Surgical Innovation: Advanced Strategies in the Treatment of Pathologies in the Oropharynx and Parapharyngeal Space
Transoral surgery has evolved and its indications for treating diseases of different regions of the head and neck have increased. Pathologies that affect different sectors of the oropharynx and parapharyngeal space can be treated in selected patients through a transoral approach, significantly reducing the morbidity of surgery and the adjuvant treatments. Objectives: To determine the effectiveness of transoral surgery of the oropharynx and parapharyngeal space in patients treated with transoral surgery with microscope (TOMS) for tumors and other pathologies. Methods: Patients treated via transoral approach with the assistance of endoscopes or using a microscope for benign or malignant tumors, as well as other pathologies affecting different regions of the oropharynx (tonsillar fossa, tongue base, and pharyngeal walls) and the parapharyngeal space, between March 2004 and April 2022, were included in the study. To perform the surgeries, cautery, ultrasonic scalpel and CO2 laser were used. Results: Twenty patients with different lesions affecting various regions of the oropharynx and parapharyngeal space were treated using a transoral approach. Ten patients underwent surgery for lesions located at the base of the tongue, two were treated for tumors located in the tonsillar fossa, four patients had lesions located in the posterior and lateral walls of the oropharynx and four patients had lesions located in the parapharyngeal space. Conclusions: Transoral surgery of the oropharynx and parapharyngeal space assisted with endoscopes was highly effective, allowing adequate exposure and complete resection of various benign and malignant tumors, as well as the resolution of other diseases treated using this approach. There was no need to convert the transoral approach to an open procedure. The use of microsurgical technique was infrequent, and we found it to be more suitable for small tumors at the base of the tongue or lesions located in the lower sector of the posterior pharyngeal wall.
Introduction
Transoral surgery has experienced significant evolution with the use of laser microsurgery to treat laryngeal cancer. This approach has been extended and applied to diseases affecting other regions of the head and neck, such as the oropharynx and parapharyngeal space. The development of technology and new knowledge about oropharyngeal cancer have facilitated and made possible the application of these surgical techniques to resect tumors from these regions. The benefits of this approach are reducing the morbidity of surgery by avoiding external approaches, gastrostomies, tracheostomies, and also avoiding or reducing adjuvant treatments that can cause morbidity and complications.
Objectives
To determine the effectiveness of transoral surgery of the oropharynx and parapharyngeal space in patients treated with transoral surgery with microscope (TOMS) for tumors and other pathologies.
Design
Descriptive and retrospective.
Materials and Methods
Patients treated via transoral approach with the assistance of endoscopes or using a microscope for benign or malignant tumors, as well as other pathologies affecting different regions of the oropharynx (tonsillar fossa, base of the tongue, and pharyngeal walls) and the parapharyngeal space, between March 2004 and April 2022, were included in the study.
Patients with superficial lesions on the base of the tongue such as vallecular cysts, hypertrophy of lingual tonsils, and neoplasms located in the soft palate were excluded.
For malignant tumors, a resection margin of > or = 2mm (R=0) was considered adequate, and a margin less than 2mm was considered close. Surgeries were performed under general anesthesia with orotracheal intubation.
Four millimeters endoscopes with 0º and 30º angles, similar to those used in endoscopic sinus surgery, and a Storz tower with full HD endocamera were used. In other cases, a microscope and laryngoscopes of different diameters were used.
For surgeries involving tumors of the base of the tongue, a Jennings mouth gag was used, an anterior point was made for traction, and then the hemibase of the tongue was resected, either its central sector or a total glossectomy was performed. In cases of malignant tumors, frozen biopsies were performed or the surgical specimen was examined intraoperatively to ensure clear resection margins.
Resections were performed in bloc. The raw area on the base of the tongue was allowed to heal by secondary intention. In the patient who underwent a total glossectomy, reconstruction was performed using a free flap, utilizing the transoral approach.
The central part of the oral tongue and the base of the tongue were resected in a patient with sleep apnea, and in a patient with ectopic lingual thyroid, the lesion was excised through an incision at the V lingual level, deepening the dissection until complete lesion removal.
In two cases, an incision was made in the ventral sector of the tongue, 1cm above the Wharton’s ducts opening, and two giant epidermoid cysts compromising the base of the tongue were dissected and removed.
