Correlation between Ultrasound Aspects, Per-Operative Macroscopic and Histopathological Aspects of Thyroid Nodules
Objective: The aim of this study is to assess the correlation between ultrasound aspect per-operative macroscopic and histopathological aspects of thyroid nodules in Abidjan. Patients and methods: This is a retrospective, prospective study; it is an analytical and a descriptive type one. It has been carried out over a period of 5 years and 5 months on 61 patients who has undergone surgery for a thyroid nodular pathology in the ORL departments of the University Hospitals of Abidjan and extended to a specialized Polyclinic of the city. Results: The frequency of the thyroid nodular surgery was 64.4%. The study involved 54 women (88.5%) and 7 men (11.5%) and the average age was 43.77 years old ± 14. The correlation between ultrasound and histopathological aspects was insignificant; the sensitivity was 83% and the specificity, 67%. The correlation between per-operative macroscopic aspects and the histopathological results were insignificant. The per-operative macroscopy sensitivity was 17%, the per-operative macroscopy specificity (70%) (insignificant). Conclusion: The pre-operative ultrasound and per-operative macroscopic aspects of thyroid nodules do not always reflect the post-operative histopathological results. This enhances the interest of a candid and continuous co-operation among ORL surgeons, endocrinologists, radiologists and pathologists.
Introduction
The formation of thyroid nodules is malignant in less than 5% of the cases. Clinical examination permits to suspect advanced cancers, but early diagnosis, at the nodular stage, is almost impossible apart from the histological analysis; what justifies that they should therefore be subjected to a surgery procedure [1]. So, this raises the whole problem of diagnosis, case management and monitoring of these thyroid nodules [2]. Are ultrasound and or per-operative macroscopic aspect sufficient for the surgeon to maintain the histological nature of a thyroid nodule? We have carried out this work in order to assess the correlation between the informative and guide value of ultrasound scan and per-operative macroscopy.
Objectives of the study
Assess the correlation between the per-operative ultrasound aspects of thyroid nodules and the postoperative histopathological results; correlate the per- operative macroscopic aspects and the postoperative histopathological results of thyroid nodules.
Patients and Methods
Methods
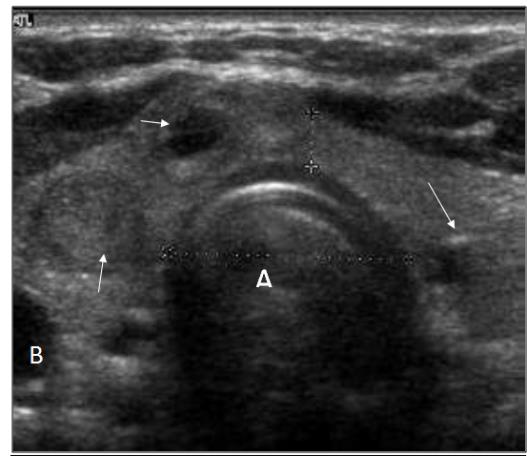
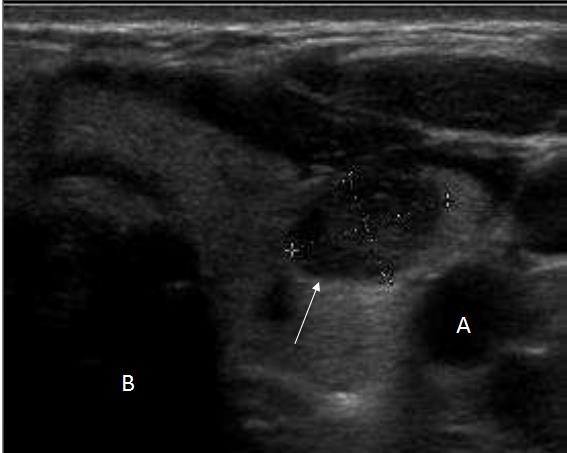
