Rhino-Cerebral Mucormycosis: A Case Presentation
A significant increase in incidence of rhino-cerebral mucormycosis, especially in immunosuppressed patients, we describe the successful medical and surgical management of extensive nasal mucormycosis in acute myeloid leukemia (AML) patient treated in Otolaryngology department at AFSH Cairo, Egypt. Our massage is serving your patient well and don't lose hope.
Introduction
There has been a significant increase in incidence of rhino-cerebral mucormycosis over the last two decades due to predisposing factors such as HIV/AIDS, diabetes mellitus, cancers as leukemias & lymphomas (The most common risk factor), kidney failure, organ transplant, long term corticosteroid and immunosuppressive drugs [1]. The primary therapy of mucormycosis is with an amphotericin derivative, preferably the liposomal form of amphotericin B to minimize nephrotoxicity, combined with an aggressive surgical approach and hyperbaric oxygen therapy, this prevents ascending dissemination of mucormycosis and certainly reduces the risk of patient mortality. Hyperbaric oxygen may be beneficial as an adjunctive therapy because higher oxygen pressure increases the ability of neutrophils to kill the organism [2].
In this case presentation, we describe the successful medical and surgical management of extensive nasal mucormycosis in immunocompromised patient with chronic acute myeloid leukemia (AML) treated in cooperation of Otolaryngology, oncology, and hyperbaric therapy unit at AFSH Cairo, Egypt.
Material and Methods
In May 2018, a 40-years old female patient was admitted to the oncology unit of the AFSH, with fever 39°C, vomiting, RT panful facial swelling, blackish purulent nasal discharge, fistula over her RT check (Figure 1).
The patient had a past medical history of acute Myeloid leukemia, she had bone marrow transplant six months before, in our hospital AFSH. Consultation to our ENT department for urgent management.

Obliteration of nasolabial fold, tender erythema/edema of the right upper and lower eyelids, chemosis and periorbital edema, A palatal swelling on the same side by Intraoral examination, there was an external skin fistula over the right maxilla draining pus. No pain with palpation of the palate.
- Visual acuity was markedly affected, with limited motility of the right.
- Other cranial nerve examination were normal except for loss of smell.
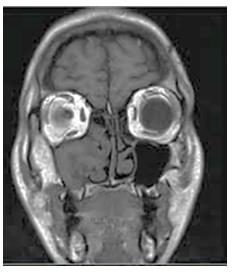
Nasal examination revealed; Blackish yellow nasal crustations in right nasal fossa with firm stony feeling of the turbinate. Ct scan and MRI done (Figure 2), show enhancing hypodense Sino-nasal soft tissue with bone rarefaction, erosion of the anterior maxilla wall, NO intra- orbital and intracranial extension laboratory values on admission were as follows: (Figure 3), marked diminished platelet count, platelets were only 7,000 per microliter, abnormal.
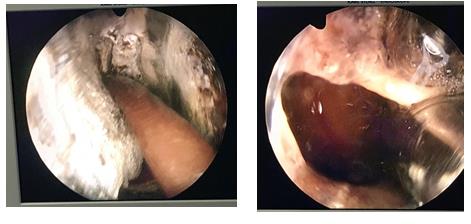
Medications was started at once in the form of; liposomal form of amphotericin B (Ambisome 150 mg), IV route, every 24 hours duration, slowly infusion for an hour, for one month. Other medications like (Zovirax, Surgery; Emergency endoscopic bilateral ethmoidectomy was performed. Endonasal surgery was immediately undertaken, comprising right ethmoidectomy and right medial meatotomy (Figure 4), and with histopathology, bacteriology and mycologic sampling.
Functional endoscopic nasal surgery was done in the typical maneuver but no anatomical land marks were seen during surgery except for the middle turbinate, the tissues were hard fibrous brawny color and friable, by experience we did middle meatal antrostomy, a large amount of blood stained sticky mucoid pus drained out, next we smoothly widening the antral medial wall, we irrigation all the cavity with, no anatomic land marks for the anterior and posterior ethmoid just egg shell bone covering was removed genially for fear of CSF leak and bleeding and we could reach the sphenoid sinuses with posterior choana and medial to the septum land marks. Time of operation was two hours, fortunately no blood transfusion was needed, the bleeding intraoperatively was minimal or no bleeding at all.
