Safe and Optimum Steps for Total / Hemi Thyroidectomy
Thyroidectomy is always an interesting surgery for all general, ENT, endocrine and oncosurgeons. There is lot of paradigm shift in thyroid surgeries from no identification to identification and tracking for recurrent laryngeal nerve and from open thyroidectomy to video-assisted and minimal invasive thyroidectomy procedures.
Introduction
Thyroidectomy is always an interesting surgery for all general, ENT, endocrine and oncosurgeons. There is lot of paradigm shift in thyroid surgeries from no identification to identification and tracking for recurrent laryngeal nerve and from open thyroidectomy to video-assisted and minimal invasive thyroidectomy procedures. Most of surgeons in our country are more trained in open thyroidectomy and basic principal in even minimal invasive surgeries also remains same for it which we are discussing in this article for educational purpose of post graduates of all sub specialties mentioned. Previously lot of surgeries are described for thyroid lesion like hemi- thyroidectomy, subtotal,near total, Dun-hill procedure, lobectomy and total thyroidectomy. Now a day’s most of these procedures are obsolete terms only and need not to describe anywhere. Total Thyroidectomy is definitive surgery and hemi-thyroidectomy is an excisdional biopsy procedure in malignancy cases and therapeutic in some benign solitary nodules if indication provided. Rest of named surgeries is not being performed now a days in most of world.
| Steps for Hemi/Total Thyroidectomy | |||
|---|---|---|---|
| 1 | Positioning & painting draping | ||
| 2 | Incision skin crease | ||
| 3 | Sub platysmal flap | ||
| 4 | Incising investing layer of deep cervical fascia & Muscle retraction/ division Middle thyroid vein | ||
| 5 | Superior pedicle management | ||
| 6 | Recurrent laryngeal nerve and parathyroid | ||
| 7 | Glands identification | ||
| 8 | Inferior thyroid vessel management | ||
| 9 | Thyroid dissection from bed | ||
| 10 | Repeat procedure in contra lateral side | ||
| 11 | Hemostasis | ||
| 12 | Drain placement | ||
| 13 | Wound closure |
Step 1: Positioning to Draping
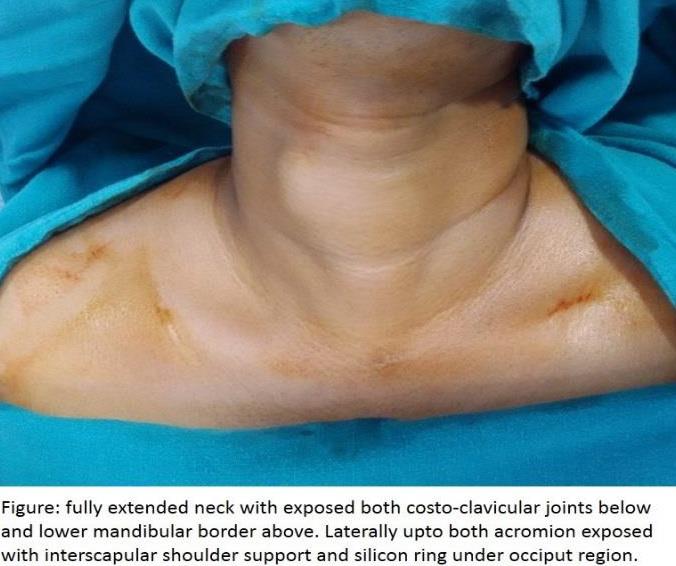
Correct optimal positioning is critical for proper exposure of thyroid bed and approach for maneuvers. After general anesthesia and endotracheal intubation, patient should be kept in supine position with full neck extension supported by sand bag underneath inter- scapular region and a silicone gel or sheath under occipital region. Neck extension makes the swelling more prominent and surgical landmarks more visible. For draping, take three sheets of cloth, across and under head region. Drop one sheet on operation table, one over the shoulders and upper most to cover head and face region upto the mandible lower border or chin. Both clavicles with both side costoclavicular joints below, mandibular lower border above and acromian process on both sides should be visible for proper exposure. Neck should be centralized. Operative table lights should be adjusted in lower part of neck.