For malignant tumors of the tonsillar fossa, radical tonsillectomy (resection of the superior constrictor muscle while preserving the buccopharyngeal fascia) with intraoperative margin control and selective lateral neck dissection was performed, while for a benign tumor, partial resection of the constrictor muscle was done.
For tumors in the posterior or lateral wall of the oropharynx, microsurgery technique was used in some cases, while endoscopes were used in others to expose and resect the lesions.
For tumors in the parapharyngeal space, an arcuate incision was made in the palate using a cautery, dividing the palatal muscles and the superior pharyngeal constrictor. Myomucosal flaps were dissected to expose the tumors, and extracapsular dissection was performed with the assistance of endoscopes. The neoplasms were completely excised without fragmentation.
Using the same technique, an elongated styloid process (Eagle Syndrome) was resected.
Most of the patients had the postoperative period in intermediate therapy.
Functional swallowing assessment was performed 24 hours after surgery in some cases.
Surgery was considered successful when complete resection of malignant and benign tumors was achieved and when the transoral approach did not need to be converted to an open approach.
Results
Twenty patients with different lesions affecting various regions of the oropharynx and parapharyngeal space were treated using a transoral approach at the Italian Hospital of Buenos Aires and the Central Polyclinic of UOM. Sixteen were female and four were male, with an average age of 53.95 years (23-81).
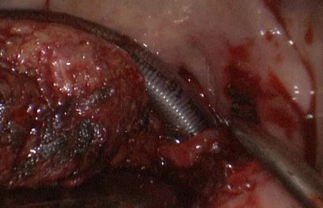
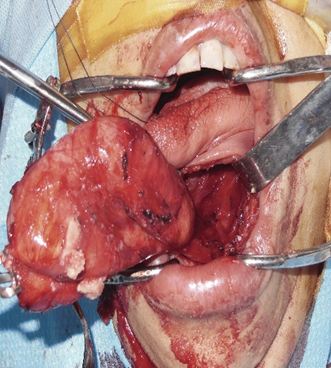
Ten patients underwent surgery for lesions located at the base of the tongue. Four of them had malignant tumors, two of which required central oral glossectomy and tongue base resection, while another underwent oral hemiglossectomy and tongue base resection (Figures 1 & 2).

A B C Figure 1: Adenoid-Cyst Carcinoma- A: MRI; B: Transoral Tongue Base Resection (Endoscopic Vision); C: Postoperative MRI.
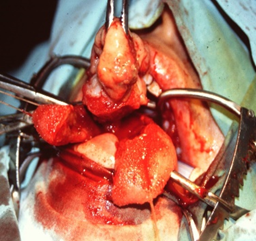
In one patient, total glossectomy was performed with simultaneous reconstruction using an anterolateral thigh free flap, performed by a transoral approach without mandibulotomy and with tracheostomy (Figure 3).
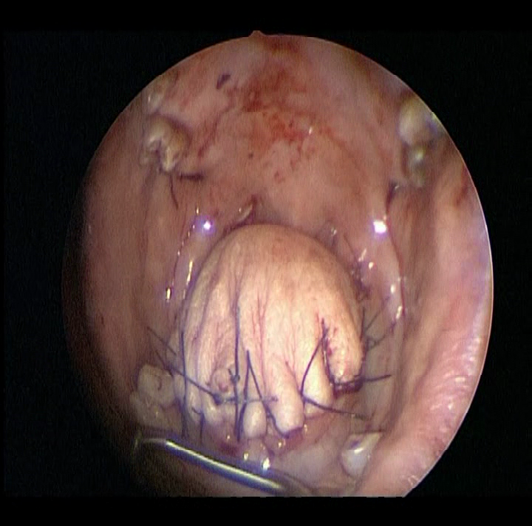

A B C Figure 3: Total Glossectomy – A: Transoral Endoscopic Resection; B&C: Anterolateral Thigh Free Flap.
