Endoscopic-Assisted Excision of an Extensive Inverted Papilloma (Krouse Stage IV) through Lateral Rhinotomy Approach: A Case Report
Inverted papilloma is a benign epithelial growth arising from the Schneiderian mucosa with a tendency to grow into the underlying stroma. The etiology remains obscure but its tendency for an association with malignancy makes it an important entity important for the surgeon. We present a case report of an extensive inverted papilloma (Krouse stage IV). The tumour involved entire right side nasal cavity extending to the vestibule, extended to the orbit and also intracranially (though extradural) through the frontal and ethmoid sinuses. This extensive tumour was removed by a combined (lateral rhinotomy plus endoscopic) approach and obviated the need for external approach to frontal sinus as well as extended lateral rhinotomy. Thus, even for extensive tumours using the endoscope as an adjunct aids in complete tumour removal and prevents additional morbidity to the patient.
Introduction
Inverted papilloma was first described by Ward in 1854 [1]. It is widely known to arise from the Schneiderian mucosa of the lateral nasal wall and accounts for 0.5% to 4% of primary nasal tumors [2].
The etiology of inverted papilloma remains controversial; with some pointing to it being viral while others completely rejecting it as a true papilloma outright and marking it as an inflammatory polyp [3, 4].
HPV has been implicated by many authors, while others point to EBV [5, 6, 7, 8]. Irrespective, the cause of concern here still remains its ability to recur as well as its association with carcinoma. Malignancy has been reported in 5-15% of cases [9]. Nygren et al in his large study of 88 cases, showed a malignant transformation rate of 8.9% [10]. Mirza et al in their 20 -year study found a rate of 11%, while in their literature review; they found 7.1% cases had a synchronous malignancy [11]. Thus, it is imperative to achieve complete excision of this tumor as well as a need for regular follow-up is requisite for long tumor surveillance.
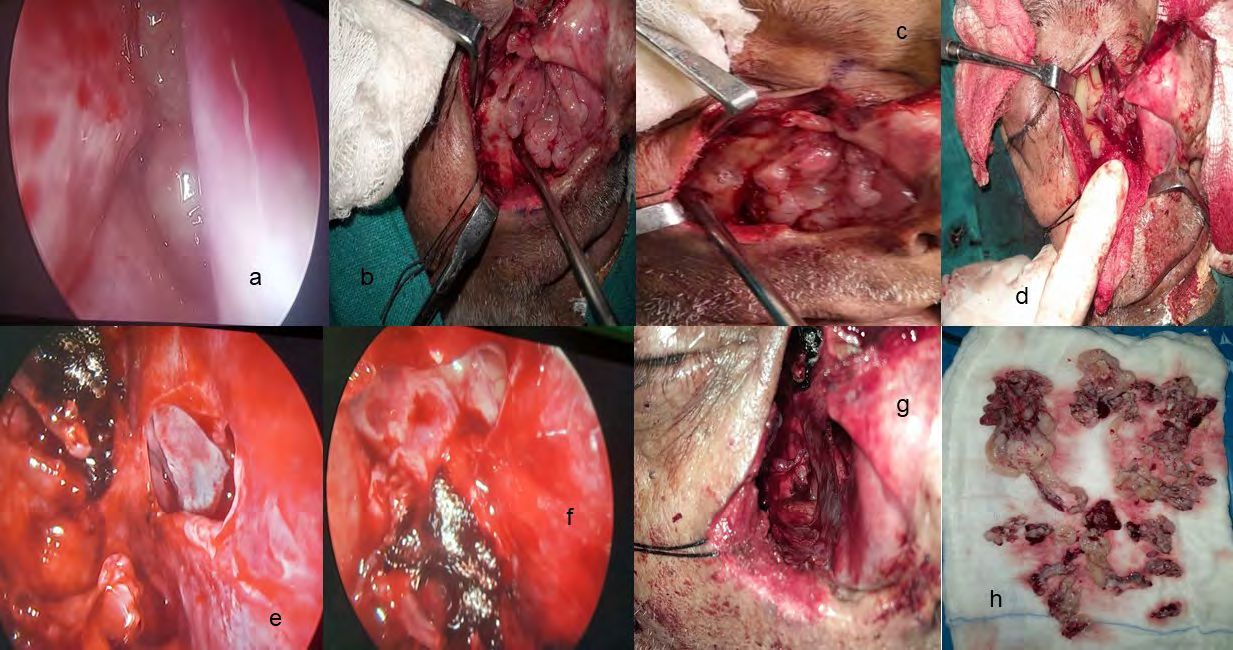
The first step to reach a probable clinical diagnosis is taking a complete history and a thorough examination. In addition, clinical examination can also help reach a differential diagnosis. Imaging helps to further clarify the diagnosis with some authorities advocating CT (Computed Tomography) while others MRI (Magnetic resonance Imaging). CT helps to identify bony confines of the tumour: more aggressive disease process produces more bony alterations; perforations instead of thinning may be an indication of malignancy. Evaluation of skull base and orbit is important. MRI can identify the soft tissue extent. The sinuses may have retained secretions or may be filled with mass: this may change the approach to the tumour [12]. Confirmation, however, is by means of a biopsy only. Staging has been proposed by Krouse and Han et al to better the surgical results [9, 13, 14, 15]. Krouse staging is widely followed for inverted papilloma. It has four categories: T1 to T4 starting with the confinement of tumour to nasal cavity without an intrasinus extension (T1), involvement of osteomeatal complex, ethmoid sinus, or medial wall of maxillary sinus (T2), extension to sphenoid, frontal or any other wall of maxillary sinus (T3) and finally involvement of contiguous structures like orbit, pterygomaxillary space or having an intracranial extension (T4) [13]. Different approaches have been used for its resection, and traditionally, A 72-year-old patient came with complaints of right nasal obstruction for 3 years. The nasal obstruction was gradual in onset and slowly progressive, with no diurnal or seasonal variation. There was no history of epistaxis, facial numbness, headache, or facial fullness. Nasal endoscopy with 0-degree revealed a huge multilobulated mass in the right nasal cavity extending up to the vestibule, which was firm in consistency and irregular. Even inferior turbinate was obscured entirely by the mass. In the left nasal cavity, the mass was seen just anterior to the axilla of the middle turbinate coming from the right nasal cavity via a septal perforation (Figure 1). Mass was also extending to the left nasal cavity via the nasopharynx and left choana. Some part of the mass was seen hanging in the oropharynx.
