Road Map to the Sphenoid Sinus in Trans-Nasal Endoscopic Pituitary Surgery
Endoscopic surgical techniques have been applied to the treatment of cranial base pathology, most commonly cerebrospinal fluid leaks and pituitary tumors [1].
Abdelrahman Younes1*, Waleed Rajab2, Amr AElsamman1 and HN
Lasheen1
Introduction
Endoscopic surgical techniques have been applied to the treatment of cranial base pathology, most commonly cerebrospinal fluid leaks and pituitary tumors [1]. Endoscopically “assisted” transsphenoidal microsurgery has since been reported by various authors, stressing the advantages of visualization around corners, particularly for tumors that extend beyond the sella. The endoscope, however, frequently restricts the working space and maneuverability of the instruments within the speculum when the microscope is the primary means of visualization [2, 3, 4, 5, 6, 7]. This limitation has led to a fully endoscopic, nonspeculum endonasal approach to the ventral cranial base [8]. An endoscopic transnasal sphenoidotomy approach with or without a septal dissection for resection of pituitary adenomas and other sellar lesions became available. However, an endoscopic transnasal sphenoidotomy approach without a septal dissection provided excellent exposure of the sella and adequate working space. The technique produces less postoperative pain and shortens hospital stay [9]. The sphenoidotomy approach eliminates the problems of lip numbness, septal perforations, and oronasal fistulas. The endoscopic sphenoidotomy approach has become the preferred approach to sellar lesions [10]. The ultimate target of the surgery is the sphenoid sinus; therefore the goal of the intranasal portion of the procedure is to create a passage to the sinus that is wide enough to accommodate the endoscope and the accompanying instruments. This study demonstrates a road map for approaching the sellar lesions. It presents the best surgical approach to achieve this goal of wide and safe exposure in different situations of nasal, sphenoid, and sellar pathologies.
Perspective Article
Materials and Methods
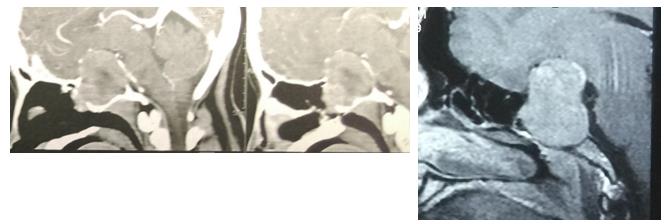
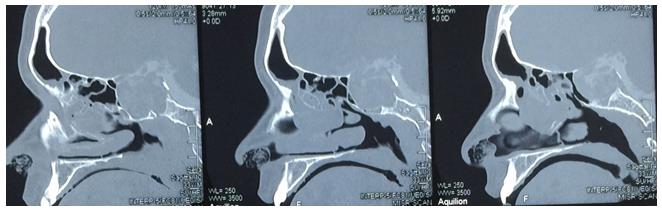
This prospective study was conducted from November 2012 to March 2016. One hundred forty-nine patients submitted underwent endonasal endoscopic removal of pituitary adenomas. There were 57 male (38.25%) and 92 female (61.74%) subjects. The male-to-female ratio was 0.62 to 1. The age range was 18 to 62 years (average age, 43 years). Besides a detailed history (headache, amenorrhea, galactorrhoea, visual symptoms, decreased vision, blurring of vision, double vision, total blindness), general physical central nervous system ophthalmologic examination, and complete ear, nose, and throat examinations were done for every patient. Pre-operative nasal endoscopy as done to evaluate the sinonasal anatomy and rule out any concurrent infectious processes that may mandate a delay in surgery. Endocrinal status was assessed (luteinizing hormone, follicle-stimulating hormone, triiodothyronine, thyroxine, thyroid-stimulating hormone, prolactin, growth hormone, and cortisol) and medical fitness for surgery was ascertained. Preoperative magnetic resonance imaging, and computerized tomography (CT) scans were obtained for all patients. The exquisite definition of the bony boundaries of the sinus, provided by thin-sliced axial and coronal scans, was essential to assess the symmetry and aeration of the sphenoid sinus and to decipher the relationship of the sphenoid sinus septum to the sella turcica floor and carotid canals. Surgery was indicated whenever there was evidence of gland enlargement, especially when growth was accompanied by compression of the optic chiasma, cavernous sinus invasion, or development of pituitary hormonal imbalances.
Surgical Technique
The operation took place with the patient supine. The head of the bed was elevated and the patient’s neck was slightly extended and rotated toward the nostril to be used for the procedure. Depending on the pre-operative assessment of the patient's nasal passageway, a 4-mm endoscope was used. The video monitor was positioned behind the patient’s shoulder directly opposite the surgeon’s line of vision. A0°_ endoscope was used to guide the intranasal dissection and initial tumor resection. In cases with the favorable parameters for the nasal cavity, sphenoid sinus, and sellar lesion, the standard endonasal endoscopic trans-sphenoid technique was applied. These favorable parameters are as follows:
- Good sphenoid sinus pneumatization
- No lateral extension of the sellar lesion
- No marked extension of the sellar pathology inside the sphenoid sinus cavity
- Pituitary microadenoma
- No concha bullosa of the middle turbinate
- Easy lateralization of the middle turbinate
- No intranasal polypi Lateralization of the middle turbinate for identification of the superior turbinate to localize the natural sphenoid ostium was the first step.