Selective bilateral cervical lymph node dissection was performed in one patient with stage T3-N0 squamous cell carcinoma. In all patients with malignant tumors of the tongue base, clear margins were achieved except in the patient who underwent total glossectomy, where there was a discrepancy between the intraoperative report (R0) and the final pathology report (close margin). No recurrences were detected during the follow-up period for one year (leiomyosarcoma) and five-years (squamous cell carcinoma). The patient treated for adenoid cystic carcinoma had a recurrence five years later, therefore a total transoral glossectomy was performed.
No recurrences were detected during the two-year follow-up period.
Two patients had giant epidermal cysts in the ventral region and at the base of the tongue, which were completely resected using a ventral approach and assisted endoscopic dissection (Figure 4).
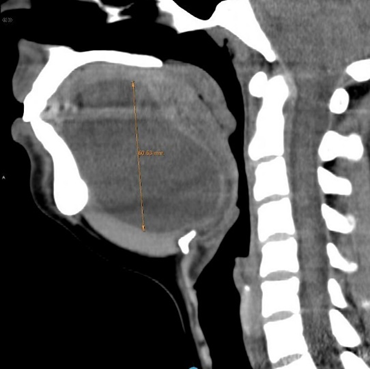
A B Figure 4: Epidermal Cyst of the Tongue: A CT; B: Transoral Endoscopic Ventral Resection.
One patient underwent resection of a lingual thyroid that could not be exposed at another center using transoral microsurgery technique, while another patient had deep tumor excision located at the base of the tongue, which turned out to be necrotizing sialometaplasia.
In an asymptomatic woman who had a tumor at the base of the tongue and could not be intubated during a gynecological surgery, subtotal transoral tumor resection was performed, revealing a deep muscular plane cyst. In a patient with Down syndrome, macroglossia, and severe apneas, who did not adhere to CPAP therapy, central oral glossectomy and tongue base resection were performed (Figure 5).

Nine patients underwent transoral resection with endoscopic assistance, and one patient underwent microsurgery technique. Electrocautery (7/10) and ultrasonic scalpel (3/10) were used for deep muscular plane resections at the base of the tongue.
Two patients had tumors located in the tonsillar fossa, one with pT2 pN1 squamous cell carcinoma, Mx, P16+. All margins assessed by intraoperative biopsies were negative, but the final pathology report indicated involvement of one lateral margin (R1), while the deep margin was adequate (1cm). Due to this discrepancy between intraoperative and postoperative histopathological studies, radiation therapy was recommended. No recurrences were detected during the 4-year follow-up period. Four patients had lesions located in the posterior and lateral walls of the oropharynx. Two
vascular malformations were operated without embolization, and two patients had extensive cysts. Complete resection was achieved in all cases. Microsurgery technique was used for lesions located inferiorly in two patients, while endoscopic- assisted surgery was performed in the other two.
Four patients had lesions located in the parapharyngeal space. Two of them had moderate-grade mucoepidermoid carcinomas, located in the parotid and masticator spaces.
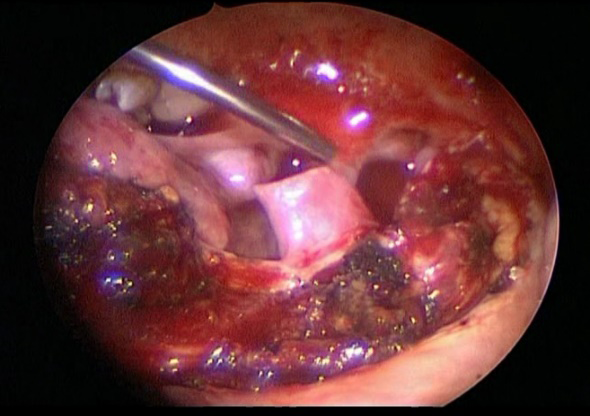
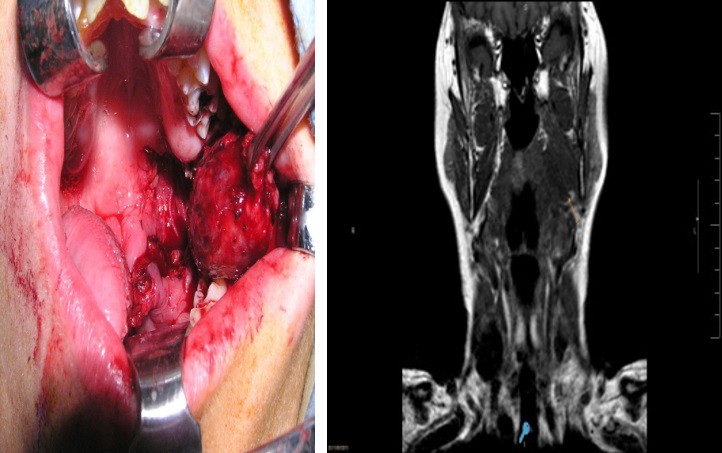
The resection was extracapsular and without fragmentation, and during the 2-year and 5-year follow-up periods, no recurrences were detected, respectively. Another patient had a giant pleomorphic adenoma in the deep lobe of the parotid gland, which was completely resected without fragmentation (Figure 6).