open approaches have provided excellent results [16]. Lateral rhinotomy or its extensions and midfacial degloving provide a good route for medial maxillectomy or Denker or total maxillectomy to remove the tumor in its entirety. However, the endoscope has now greatly influenced the surgical technique, as it proves to be a great adjunct to open surgery; and has totally substituted it in the majority of cases. Here we present the case of a 72-year-old male who came with a right nasal mass, was investigated and diagnosed as a case of inverted papilloma (Krouse Stage IV) and subsequently treated.
Case Report
A Contrast-enhanced CT (CECT) was done and it displayed a large infiltrative soft tissue lesion involving the right nasal cavity, right ethmoid and bilateral frontal sinuses with mild to moderate heterogenous enhancement on contrast. Small erosion was present in the posterior wall of the left frontal sinus. Gross expansion of the right ethmoid and right frontal sinus was seen with associated marked thinning and erosion of their walls. A small erosion of the roof of the ethmoid was seen with an extension of mass intracranially but extradurally (Figure 2).
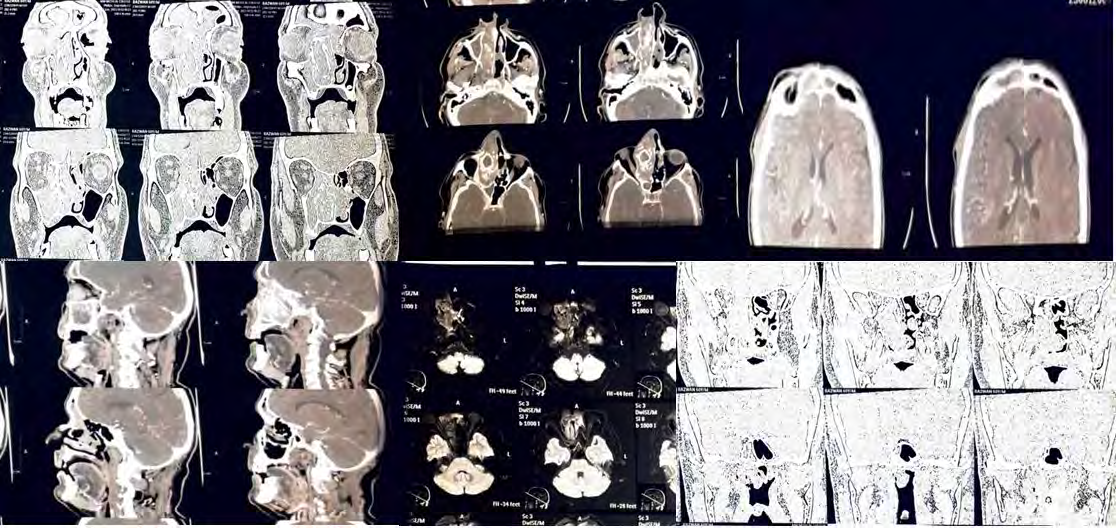
Figure 2: NCCT –PNS (Non-Contrast Computed Tomography- Paranasal Sinus) Revealed Poorly Defined Infiltrative Soft Tissue Sinonasal Mass Involving the Right Ethmoid Air Cells, Bilateral Frontal Sinuses(R>L), with Extension into the Right Nasal Cavity with Intra-Orbital (Right Medial Extra Conal Space) and? Intracranial Extension and Bony Destruction of the Right Frontal Sinus, Right Lamina Papyracea, Medial Wall Right Maxillary Sinus, Septum.