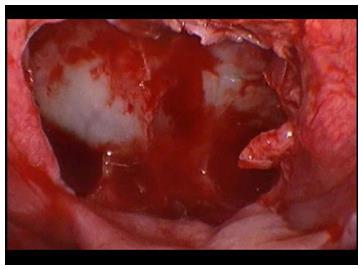
The sphenoid ostium then was enlarged using Kerrison forceps, taking care of the septal branch of the sphenopalatine artery by dissecting the mucosal flap inferior to the sphenoid ostium and removing the bone beneath. A posterior septectomy was then performed, including removing the sphenoidal keel using a cutting burr. The inter-sphenoidal septation was removed using a diamond burr, exposing the sella between the two carotids and the optico-carotid recess. After removal of the pituitary adenoma by the neurosurgeon, different reconstructive techniques were used to ensure adequate cerebrospinal fluid (CSF) seal if necessary. Medialization of both middle turbinates was done. This was the standard technique performed in this study (94 cases). However, not all cases fulfilled the previous parameters, so certain modifications of the standard technique were applied accordingly. In cases presented with concha bullosa (6 cases), resection of the medial portion of the pneumatized middle turbinates was done, followed by the same steps used in the standard technique. In cases with difficult lateralization of the middle turbinates, uncinectomy with anterior and posterior ethmoidectomy was done to allow lateralization of the middle turbinates (4 cases).
In the case of macroadenomas with protrusion of the sellar pathology inside the sphenoid sinus with near total obliteration of the sinus and/or lateral tumor extension to the cavernous sinus, room for free instrumentation and good tumor exposure was created. This was named “cavity and a half.”Good anterior and posterior ethmoidectomy were performed on one side with exposure of the lamina papyracea from the uncinate attachment anteriorly to the face of the sphenoid posterior. The third part of the middle turbinate on this side was then removed, making it flail, followed by cutting the lower two thirds of the middle turbinate, leaving the upper part to preserve the olfaction. On the other side of the nose, lateralization of the middle turbinate followed by posterior septectomy connecting two sides was done. This technique allowed better visualizations, especially for lateral extension (42 cases). In cases presented with intranasal polypi not responding to medical treatment, endoscopic polypectomy with anterior and posterior ethmoidectomy and preservation of both middle turbinates before opening the sphenoid was done (3 cases).
Results
One hundred twenty-one patients presented without previous surgical management, whereas28 cases were operated on as revision hypophysectomy. Analysis of the pre-operative CT and MRI findings of these cases revealed 4 cases with conchal pneumatization of the sphenoid sinus, 12 cases with pre-sellar, 8 with post-sellar, and the remainder with sellar pneumatization. Concha bullosa of the middle turbinate was reported in 6 cases, and intranasal polypi were noted in 3 cases (1with Cushing’s disease and 2with acromegaly). The standard technique for removal of the pituitary adenoma was used in 98 cases. In 6 cases, removal of the medial portion of the concha bullosa was done before performing the standard technique. Anterior and posterior ethmoidectomy was done before lateralization of the middle turbinate in 4 cases. The cavity and a half technique were followed in 42 cases. Complications after operations in this study were as follows:
- Postoperative recurrence of the sellar lesion in 2 cases.
- Post-operative CSF leak in 1patient.
- Post-operative hemorrhage in 0 cases.
- Post-operative permanent anosmia in 3 cases.
- Post-operative permanent diabetes insipidus in 1case.
- Post-operative meningitis in 0 cases.
Intraoperative CSF leak was noticed in 78 cases; in these cases the dural tear was sealed after tumor removal using a small plug of fat harvested from the abdomen in all cases. Reinforcement using a vascularized middle turbinate flap as a second layer was necessary in 12 cases, whereas one case with a high expectation of post- operative CSF leakage due to planum injury reconstruction was done using a Hadad flap (vascularized nasoseptal flap).In the rest of the cases, only a small plug of gel foam and a sheet of Surgical® were used.