We have carried out a retrospective, prospective study; an analytical and a descriptive type study in the ORL and cervico facial surgery departments of the University Hospital of Abidjan and extended to a clinic over a period of 5 years and 5 months. The Data have been collected through: hospitalization registers of various hospital centers; patients’ medical records including: ultrasound results or descriptions of thyroid nodules surgical reports, especially operative macroscopic description; histopathological results of surgical specimens. Patients included in this study were those who presented one or more thyroid nodules with a medical record including: a case history with the results of O.R.L examination, paraclinical check-up in particular ultrasound description; a surgical report with operating macroscopic description; histopathological results. Patients who were left out from the study did not present simultaneously thyroid nodules on the ultrasound scan, in the operative procedure and in the histopathological analysis. According to the different per-operative macroscopic, ultrasound aspects, we have considered as: a. Non-malignant lesions, the presence of at least three elements in favor of the non-malignant character. b. On the ultrasound scan( liquid thyroid nodules, sharp borders, absence of latero-cervical adenopathy); in per-operative (soft consistency, sharp limits, absence of latero-cervical adenopathy) c. Malignant lesions, the presence of at least three elements which are suspected of malignancy: on the ultrasound scan (microcalcifications, size of thyroid nodules higher than 2 cm, solid character, latero- cervical adenopathy); In Per- operative: indurate nodules, invasion of neighboring tissues, latero- cervical adenopathy; Multinodular goiter (from two thyroid nodules) The ultrasound description was made according to the pictures obtained (Figure 1&2) and the morphological criteria of malignancy and benignancy (Table 1 & 2).
- Solid and hypoechogen character of the nodule
- Fuzzy, scalloped or spiculated borders
- Quadrangular
- Capsular break
- Invasion of adjoining structures
- Anteroposterior diameter (AP)> transverse diameter (T)
- Microcalcifications
- Discontinuous peripheral macrocalcifications
- Type IV Vascularization (predominant or exclusive intra-nodular hypervascularization)
- Vascular resistance index (RI)> 0.8
- High index hardness in elastography
- Adenopathy (ies) in drainage areas
Table 1: Ultrasound aspects that leads to suspect the
- Liquid Nodules
- Microcystic or hyperechogen or solid character
- Complete fine peripheral halo
- Complete peripheral calcification
- Peripheral vascularization
- Absence of adenopathy
- Absence of rigidity gradient with the surrounding tissue
Table 2: Ultrasound aspects in favor of benignancy of
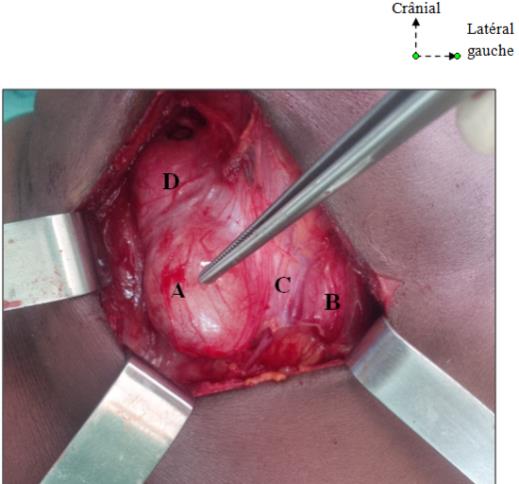
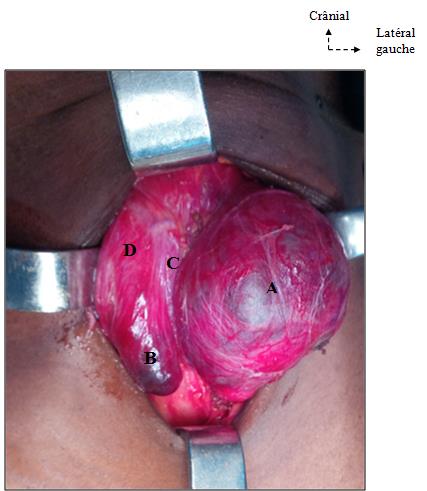
Figure 4: Per-operative aspect of a nodulo-multicystic goiter. A: Numerous cysts; B: Voluminous left nodule; C: Isthmus held by goiter; D: Right lobe (Picture: ORL department of Cocody) Gentle palpation has allowed us to specify consistency, number and borders of thyroid nodule(s) compared to adjacent tissue. Ablation of the mass has allowed us to estimate the size (measurements) with a sterile tape measure. We have noted vertical and horizontal diameters of the thyroid nodule(s) in all the cases. The tape measure has been placed over the right and left cranial pole of each thyroid lobe (Figure5 & 6).