A B C D Figure 6: Parotid Space Mucoepidermoid Carcinoma. A, B: coronal and axial MRI, C: endoscope-assisted transoral resection, D: postoperative MRI.
In a patient with refractory facial and cervical pain despite multiple previous treatments, transoral styloidectomy was performed, resulting in symptom resolution.
No intraoperative or immediate postoperative complications were encountered (Table 1).
| Age/sex | Location | Pathology | Exposure | Surgery | Tracheostomy/ nasogastric tube | Adjuvant treatment | Complications |
|---|---|---|---|---|---|---|---|
| F/32 | oral, and tongue base | leiomyosarcoma | +++ | central oral and tongue base glossectomy (endoscopes) electro- cautery | no | no | no |
| F/71 | oral and tongue base | squamous cell carcinoma T3N0M0 | +++ | oral and tongue base hemiglossectomy (endoscopes) + selective lateral dissection electro-cautery | no | RT | no |
F/68 tongue base adenoid cystic carcinoma +++
F/73 tongue base adenoid cystic carcinoma +++
F/36 tongue base lingual thyroid +++ resection (endoscopes) ultrasonic scalpel no no no F/36 oral and tongue base macroglossia/ severe SAHS +++ F/35 oral and tongue base epidermal cyst +++ ventral submucosal resection (endoscopes) electro-cautery no no no F/32 oral and tongue base epidermal cyst +++ F/71 tongue base mucous retention cyst +++ partial resection (microscope) electro- cautery no no no F/32 tongue base necrotizing sialometaplasia +++ total resection (microscope) electro- cautery no no no M/69 tonsillar fossa squamous cell carcinoma pT2 pN1 Mx/P16+ +++ radical tonsillectomy + selective neck dissection electro-cautery no RT no M/68 tonsillar fossa / soft palate basal cell adenoma +++ tonsillectomy + soft palate resection electro- cautery no no M/58 posterolateral pharyngeal wall cyst +++ total submucosal resection (endoscopes) electro-cautery no no F/68 posterior pharyngeal wall F/24 posterior pharyngeal wall vascular malformation +++ F/66 lateral pharyngeal wall cyst +++ total resection (microscope) electrocautery no no F/81 parotid space moderate grade mucoepidermoid carcinoma +++ total resection (endoscopes) electrocautery no RT no hemiglossectomy of the base of the tongue (endoscopes) ultrasonic scalpel no no no total glossectomy (endoscopes) + free flap reconstruction ultrasonic scalpel tracheostomy and gastrostomy RT no central oral and base glossectomy (endoscopes) electro- cautery no no ventral submucosal resection (endoscopes) electro-cautery electrocautery no no no venous malformation +++ total resection (endoscopes) electrocautery no no total resection (endoscopes/ microscope) electro- cautery
- moderate grade mucoepidermoid carcinoma
- +++ total resection (endoscopes) electrocautery no
- RT no
- F/23 masticator space total resection (endoscopes) electrocautery electrocautery
- F/79 parotid space pleomorphic adenoma
- +++
- M/57 parapharyngeal space
- Eagle syndrome
- +++ total resection (endoscopes) electrocautery no no
Table 2: Patients Treated by Transoral Surgery (Rt: Radiotherapy, +++: Good Exposure).
Discussion
Transoral surgery of the oropharynx can be performed using different surgical techniques and with different levels of technological complexity.
