosion (Figure 2).
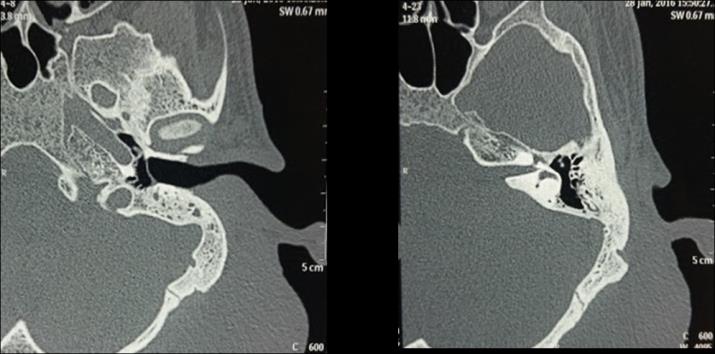
Figure 2: CT showing abnormal soft tissue at the skull base on the left side, extending from post auricular region and reaching caudally into the upper cervical region with loss of fat planes between the lesion and parotid gland and also with the sternocleidomastoid muscle. MRI was done for better soft tissue delineation. It revealed a large (9cm X 7cm X 4cm) T2 heterogeneously hyper intense lesion in the left peri-parotid region. There was loss of fat planes between the lesion and parotid gland with infiltration of the superficial lobe. There was no evidence of flow voids or calcification within the lesion. The initial fine needle aspiration cytology was reported as lymphangioma. Skin biopsy showed a dense diffuse and nodular infiltrate of lymphocytes and histiocytoid cells involving the whole of reticular dermis and extending to sub cut is with most of nodules showing formation of lymphoid follicles and few eosinophils scattered within the infiltrate. These findings were consistent with a diagnosis of Kimura’s disease. Accordingly, the patient was started on high dose corticosteroids (60 mg of oral prednisolone) for two months with gradual tapering thereafter. The response was excellent with complete disappearance of lesions (Figure 3) and normalisation of serum eosinophil and IgE levels. Now, the patient is on small dose of prednisolone 7.5 mg per day since two months and there has been no recurrence.

Discussion
Kimura’s disease (KD), also known as eosinophilic hyperplastic lymphogranuloma, commonly presents as subcutaneous swelling in the cervical region along with cervical lymphadenopathy, raised eosinophilic count and elevated serum IgE [1]. Although it was first described in China in 1937, the term “Kimura Disease” was coined by Kimura, et al. [2]. Although, the exact etiopathogenesis of KD remains largely unknown, it appears to be a systemic immunological disorder because of its association with eosinophilia and increased serum IgE levels. It may be considered a type of CD4 (+) T helper 2 (Th2) allergic reaction. Th2 cells would produce interleukins (IL) IL-4, IL-5 and IL-13, which, in turn, would act on B cells favouring the production of antigen-specific IgE. Th2 cell proliferation and the over expression of cytokines would play an essential role in the development and progression of the disease [3]. It is a benign disease which affects subcutaneous tissues, major salivary glands, lymph nodes mainly in head and neck area. Other sites such as oral cavity, groin, trunk and limbs may also be involved. The disease is supposed to be endemic in areas of China and Japan, although sporadic cases have been described elsewhere [4]. It usually presents as non-tender subcutaneous swelling in head and neck region, primarily in preauricular and submandibular area. It is associated with lymphadenopathy, peripheral eosinophilia and an elevated IgE level [5]. In our case, also the patient had elevated eosinophils and serum IgE levels. It mimics neoplastic lesions. FNAC may be inconclusive and histopathology forms the mainstay of diagnosis. In our case, though FNAC was suggestive of lymphangioma but due to presence of soft tissue lesion and loss of fluid and flow voids on both CT and MRI, further skin biopsy was performed. Skin biopsy showed a dense diffuse and nodular infiltrate of lymphocytes and histiocytoid cells involving the whole of reticular dermis and extending to sub cut is with most of nodules showing formation of lymphoid follicles and few eosinophils scattered within the infiltrate. These findings were consistent with a diagnosis of Kimura’s disease. Histological features include dense fibrosis, lymphoid infiltration with reactive follicles, and a mixed inflammatory cell infiltrate with numerous eosinophils [6], all of which can develop in subcutaneous tissue, salivary glands, and lymph nodes. The conspicuous feature of the cellular component is distinct lymphoid follicles, consisting