Step 2: Proper Skin Crease Incision
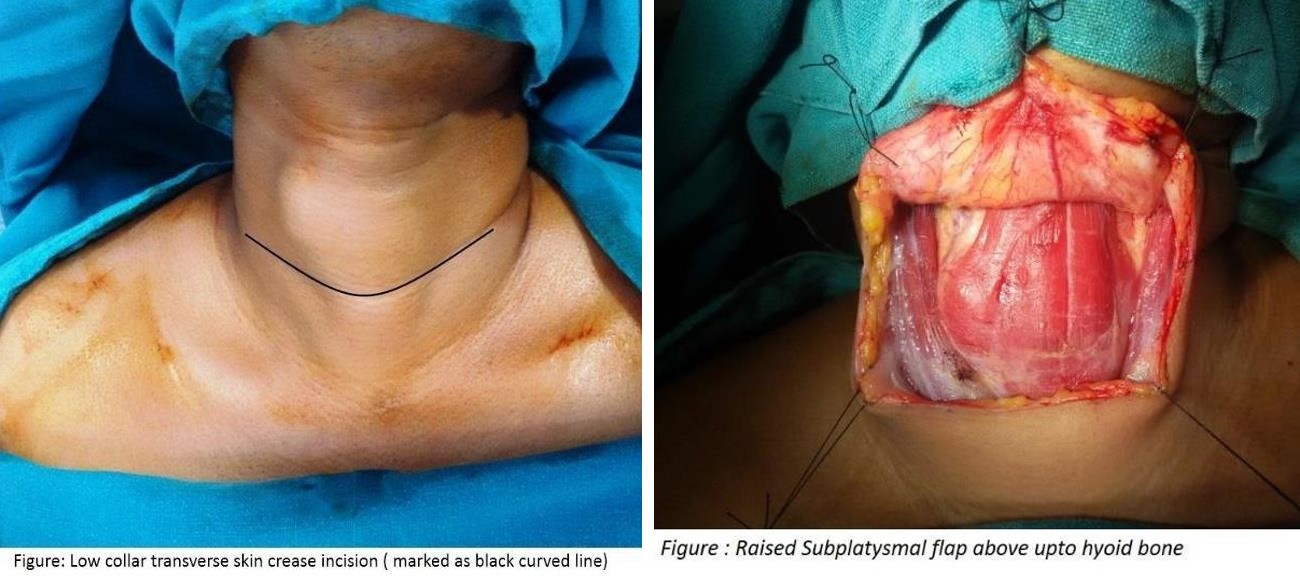
Incision in thyroid surgeries is constant if no additional neck procedure is planned. Classically described as low collar transverse skin crease incision is adequate for total thyroidectomy, while it can be limited ipsilateral if hemi- thyroidectomy planned in one side. Skin crease or Langerhans’ line incision is along the natural skin crease or fold demarcated by folds on neck flexion about 1.5- 2cms above from sternal notch or costoclavicular joints. While inextended neck, it appears as skin marks or grooves. Laterally it extends on both sides upto anterior borders of sternocleidomastoid muscle. Sometimes in huge tumors incision size may be extended more laterally. If unilateral or bilateral neck dissection is also planned, then the same incision may be extended in same side as “J”shape or “U” shape incision upto the mastoid tip. Benefit of skin crease incision is cosmetic demanding and good minimal or scars less healing. Skin incision mark can be infiltrated with local anesthetic with adrenaline before 3 minutes of incision to reduce bleeding.
NOTE: After incising skin, platysmal should be incised with electro-cautery to avoid bloody field and mid portion of platysmal is thinner than lateral.
Step 3: Raising the Sub-Platysmal flap
After making a proper skin and subcutaneous platysmal muscle transverse incision, dissection is to be done under it by raising with skin hooks, raising the flap just above the upper border of thyroid cartilage. Subplatysmal flap can be anchored to drape sheets with silk sutures for continuous exposure. Raising flap with platysmal flap additionally spare a marginal mandibular nerve injury in other neck surgeries where incision is higher up in neck. Some surgeons prefer to raise flap on lower side also upto sternal notch. But it’s not essential if thyroid nodule is not too huge to approach or retrosternal goiter. Even it avoids unnecessary dissection, inflammation and vessel injuries.
Step 4: Incising investing layer of deep cervical fascia & Muscle retraction/ division
After raising Subplatysmal flap, strap muscles can be visualized enclosed in investing layer of deep cervical fascia, continuous laterally entrapping sternocleidomastoid muscles on both sides. Investing layer of deep cervical fascia has to be incised in midline vertically with electro-cautery without cutting or incising any muscle in full length of exposure. Strap muscles can be separated from loose areolar tissue in midline and retracted laterally. Just retraction of muscles gives a bloodless field in operating area. In case of huge goiter, it’s difficult to deliver the thyroid lobe or nodule by muscle retraction. Surgeons has to divide the strap muscles in upper one third of muscle length to spare the Ansa cervicalis formed by hypoglossal nerve and cervical plexus synapses in lower part of neck. Sometimes if strap muscles are directly infiltrated or adherent to thyroid mass, then it can be partially excised to take a safe margin.
Step 5: Middle Thyroid Vein Dissection
After delivering the relevant thyroid lobe out retracting the strap muscles, lobe has to retract medially lifting lateral borders. As the lobe is levated, the adjacent strap muscles and the associated adventitial tissues are swept away from the thyroid lobe and retracted laterally and gland is dissected for middle thyroid vein, a tributary of IJV, is a fragile structure and unsupported by any artery unlike superior and inferior pedicle. Middle thyroid vein is ligated and divided in between ligating sutures. Dissection is proceed superiorly upto superior lobe.
Step 6: Superior Pedicle Management
Conventionally, superior pedicle was ligated close to gland to avoid injury to external laryngeal nerve. But now a days, superior thyroid artery and vein are ligated separately after individual identification. Landmark for superior thyroid vessel is identified by Joll’s triangle which is formed medially by central line, base of triangle by insertion of strap muscle above, and laterally by superior thyroid vessels. External laryngeal nerves passes through this triangle. Injury to this nerve is noticed only in singers usually because of change in pitch of voice. Superior thyroid artery and vein are ligated and divided in between sutures.