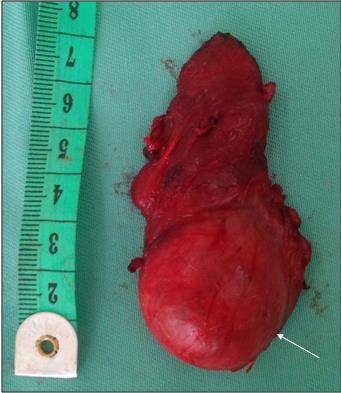
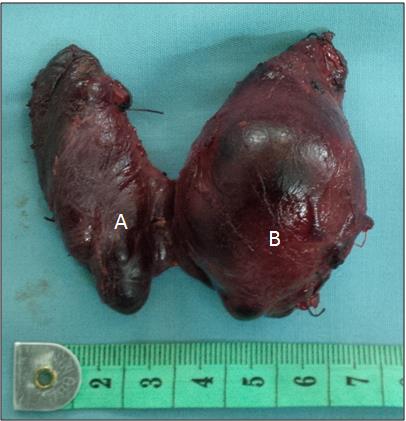
Figure 6: Surgical specimen after total thyroidectomy demonstrating a nodulo-multicystic goiter. A: Numerous cysts of the right lobe; B: Voluminous left nodule; C: Isthmus held by the goiter (Picture: ORL department of Cocody) The operative treatment taking into account the different operative macroscopic criteria suspected of malignancy or benignancy (Table 3 & 4), has consisted in either a: lobo-isthmectomy, lobectomy, subtotal or partial thyroidectomy or a total thyroidectomy. Total thyroidectomy with radical and/ or functional lymph node curettage has been completed before a thyroid cervical swelling associated with latero-cervical adenopathies and aspiration cytology malignancy signs.
- Brown or pale coloring
- Invaded adjacent tissues with hemorrhagic and necrosis foci
- Solid, firm, Indurate nodule
- Erratic thick Capsule surrounding a fleshy nodule
- Cervical adenopathy
Table 3: Operating macroscopic signs of thyroid nodules
- Homogeneous parenchyma
- Shiny, colloid aspect
- Red or dark coloring
- Normal adjacent tissue
- Thick and normal Capsule
- Renitent, soft, fleshy
Table 4: Operating macroscopic signs of thyroid nodules
Patients
During the study period, 132 patients were operated for thyroid nodular pathology. The above-mentioned inclusion criteria enabled us to maintain 61 cases.
Results
Epidemiological patterns
Frequency: Over 205 patients who have undergone surgery for a thyroid tumorous pathology, 132 have had surgery for thyroid nodular pathology that is to say a frequency of 64.4%. Age and sex: The study involved 54 women (88.5%) and 7 men (11.5%). The average age was 43.77 years old ±14 with extremes from 19 and 71 years old. The sex ratio was 0.13. X² = 46.2; P <0.05; degree of freedom (dof): 35 The distribution of the thyroid nodules according to the age has been presented in Figure 9.
Discussion
Epidemiological patterns
The frequency of thyroid nodular pathology of 64.4% of our series is similar to Koussema A series [3] who has found a frequency of 56.07%; and to that of [4] who has met a prevalence of thyroid nodules of 50% or even 67% by ultrasound detection. Female dominance, reported in the literature [3, 4, 5, 6, 7, 8] has been observed in our study. Pregnancy, iodine deficiency, cervical irradiation, menstruation seem to be predisposing causes [9]. The average age in our study was 43.77 years old. This young adult age has been found by N'gouan, et al. [5], Tanon- Anoh, et al. [6]. Other African authors [10, 11, 12] have also reported an average age of 40 years old. On the other hand, in Europe [13], the average age of functional disorders of the thyroid is 75.5 years old. This age difference in the appearance of thyroid pathologies is probably due to a deficiency-related etiology in Africa and to senile hypothyroid in Europe [12]. Furthermore, our study notes that the distribution of gender-related thyroid nodules seems to be influenced by age. This has been reported by De Luca [14] in Italy. He has noted that among adults, women have experienced more thyroid nodular pathology than men (sex ratio 4 women / 1 man), among below 15- year- old children the ratio girls / boys is 1.5 girl /1 boy, and among patients of 15-20 years old, the ratio women and men is 3 women / 1 man.