The microsurgery technique involves the use of a microscope and conventional or bivalve laryngoscopes of different diameters. It has been described using CO2 laser, which does not have significant coagulation power. We have used this technique in two patients with localized lesions in the pharyngeal wall located inferiorly and in one patient with a 1cm glandular lesion located deep in the base of the tongue, where an incision in the lingual V and further deepening of the dissection would have caused greater morbidity. The surgeries were performed using cautery.
Exposing the base of the tongue can be challenging in some patients, and the field of vision is limited as it is obtained through the diameter of the laryngoscope, which needs to be repositioned multiple times. The vision is tangential and not at angles.
In the case of using this technique to treat malignant tumors, the neoplasm resection is performed in parts.
The transoral approach with the assistance of endoscopes allows us to have magnified and angled vision, which we find very useful, especially in base of tongue surgery. 3D systems can be used to obtain three-dimensional vision.
By making an incision at the lingual V level in front of the tumor and deepening the dissection, the use of the endoscope provides an excellent view of the entire base of the tongue, vallecula, and lingual surface of the epiglottis, facilitated by the 30-degree angle or by tilting the endoscope.
This surgery also has the advantage of preserving the surgeon’s tactile sensation, and the tumor resection is in bloc.
The combination of transoral surgery with endoscopes and the use of the ultrasonic scalpel for cutting and coagulation is called TOUSS [1].
The ultrasonic scalpel transfers high-frequency mechanical vibrational energy (25-55 kHz) to the tissues, producing a lower cutting/coagulation temperature compared to CO2 laser or cautery. It incorporates a bipolar system that can seal vessels up to 7mm, which is similar in size to the lingual or superior laryngeal artery.
Retractors, self-retaining systems, laparoscopy sets, endoscopes, and endocameras with 2D or 3D systems are used.
We have used the ultrasonic scalpel in three patients with base of tongue tumors, and the coagulation was better than with other equipment.
Another possibility for transoral surgery is the Da Vinci robotic system (TORS).
The most frequent indication for transoral surgery is probably in squamous cell carcinomas of the base of the tongue and tonsil.
Weiss BG, et al. [2] reported on 368 patients treated for pT1-4, pN0-2, M0 squamous cell carcinomas of the oropharynx with transoral laser microsurgery +- neck dissection (85%) and +- chemoradiotherapy (57%). They achieved a 5-year local control rate of 83.5% for pT1, 74.1% for pT2, 77.3% for pT3, and 76% for pT4a. The disease- specific survival was 85.1% for pT1 and 74.3% for pT2 (76.5% for pT1-4a). According to the stage, the disease- specific survival was as follows: Stage I: 92.8%, Stage II: 85.7%, Stage III: 72.5%, and Stage IVa: 73.7% (Stage I-IVa: 76.5%). P16-positive patients had better survival, and 93.5% maintained adequate swallowing without a nasogastric or gastrostomy tube.
Moore EJ, et al. [3] reported a 5-year disease-specific survival rate of 94% in 314 patients with squamous cell carcinomas of the tonsil and base of tongue (81.6% were pT1-2, and 91.1% were p16+) treated with transoral robotic surgery (TORS) and neck dissection, +- chemoradiotherapy. The results of both studies are similar, but Weiss et al. included more patients with advanced stages.
In a meta-analysis [4] comparing TORS with intensity- modulated radiation therapy (IMRT) in 5624 patients (IMRT, n = 4322; TORS, n = 1302), the majority of patients treated with IMRT received concurrent chemotherapy, and the majority of patients treated with TORS received adjuvant treatment (67.8%). The disease-free survival rate was 79.6% for the IMRT group and 89.4% for the TORS group. The rates of dependence on nasogastric feeding and tracheostomy were similar in both groups.
In our series, one patient with oral tongue and base squamous cell carcinoma (T3-N0-M0) started oral feeding after transoral surgery but required a gastrostomy at the end of radiotherapy. Three years later, she presented with inspiratory dyspnea due to bilateral vocal cord adduction paralysis, leading to a tracheostomy. No cancer recurrence was detected, illustrating the morbidity that can be caused by adjuvant treatments.
Some consider a surgical margin to be close when it is 2mm or less and tumor-free when it is larger than 2mm, while others use a 5mm cutoff [5]. According to Hinni ML, et al. [6] obtaining margins greater than 5mm in depth in tonsil tumors is not possible, as the thickness of the constrictor muscle measured in preoperative magnetic resonance imaging was 2.4mm.