Management


Hyperbaric Oxygen Therapy
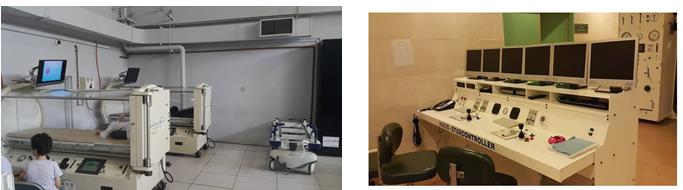
On the second day of operation started, in daily manner, for 20 sessions, it is a specialized medical treatment which involves the intermittent inhalation 100% under a pressure greater than one atmosphere (Figure 5).
Results
Results were favorable as of the first week, with cessation of pain and regression of the hemifacial edema. Body temperature is regulated around a set point of 37 ± 1°C, fever and Chills disappeared dramatically.
patients with headache recovered after treatment, the visual acuity recovered to the hand movement, we saved the patient palate as no palatal perforation occurred, skin care done for the facial fistula which healed within days. Histopathology tests showed fragments of necrotic connective tissue associated with spores and stubby and broad hyphae, associated with signs of ischemic necrosis, confirming diagnosis of mucormycosis [3, 4].
Follow up done every other day in the patient isolated room (oncology department), surgical cavity was cleaned conservatively and we courage the patient to perform nasal wash with normal and hypertonic saline nasal 4-5 time a day. At 4 months, on readmission for surveillance, the clinical symptomatology had resolved, but sinus CT found persistent lysis of the skull base, ethmoid. Osteolysis of the right mandible after multiple tooth extractions, no further complementary surgery was needed.
Discussion
Early warning signs of diagnosis of mucormycosis in immunocompromised patient with sinusitis are blood stained nasal discharge painless palpation of the nasal turbinates and fossa, eye and palatal swelling, alarm you for primary interference as in our case.
Treatment of rhinocerebral mucormycosis requires a multifaceted approach, since tissue necrosis during mucormycosis can result in poor penetration of antifungal agents to the site of infection. Therefore, debridement of necrotic tissues may be critical for complete eradication of mucormycosis. Ct scan and MRI imaging plays a vital role in detection and delineating the spread and extent of bony involvement, perineural, intra-orbital and intracranial extension of mucormycosis which is vital to therapeutic decision making. In our case we were encourage after studying the images results because the disease was limited but need rapid interference, we made all procedures to elevate the platelet count, in collaboration with the blood transfusion unit in our hospital. As the platelets count were only 7,000 per microliter, with severe thrombocytopenia.
As we described the operation was done in the typical maneuver but no anatomical land marks were seen during surgery, except for the middle turbinate fortunately no blood transfusion was needed, the bleeding intraoperatively was minimal or no bleeding at all. We recommend to use AmBisome vial, for the treatment of severe systemic mycoses, it’s less toxic than conventional amphotericin B, particularly with respect to nephrotoxicity, we also advice to practice Hyperbaric Oxygen Therapy in treatment for invasive fungal infections, since it reduces tissue hypoxia and the vascular insufficiency.
Conclusion
There are critical factors for eradicating mucormycosis; Rapidity of diagnosis, Reversal of the underlying predisposing factors (if possible), Appropriate surgical debridement of infected tissue, appropriate antifungal therapy. The further progress of these life- threatening fungal infections with a depends on early and definitive diagnosis and radical surgical therapy to reduce the amount of infectious agent.
References
-
Rapidis AD (2009) Orbitomaxillary mucormycosis (zygomycosis) and the surgical approach to treatment: perspectives from a maxillofacial surgeon 15(5): 98-102.
-
Saraiya HA (2014) Successful management of cutaneous mucormycosis ESCMID and ECMM Joint Clinical guidelines mucormycosis. Clinical Microbiology and Infection 20(3): 5-26.
-
Wingard JR, Majhail NS, Brazauskas R, Wang Z, Sobocinski KA, et al. (2011) Longterm survival and late deaths after allogeneic hematopoietic cell transplantation. J Clin Oncol 29(16): 2230-2239.
-
Yohi RA, Bullock JD, Aziz AA, Markert RJ (1994) Survival factors in rhino-orbital-cerebral mucormycosis. Surv Ophthalmol 39(1): 3-22.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?