Diagnostic aspects
Correlation between ultrasound aspects and histopathological aspects of thyroid nodules: Ultrasound scan, dependent operator examination, permits to set malignancy or benignancy criteria, directing in this way, towards thyroid surgery. Histopathology, besides its diagnostic interest, is a deciding examination in the management of thyroid nodules. Despite the absence of link between ultrasound scan and histopathology in our work, ultrasound scan was a specific (67%) and sensitive (83%) examination. Zahiri [15] has found in his study 12.5% of calcification in thyroid ultrasound without any evidence of malignancy during the anatomo-pathological examination. Correlation between histopathological results and per-operative macroscopic aspects of thyroid nodules: We have not established a link between histopathological results and per-operative macroscopic aspects of the thyroid nodules. The per-operative macroscopic aspects were less sensitive (17%) but more specific (70%). Zahiri [15] has not drawn a parallel between the clinic, the imaging data and the per-operative macroscopic findings. This observation seems to attest the lack of link between the per-operative macroscopic aspects and the histopathological results of thyroid nodules. Correlation between per-operative macroscopic ultrasound aspects and histopathological results of thyroid nodules: The diagnosis of malignant or benign thyroid nodule remains a topic of current interest [16]. We have not found any relationship between the different per-operative macroscopic, ultrasound and histopathological aspects of the thyroid nodules. Moulin [16] has reported in his study that neither biology (except calciton in for the diagnosis of medullary cancers) nor imaging can allow, in most cases, to distending benign thyroid nodules of thyroid cancers. The diagnostic uncertainty of thyroid nodular tumors and the lack of management directives based on evidence have led to a vast number of contradictory recommendations. These contradictions have also been highlighted by several authors [17, 18]. These ones could be explained by the fact that most of the studies were small size, and all, have limited their analysis to patients who have undergone aspiration cytology [18]. Currently, aspiration cytology is the most efficient screening procedure for it is rapid, accessible to the greatest number of people, not very invasive, inexpensive, and reproducible, and has the best sensitivity and specificity [1, 19, 20, 21]. However, its limitations (a sampling that is not very cellular or a cell- free sampling, problems to differentiate between adenoma and carcinoma) can lead to Immunocyto chemistry which is an examination, although it is expensive and not available in Côte d'Ivoire, could reduce the frequency of total thyroidectomy and improve case management.
Conclusion
The sensitivity of the per-operative macroscopic is low and its specificity is not very high. There is no link between per-operative macroscopic aspects and histopathological results of thyroid nodules. Ultrasound scan remains a sensitive and specific examination despite the absence of link between ultrasound scan and histopathology. Per-operative macroscopic, ultrasound aspects of thyroid nodules do not always reflect histopathological results. Nevertheless, ultrasound scan always plays an important part in the management of thyroid nodules. Therefore, a candid and continuous co- operation among ORL surgeons, endocrinologists, radiologists and pathologists, is profitable. This co- operation requires more rigour in prescribing request for medical examination; in writing operative procedures, in carrying out an ultrasound scan; in the pathological analysis of surgical specimens and this, in order to improve case management.
References
-
Martins LB, Betea D, Thiry A, Petrossians P, Beckers A (2006) Nodules de la thyroïde. Rev Med Liege 61(5- 6): 309-316.
-
Trotoux J, Aidan D (1997) Tumeurs du corps thyroïde. EMC (Éditions Scientifiques et Médicales Elsevier SAS, Paris) 20-875-A-10.
