A Case of Primary Syphilis Masquerading as Tonsil Carcinoma
We present a case of a man who presented with unilateral odynophagia, an enlarged tonsil and an ipsilateral neck lump. The diagnosis was presumed to be carcinoma of the tonsil and he was investigated as such. During the period of investigation, he self-referred to a genitourinary medicine clinic and was diagnosed with primary syphilis. After treatment with antibiotics his signs and symptoms completely resolved.
Case History
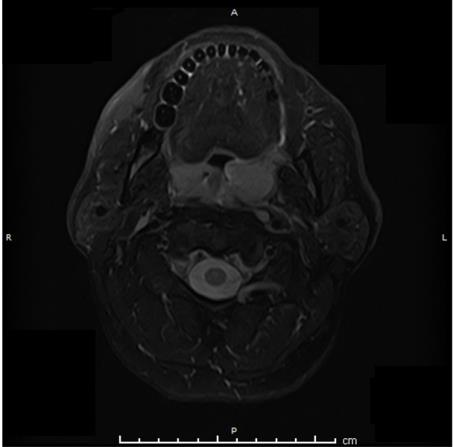
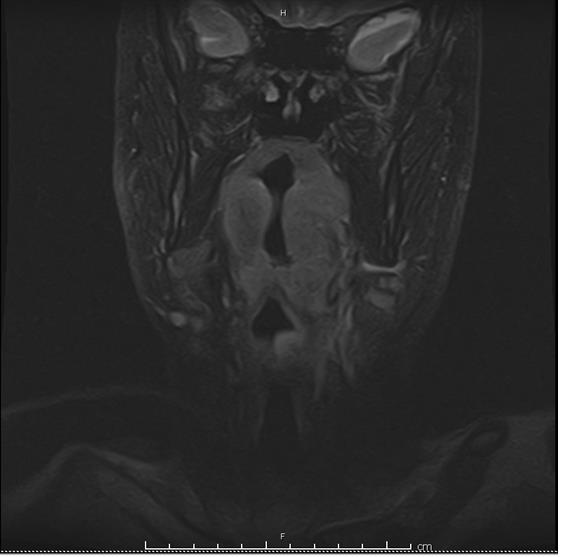
A 47 year old man was referred by his GP to ENT clinic with a 2 month history of left sided odynophagia, left neck lump and 1 stone weight loss. The gentleman denied smoking, drinks alcohol rarely and works both in an office and as a delivery driver. His past medical history included controlled hypertension and childhood epilepsy but had been seizure free for 10 years. On examination, he displayed a large mass of his left tonsil which was indurated to palpation as well as a firm, fixed left level 2 neck node. Clinically, the case was strongly consistent with carcinoma of the tonsil with ipsilateral nodal disease. An MRI and ultrasound neck as well as CT chest was requested. The MRI showed a grossly enlarged left tonsil (Figures 1 & 2).
The Ultrasound revealed a 25.2mm lymph node in the left level 2 region of the neck with pathological features (Figure 3). The node underwent fine needle aspiration cytology (FNAC) however, this showed reactive lymphoid cells only with no evidence of malignancy.

In view of the likely diagnosis of tonsillar malignancy, a panendoscopy and biopsy of the tonsil was organised. However, in the meantime, the patient presented to the genitourinary medicine clinic for a routine appointment. The patient was diagnosed with primary syphilis and received a 2 week course of doxycycline. After 2 weeks his lymphadenopathy, tonsil mass and odynophagia symptoms had all resolved.
Discussion
The incidence of tonsil cancer has tripled over the last 30 years [1]. In the UK, new cases have risen from 459 in 1985 to 1462 in 2015 [1, 2]. The reason for this is likely to be multifactorial however Human papilloma virus (HPV) plays an important role; half of all tonsil cancers are caused by HPV [3, 4] as opposed to the traditional risk factors of smoking and alcohol. Excluding a malignancy in any patient who presents with a tonsil mass is a priority however, as this case illustrates, other differential diagnoses should be considered.
Differential Diagnoses
A retrospective literature review of 20 studies with 54,901 patients. Randall DA, et al. [5] found that only 0.087% of patients who underwent tonsillectomy for unilateral tonsil enlargement alone had underlying malignant pathology. The majority of unilateral tonsillar enlargement is due to chronic inflammation, Actinomycoses sp. infection or lymphoid hyperplasia [6]. However, non-epithelial malignancies may present with unilateral tonsillar enlargement, the most common of which is lymphoma [7], furthermore systemic infections such as TB [8] and in this case, syphilis should also be a consideration.