In another study of 425 patients, a close margin (<2mm) or a positive margin was a significant prognostic factor when compared to a negative margin. The close margin did not impact survival [7]. In a multicenter study of patients treated with TORS for oropharyngeal tumors, the incidence of positive margins was 3.8% [5]. Moore EJ, et al. [8] reported involved margins in 3.9% of 102 patients treated for tonsil cancer with non-robotic transoral surgery, and Grant DG, et al. [9] had a positive margin rate of 3.4% in patients treated with transoral surgery for base of tongue tumors.
In our series of malignant oropharyngeal tumors, we achieved clear margins based on intraoperative histopathological examination of the surgical specimen or margin biopsies in five patients (5/5). In the deferred histopathological examination, one patient had a close margin (1mm), and another had a compromised lateral margin (R1).
Parimbelli E, et al. [10] compared TORS with transoral surgery to determine which technique was more cost- effective and reported that transoral surgery was more cost- effective (equipment cost), but this advantage was sensitive to the prescription of postoperative adjuvant treatments and the number of reoperations. The number of reoperations performed after transoral surgery was higher than with TORS, favoring the cost-effectiveness of the latter technique. In another study of 1467 patients treated with transoral surgery for tumors of the oral cavity, oropharynx, larynx, and hypopharynx, 386 patients (26.3%) underwent a second resection, and of those, 22 had a third and fourth transoral surgery [11].
Shenouda K, et al. [12] compared two cohorts of patients with T1-T2 oropharyngeal squamous cell carcinomas operated with a transoral approach. TORS was used in 21 patients, and non-robotic transoral surgery was used in 24 patients. The 3-year and 5-year overall survival rates were 80.2% and 74.5%, respectively, in the TORS group and 91.5% and 82.5% in the non-TORS group. The local control rate at 3 and 5 years was 90% in the TORS group and 95.8% in the non- TORS group. They did not report differences in morbidity, need for tracheostomy/nasogastric tube, or hospital stay. The incidence of positive margins (R1) was 38.1% in TORS and 16.7% in non-TORS, but this did not have a significant impact on the 5-year survival. They concluded that lateral oropharyngectomy with TORS for T1-T2 tonsil carcinomas did not significantly impact oncological or functional outcomes. In another study comparing the results of transoral surgery, non-robotic transoral surgery, and TORS, similar oncological and functional outcomes were reported [13]. Transoral surgery of the parapharyngeal space is another technique that has evolved from being contraindicated to becoming a first-line surgery in selected patients [14, 15].
Tumors of the parotid (deep lobe) or masticator space are the ones most frequently treated with a transoral approach. In a literature review on transoral surgery for tumors of the parotid gland, they reported 139 patients treated with this surgical technique, and the most frequent histology was pleomorphic adenoma (116: 84.1%). Transoral approach was performed in 125 cases (89.9%), while the combination of transoral and transcervical-transparotid approach was done in 14 patients (10.1%). TORS was performed in 55 cases (39.5%) of the transoral approaches and in 11 cases (7.9%) of the combined approaches. Transoral approach assisted with endoscopes was used in 41 patients (29.5%). Complications were reported in nine cases, representing 6.5%. The complications included pharyngeal dehiscence (2/9), deep cervical seroma/sialocele (2/9), facial nerve paralysis (2/9), and skin hyperemia at the angle of the jaw (1/9) [16]. We believe that achieving clear margins is similar to what is accomplished with external surgeries using transparotid or cervical approaches, and even with mandibulotomy. While these approaches provide a larger surgical field, deeper dissection often results in the tumor being dissected from the pharyngeal wall or the base of the skull using blind “surgeon’s finger” or by placing an endoscope to partially enhance visibility. All three tumors treated with this surgical technique were completely resected without fragmentation, but compromised margins (R1) were detected in the two malignant neoplasms. Therefore, due to this reason and the intermediate histological grade of malignancy, postoperative radiotherapy was indicated.
Conclusions
Transoral surgery of the oropharynx and parapharyngeal space assisted with endoscopes was highly effective, allowing adequate exposure and complete resection of various benign and malignant tumors, as well as the resolution of other diseases treated using this approach.