-
Koussema ALK, Adjenou K, Amana B, Goeh AKE, Djagnikpo O, et al. (2008) Aspects échographiques des anomalies de la glande tyroïde : à propos de 134 cas. Med Afr Noire 10(1): 573-578.
-
Liénart F (2012) Le nodule thyroïdien : bénin ou malin ? Thyroid nodules: benign or malignant? Rev Med Brux 33(4): 254-262.
-
N’gouan JM, Téa ZB, Koffi-N’guessan L, Yépié A, Kouassi A, et al. (2011) La chirurgie thyroïdienne en ORL à Abidjan Rev Col Odonto-Stomatol. Afr Chir Maxillo-fac 18(1): 45-49.
-
Tanon-Anoh MJ, Yoda M, Akré A, Kouassi M, Etté-Akré E, et al. (2004) La chirurgie de la pathologie thyroïdienne bénigne en ORL et Chirurgie Cervico- faciale au CHU de Yopougon (Côte d’Ivoire). Rev Col. Odonto-Stomatol. Afr Chir Maxillo-fac 11(1): 11-15.
-
Monabéka HG, Ondzotto G, Péko JF, Kibéké P, Bouénizabila E, et al. (2005) La pathologie thyroïdienne au centre hospitalier universitaire de Brazzaville. Cah Santé 15(1): 37-40.
-
Okiémy G, Elé N, Ngouoni GB, Gombet T, Kipamboudi A (2004) Les goitres plongeants à propos de 27 cas. Med Afr Noire 51(3): 167-171.
-
Lapidus N, Ayadi S, Badier B (2008) Endocrinologie diabétologie nutrition. In: Le livre de l’externe, et al. (ED’s), 45.
-
Tajdine TM, Lamrani M, Sehrane K, AchourA, Benariba F, et al. (2005) Les goitres multihétéronodulaires plongeants : à propos de 100 cas marocains. Cah Santé 15(4): 247-252.
-
Touré A, Diallo AT, Camara LM, Toure FB, Camara ND (2006) La chirurgie thyroïdienne: expérience du service de chirurgie générale du CHU Ignace DEEN de Conakry. Mali Méd 21: 23-27.
-
Bourée P, Ouedraogo S, Tapsoba TL (2009) Apport de l’échographie dans le diagnostic de la pathologie thyroïdienne au Burkina Faso. À propos de 54 cas. Médecine d’Afrique Noire 56(3): 129-32.
-
Ayache S, Tramier B, Chatelain D, Mardyla N, Benhaim T, et al. (2005) Évolution de la chirurgie thyroïdienne vers la thyroïdectomie totale: À propos de 735 cas. Ann oto-laryngol chir cervico-fac 122(3): 127-133.
-
De Luca F, Aversa T, Alessi L, Cama V, Costanzo D, et al. (2014) Thyroid nodules in childhood: indications for biopsy and surgery. Ital J Pediatr 40(48): 1-4.
-
Zahiri K, Lakhloufi A, Chehab F, Squallid A, Khaiz D, et al. (1997) Goitre multi-hétéronodulaire bénin: à propos de 78 cas. Médecine du Magrheb 64: 21-25.
-
Moulin G (2005) Corrélations anatomo-radiologiques: pathologie thyroïdienne. J Radiol 86(10): 1228-1453.
-
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. (2009) Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19(11): 1167-1214.
-
Smith-Bindman R, Lebda P, Feldstein VA (2013) Malignancy of a thyroid nodule can be predicted but ultrasonography if it has microcalcifications and is solid and larger than 2 cm. Clin Thyroidol 25(11): 256-258.
-
Tramalloni J, Monpeyssen H, Correas JM, Hélénon O (2009) Conduite à tenir devant un nodule thyroïdien: échographie, cytoponction. J Radiol 90(3): 362-370.
-
Mackenzie EJ, Mortimer R (2004) Thyroid nodules and thyroid cancer. Med J Aust 180(5): 242-247.
-
Kim N, Lavertu P (2003) Evaluation of a thyroid nodule. Otolaryngol Clin North Am 36: 17-33.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?