Syphilis in ENT
Syphilis is a sexually transmitted infection caused by the spirochete Treponema pallidum. The disease is categorised into 4 stages following infection; primary, secondary, latent and tertiary. Primary syphilis most commonly presents with an ulcerative lesion (chancre) at the site of contact which is usually the genitals [9] however, albeit rarely, primary syphilis may present as an oropharyngeal lesion; a 2017 literature review identified 12 previous published cases of primary syphilis presenting with a tonsillar ulcer or unilateral tonsil enlargement [10]. Regional lymphadenopathy, as in our case, is found in up to 80% of cases [9]. Secondary syphilis occurs between 2-12 weeks following initial infection due to haematological dissemination of the bacteria and most commonly presents with a maculopapular skin rash. However, several manifestations may occur including lymphadenopathy, iritis, uveitis, arthritis, hepatitis and, pertinent to the ENT surgeon, multiple grey / white oral mucosal pseudomembranous lesions as well as non- specific pharyngitis, tonsillitis and laryngitis [11].
Tertiary Syphilis occurs 3-15 years after initial infection if left untreated and may manifest as gummatous disease, cardiovascular syphilis or neurosyphilis. The latter is due to central nervous system involvement and may present with a picture of meningitis, paresis, seizures or rarely, otosyphilis; which may present to the ENT surgeon with symptoms of sensorineural hearing loss and vertigo [12]. Syphillis may be diagnosed with dark field microscopy of material from primary lesions, serological testing for treponema antibodies or CSF analysis in the case of neurosyphilis [11]. Treatment with antibiotic therapy (penicillin, unless contraindicated) is required for any stage of syphilis infection.
Conclusion
In summary, this case represents a rare presentation of unilateral tonsillar enlargement but serves to highlight the importance of considering a broad range of differential diagnoses when faced with a similar case. Although the majority of unilateral tonsillar enlargement is due to benign or reactive pathology and excluding a carcinoma should remain a primary concern, the ENT surgeon must be aware of alternate causes and direct a history, examination and investigations appropriately.
References
-
Reddy VM, Cundall-Curry D, Bridger MWM (2010) Trends in the incidence rates of tonsil and base of tongue cancer in England, 1985–2006. Ann R Coll Surg Engl 92(8): 655-659.
-
Cancer Research UK. (2018) Oral Cancer http://www.cancerresearchuk.org/health- professional/cancer-statistics/statistics-by-cancer- type/oral-cancer/incidence#heading-Four. [Accessed 11 April 2018].
-
(2007) Human Papillomaviruses, IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 90. IARC Working Group on the Evaluation of Carcinogenic Risk to Humans. Lyon (FR): International Agency for Research on Cancer.
-
Klussmann JP, Gültekin E, Weissenborn SJ, Wieland U, Dries V, et al. (2003) Expression of p16 Protein Identifies a Distinct Entity of Tonsillar Carcinomas Associated with Human Papillomavirus. Am J Pathol 162(3): 747-753.
-
Randall DA, Martin PJ, Thompson LD (2007) Routine histologic examination is unnecessary for tonsillectomy or adenoidectomy. Laryngoscope 117(9): 1600-1604.
-
Papouliakos S, Karkos PD, Korres G, Karatzias G, Sastry A, et al. (2009) Comparison of clinical and histopathological evaluation of tonsils in pediatric and adult patients. Eur Arch Otorhinolaryngol 266(8): 1309-1313.
-
Lifshitz G, Gruber M, Ronen O (2019) Occult malignancy in pediatric tonsil and adenoid surgeries- A national survey. Int J Pediatr Otorhinolaryngol 117: 171-174.
-
Das A, Sibes K Das, Sudipta P, Sumitra B (2015) Tonsillar Tuberculosis: A Forgotten Clinical Entity. J Family Med Prim Care 4(1): 124-126.
-
Kent ME, Romanelli F (2008) Reexamining syphilis: an update on epidemiology, clinical manifestations, and management. Ann Pharmacother 42(2): 226-236.
-
Yang CH, Su TY, Chang KP, Lee LY (2017) Case Report Primary syphilis of the tonsil: a case report and literature review. Int J Clin Exp Med 10(9): 13916- 13919.
-
Ficarra G, Carlos R (2009) Syphilis: The Renaissance of an Old Disease with Oral Implications. Head Neck Pathol 3(3): 195-206.
-
Theeuwen H, Whipple M, Litvack JR (2019) Otosyphilis: Resurgence of an Old Disease. Laryngoscope 129(7): 1680-1684.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?