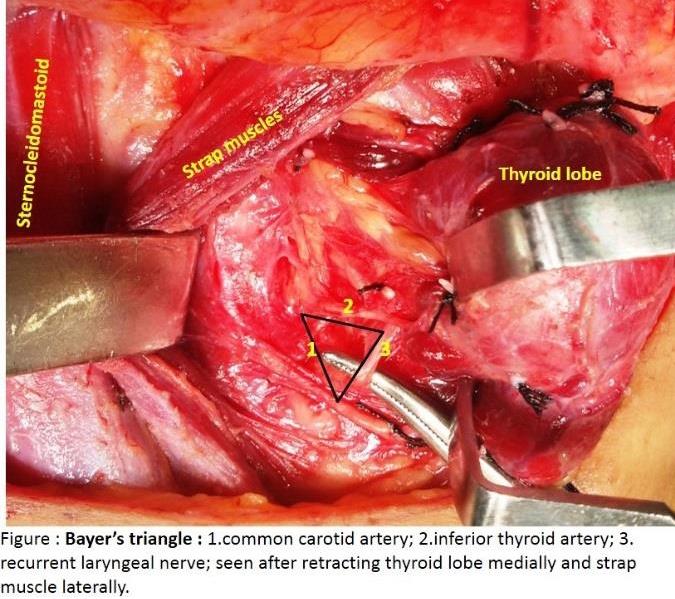
Step 7: Recurrent Laryngeal Nerve and Parathyroid Glands Identification
As the lobe is elevated, the adjacent strap muscles and the associated adventitial tissues are swept away from the thyroid lobe and retracted laterally. At this point recurrent laryngeal nerve should be identified before ligating any structure in neck. Recurrent laryngeal nerve runs parallel to trachea and turn obliquely into larynx. On medial rotation of thyroid lobes it appears oblique antero- medially in its course which can be recognized because of its neurovasorum from exit from thorax to entry into larynx in its course. Landmark to recognize RLN is Beahr’s triangle with apex pointing towards trachea. Laterally base is formed by common carotid artery, superiorly by inferior thyroid artery and inferiorly by RLN. Another reliable way to recognize RLN is crico- thyroid joint at lower border of CTmuscle. Maceration of cricothyroid muscle may also lead to voice dysfunctioning or dislocate cricoarytenoid joint. During dissection, fascial covering over the nerve should be left to avoid direct contact of foreign body or its toxic metabolites. Both superior and inferior Parathyroid gland has to be identified and preserved from being avulsed or devascularised during dissection. Identification of parathyroid is difficult due to variability in location of these gland especially inferior parathyroid glands (PGs) due to its embryological decent with thymus. PGs has so high proportion of location variability that many times it doesn’t get identified. These may have ectopic like intrathyroidal, parapharyngeal, or superior mediastinal locations. It has to be recognized in different ways as its color is light brown to tan which relates to their fat content, vascularity, and percentage of oxyphill cells within the glands. Color may confuse with fat lobules but a distinct hilar vessel can be identified if not obscured by surrounding fat tissue.
Step 8: Inferior Thyroid Vessels Management
After identification of RLN & inferior parathyroid gland, inferior thyroid artery is identified in relation to RLN, but should be preserved. ITA should be ligated & divided near to capsule of gland. This reduces devascularisation of parathyroid glands. Capsular vessels ligation during whole thyroid dissection also preserves ITA.
Step 9: Thyroid Dissection from Bed
After dissecting both poles, thyroid gland has to be lifted from tracheal bed. The holdup tends to be a condensation of fascia called berry’s ligament between anteromedial trachea and posterio-lateral surface of trachea. Minor vessels over the trachea can be managed with bipolar cautery easily, but if left unmanaged is major cause of post-operative reactionary hemorrhage.
Step 10
Repeat the same procedure on other side as well if total or near total thyroidectomy is warranted.
Step 11
Hemostasis is extremely important as post-operative
bleeding may cause breathing difficulty or chocking sensation in wards. Vascular pedicels on both side additional to tracheal oozing is common sites for hemorrhage in post-operative period.
Step 12
Drain placement: Although perfect hemostasis obviates the need for drain placement, but routinely surgeons prefer to have a 14 F’ vacuum drain placement – a. -as close as possible to incision. b. -as lateral as possible to the incision to hide its scar in collar. c. -should be placed under muscle layer before closure. Any lymph nodes neck dissection make the drain placement mandatory for seroma drainage.
Step 13: Wound closure
People are very apprehensive for neck scar & appearance; hence fineness with wound closure is very important. Muscle layer should be closed with 2-4 loose sutures in midline and cervical fascia in midline with 3-0’ vicryl sutures. Skin flap should be closed with platysma without having a button hole. Leaving platysma unsutured in skin can produce unsightly & cosmetically unappealing bulge in neck. Monocryl 4-0’ suture is adequate for subcuticular skin closure. Check the vocal cord mobility during anesthetic recovery in operation room. Thanks!!!
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?