mainly of lymphocytes. The fibrocollagenous component is formed by the infiltrate with numerous eosinophils, and eosinophilic micro abscesses are common. The vascular component consists of proliferating and swollen endothelial cells, without atypical nuclei or abundant eosinophilic cytoplasm. Salivary glands are frequently involved (they experience parenchyma atrophy and fibrosis); regional lymph nodes, usually enlarged, experience follicular hyperplasia with increases in eosinophils with or without fibrosis. Renal involvement may occur in up to 60% of patients as membranous glomerulonerphritis, minimal change glomerulonephritis, diffuse proliferative glomerulonephritis, mesangial proliferative glomerulonephritis and also nephritic syndrome (12% of cases) [5, 7]. The differential diagnosis of Kimura’s disease frequently in previous literatures are Lymphomas, salivary gland neoplasms, benign lymphoepithelial lesions (BLL / Mikulicz’s disease), Angiolymphoid hyperplasia with eosinophilia (ALHE/ Epitheloidhemangioma) and angioimmunoblastic lymphadenopathy (AIL). Constant classical features of KD include numerous lymphoid follicles, mixed inflammatory infiltrate composed mainly of eosinophils and increased amount of post capillary venules [8]. There are multiple theories of origin of the disease which include interference with immune regulation, atopic reaction to a continuous antigenic stimulus (especially Candida albicans) parasitic infection and neoplasm. The most accepted theory is that of Candida acting as a source of persistent antigenemia, although neither hyphae nor spores have been isolated [5]. Well defined treatment protocol for treatment of disease are yet to be established [2]. Treatment usually ranges from observation & follow-up of mild & symptomatic cases to conservative surgical approach, medication & radiotherapy in symptomatic & recurrent cases. According to previous literature, only surgical approach had high incidence of recurrence up to 25% [1]. Our patient had complete remission after high dose corticosteroids and is now on continuous low dose steroid to avoid recurrence. If the lesion is recurrent with systemic involvement, application of medication like corticosteroid and immunosuppressive agents have been shown to decrease size of the lesion [2]. Irradiation should be considered in patients resistant to the steroid or to prevent the patient from deleterious effect of long term use of steroid [8].
Conclusion
Kimura’s Disease, though uncommon should be considered in differential diagnosis in patients who present with head & neck mass and lymphadenopathy and investigated accordingly as this disease has good prognosis.
References
-
Yuen HW, Goh YH, Low WK, Lim-Tan SK (2005) Kimura’s disease: a diagnostic and therapeutic challenge. Singapore Med J 46(4): 179-183.
-
Kimura T, Yoshimura S, Ishikawa E (1948) On the unusual granulation combined with hyperplastic changes of lymphatic tissue. Trans Soc Pathol Jpn 37: 179-180.
-
Briggs PL (2006) Kimura disease is not angiolymphoid hyperplasia with eosinophilia: clinical and pathological correlation with literature review and definition of diagnostic criteria. Anais Brasileiros de Dermatologia 81(2): 167-173.
-
Atar S, Oberman AS, Ben-Izhak O, Flatau E (1994) Recurrent nephrotic syndrome associated with Kimuras disease in a youngnon-oriental male. Nephron 68(2): 259-261.
-
Armstrong WB, Allison G, Pena F, Kim JK (1998) Kimura's disease two case reports and a literature review. Ann Otol Rhinol Laryngol 107(12): 1066- 1071.
-
Chun SI, Ji HG (1992) Kimura’s disease and angiolymphoid hyperplasia with eosinophilia: clinical and histopathologic differences. J Am Acad Dermatol 27: 954-958.
-
Hui PK, Chan JKC, Ng CS, Kung ITM, Gwi E (1989) Lymphadenopathy of Kimura's disease Am J Surg Pathol 13(3): 177-186.
-
Jani A, Coulson M (1997) Kimura's disease A typical case of a rare disorder. Western Journal of Medicine 166(2): 142-144.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?