There was no need to convert the transoral approach to an open procedure.
The use of microsurgical technique was infrequent, and we found it to be more suitable for small tumors at the base of the tongue or lesions located in the lower sector of the posterior pharyngeal wall.
• Declaration of Conflicts of Interests No conflicts of interest were declared.
References
-
Fernandez-Fernandez MM, Montes-Jovellar L, Arias PLP, Alamo POD (2015) TransOral endoscopic UltraSonic Surgery (TOUSS): a preliminary report of a novel robotless alternative to TORS. Eur Arch Otorhinolaryngol 272(12): 3785-3791.
-
Weiss BG, Ihler F, Anczykowski MZ, Bertlich M, Kitz J, et al. (2019) Transoral laser microsurgery for treatment of oropharyngeal cancer in 368 patients. Head & Neck pp: 3144-3158.
-
Moore EJ, Abel KMV, Price DL, Lohse CM, Olsen KD, et al. (2018) Transoral robotic surgery for oropharyngeal carcinoma: surgical margins and oncologic outcomes. Head Neck 40(4): 747-755.
-
Virgilio AD, Costantino A, Mercante G, Pellini R, Ferreli F, et al. (2021) Transoral robotic surgery and intensity- modulated radiotherapy in the treatment of the oropharyngeal carcinoma: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol 278(5): 1321- 1335.
-
Weinstein GS, Malley BWO, Magnuson SJ, Carroll WR, Olsen KD, et al. (2012) Transoral Robotic Surgery: A Multicenter Study to Assess Feasibility, Safety, and Surgical Margins Transoral, Laryngoscope 122(8): 1701-1707.
-
Hinni ML, Zarka MA, Hoxworth JM (2013) Margin Mapping in Transoral Surgery for Head and Neck Cancer. Laryngoscope 123(5): 1190-1198.
-
Binahmed A, Nason RW, Abdoh AA (2007) The clinical significance of the positive surgical margin in oral cancer. Oral Oncol 43(8): 780-784.
-
Moore EJ, Henstrom DK, Olsen KD, Kasperbauer JL, Mcgree M (2009) Transoral resection of tonsillar squamous cell carcinoma. Laryngoscope 119(3): 508- 515.
-
Grant DG, Salassa JR, Hinni ML, Pearson BW, Perry PAC WC (2006) Carcinoma of the tongue base treated by transoral laser microsurgery, part two: Persistent, recurrent and second primary tumors. Laryngoscope 116: 2156-2161.
-
Parimbelli E, Soldati F, Duchoud L, Almeida JD, Broglie M, et al. (2021) Cost-utility of two minimally-invasive surgical techniques for operable oropharyngeal cancer: transoral robotic surgery versus transoral laser microsurgery. BMC Health Services Research pp: 1173.
-
Jackel MC, Ambrosch P, Martin A, Steiner W (2007) Impact of re-resection for inadequate margins on the prognosis of upper aerodigestive tract cancer treated by laser microsurgery. The Laryngoscope 117(2): 350-356.
-
Shenouda K, Rubin F, Garcia D, Badoual C, Bonfils P, et al. (2020) Evaluation of robotic surgery for transoral resection of T1-2 squamous cell carcinoma of the tonsillar fossa. European Annals of Otorhinolaryngology, Head and Neck diseases 137(1): 31-36.
-
Jackson R, Ross E, Jose J (2021) Endoscopic video‑assisted transoral (EVAT) surgery of the oropharynx:clinical, oncological and functional outcomes. European Archives of Oto-Rhino-Laryngology 278(11): 1-10.
-
Larson AR, Ryan WR (2021) Transoral Excision of Parapharyngeal SpaceTumors. Otolaryngol Clin N Am 54(3): 531–541.
-
Lao WP, Han PS, Lee NH, Gilde JE, Inman JC (2020) Transoral Excision of Parapharyngeal Tumors. Ear Nose & Throat Journal 100(10): NP454-NP458.
-
Riva G, Lorenzi A, Borello A, Albera A, Canale A, et al. (2022) Transoral Approach to Parotid Tumors: A Review of the Literature. Curr Oncol 29(12): 9416-9427.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?