Discussion
The endoscopic transnasal approach offers less invasive access to the pituitary gland and surrounding areas in addition to providing better intraoperative imaging of the region [11]. A great step related to the development of endoscopic neurosurgery was the teamwork with otorhinolaryngologists in skull base approaches. In general, pituitary adenomas are diagnosed more frequently in women than in men, probably because of the association of these tumors with menstrual irregularities. The incidence of pituitary adenoma increases with age, peaking between the third and sixth decades. Pituitary adenoma can be divided into functioning and nonfunctioning tumors, or according to size, namely, microadenomas or macroadenomas. Functioning pituitary adenomas can be clinically classified by means of the hormones they secrete. These tumors become symptomatic because they secrete hormones such as growth hormone, adrenocorticotropic hormone, and prolactin. Use of the endoscope for pituitary tumor resection represents a significant advancement in pituitary surgery. The visualization advantage of an endoscope, especially the 30° endoscope, over an operating microscope was obvious in the suprasellar region; it eliminated the need to blindly curette blindly for a suprasellar tumor. The wide-angled panoramic view is useful for pituitary tumor surgery because it allows excellent anatomic visualization at the posterior wall of the sphenoidal sinus; angled-lens views, such as with 30°-, 45°-, and 70°- endoscopes, allow direct visualization at the suprasellar region or various anatomic corners. To achieve safe surgery and accepted outcomes during an endonasal endoscopic approach to the pituitary gland, a panoramic view and free handling of the instruments are mandatory. Dimensions of the sphenoid sinus, nasal cavities, and sella are of paramount importance in pituitary surgery. This study demonstrated a road map to the sphenoid sinus in endonasal endoscopic management of pituitary adenomas with the aim of achieving the best exposure for free handling of the instruments and panoramic views of the sella for different nasal cavity conditions, sphenoid sinus pneumatization types, and degrees of sellar protrusion inside the sphenoid sinus. In light of the experience gained after 149 endonasal endoscopic hypophysectomies, this study suggests the following recommendations: a. Keep the integrity of the middle turbinates if the sphenoid sinus and the sellar lesion allow good exposure and free instrumentation. b. In the case of concha bullosa, remove the medial half of the bulbous anterior end of the middle turbinate. c. If lateralization of the middle turbinate is difficult or insufficient for good exposure of the sphenoid sinus, do anterior and posterior ethmoidectomies. d. If the space inside the sphenoid sinus is insufficient for free instrumentation (conchal or pre-sellar pneumatization), the cavity and a half technique is suitable. e. In cases of macroadenomas of the pituitary gland with considerable protrusion inside the sphenoid sinus cavity, the cavity and a half technique is the procedure of choice. f. If the nasal cavity is narrowed by polyps, do a polypectomy together with anterior and posterior ethmoidectomies before dealing with the sphenoid sinus.
Conclusion
The endonasal endoscopic approach is the procedure of choice for the management of pituitary adenomas. To achieve safe surgery with a good outcome, a panoramic view and free instrumentation of the lesion is mandatory. This study presents a road map for management of these lesions for different situations of the nasal cavity, sphenoid sinus, and sellar lesion. There is no standard technique to reach the sphenoid sinus and expose the sella.
| Total number of cases | 149 | ||||
|---|---|---|---|---|---|
| Standard transnasal transsphenoid with modifications | 94 | ||||
| Concha bullosa | 6 | ||||
| Anterior and posterior ethmoidectomy | 4 | ||||
| Polypectomy (endoscopic sinus surgery) | 3 | ||||
| Cavity & a half (resection of the middle turbinate at one side) | 42 |
Table 1: Shows the different approaches and modifications to the sphenoid sinus.
References
-
Carrau RL, Kassam AB, Snyderman CH (2001) Pituitary surgery. OtoLaryngol Clin North Am 34: 1143-1155.
-
Dusick JR, Esposito F, Kelly DF, Cohan P, De Salles A, et al. (2005) The extended direct endonasal transsphenoidal approach for nonadenomatoussuprasellar tumors. J Neurosurgery 102(5): 832-841.
-
Frank G, Pasquini E, Doglietto F, Mazzatenta D, Sciarretta V, et al. (2006) The endoscopic extended transsphenoidal approach for craniopharyngiomas. Neurosurgery 59:ONS75-83.
-
Frank G, Pasquini E, Mazzatenta D (2001) Extended transsphenoidal approach. J Neurosurgery 95(5): 917-918.
-
Couldwell WT, Weiss MH, Rabb C, Liu JK, Apfelbaum RI, et al. (2004) Variations on the standard transsphenoidal approach to the sellar region, with emphasis on the extended approaches and parasellar approaches: Surgical experience in 105 cases. Neurosurgery 55(3): 539-547.
-
Daniel MP, Amin BK, Carl S, Ricardo LC, Arlan H, et al. (2007) Endoscopic Cranial Base Surgery: Ready for Prime Time? Clinical Neurosurgery 54: 48-57.
-
Lund VJ (1997) Extended applications of endoscopic sinus surgery the territorial imperative. J Laryngol Otol 111(4): 313-315.
-
Heilman CB, Shucart WA, Rebeiz EE (1997) Endoscopic sphenoidotomy approach to the sella. Neurosurgery 41(3): 602-607.
-
R Viswakarma, N Singh, R Ghosh (2006) Endoscopic Hypophysectomy. Indian J Otolaryngol Head Neck Surg 58(2): 162-164.
-
Ali NK, Ian T, Velauthan R, Alberto A, Anita J, et al. (2005) Pituitary adenoma. Overview, imaging, follow up and multimedia. E-medicine.
-
Satya PD, Vishal RM (2014) Endoscopic Endonasal Transsphenoidal Hypophysectomy: Two Hand Versus Four Hand Technique: Our Experience. Indian J Otolaryngol Head Neck Surg 66(3): 287-290.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?