Imaging) revealed a large sinonasal mass centered in the right nasal cavity with bony erosions and extensions (Figure 3).
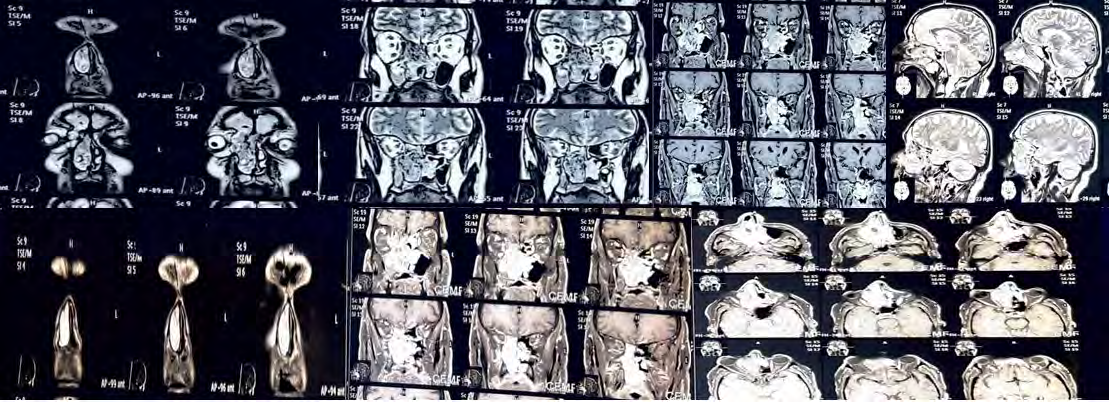
Figure 3: CE-MRI Brain, Orbit And PNS Revealed a Large Heterogenous Sinonasal Mass Centered in the Right Nasal Cavity with Involvement of Bilateral Ethmoid Cells with Lateral Extension in the Right Maxillary Sinus and Superior Extension into the Bilateral Frontal Sinus. The Mass Appeared Isointense on T1W and Heterogenously Hyperintense on T2W FAT Sat Images with T2W Hypointense Areas Giving a Cerebriform Appearance. Multiple Foci of Calcifications were seen within it. Left Lateral Displacement and Erosion of Septum, Destruction of Right MT & IT, Uncinate, and Medial Wall of the Maxillary Sinus was Noticed. Superolaterally, it was causing the Destruction of the Right Lamina Papyracea and the Extension of Mass into Medial Extraconal Space of the Right Orbit Displacing the Globe Laterally. It was also Causing Erosion of The Anterior and Posterior Walls of the Frontal Sinus (Right), However, no Gross Intracranial Extension was Seen. Erosion of the Anterior Wall of the Sphenoid Sinus (Right) and Extension into Right Pterygopalatine Fossa with Mild Widening was also Reported.
A biopsy of the mass was taken and it revealed the tissue bits lined predominantly by stratified squamous epithelium, transitional epithelium and focally by respiratory epithelium. Focal downward infiltration of nests and cystic spaces of squamous and transitional epithelium exhibiting basal mitosis, neutrophilic transmigration and minimal atypia was seen and all findings were consistent with characteristics of sinonasal papilloma, inverted type. A preoperative diagnosis was made to be that of inverted papilloma- Krouse Stage IV, as there was extradural extension of tumour.
The patient was planned for excision of inverted papilloma and an appropriate informed and written consent was taken. The extent of the tumour necessitated the open approach, as the bulk of the tumour lay in the superior part of the nasal cavity, extending to the orbit and also frontal sinus. Thus, adopting medial maxillectomy via lateral rhinotomy approach, with the option to extend the Moure’s incision superiorly to the forehead (extended lateral rhinotomy) or as lynch extension or conversion to a Weber Fergusson incision with supraciliary or subciliary extension as and when needed. Due to the extension of the tumor into the frontal sinus, an external approach to the frontal sinus was planned by extended lateral rhinotomy and osteoplastic flap for which an x-ray impression of frontal sinus boundaries was made using X-ray nose-PNS Caldwell view. The patient was taken up under general anesthesia and lateral rhinotomy was done. Intraoperatively, the mass was seen to erode the anterior maxillary wall (about 0.5cm defect) and protrude out through it. Laterally, the mass was seen extending into the orbit (about 2 cm defect) with erosion of lamina papyracea but the orbital periosteum was intact. The mass was also seen extending into the left frontal sinuses after erosion of the inter-sinus septum from the right frontal sinus. The nasal septum was also found to be eroded superiorly just anterior to middle turbinate (about 1 cm defect). The tumor was attached to anterior ethmoid cells. After this mass in the nasal cavity was removed along with the medial maxillectomy specimen. The ethmoidal labyrinth was also removed along with the middle turbinate (Figure 1b-1h). The endoscope was introduced, and the removal of the frontal sinus portion of the mass was attempted. The mass came out in a single piece along with purulent discharge from bilateral frontal sinuses; the intracranial portion had come out simultaneously as well. The need for an external approach was thus saved. A small defect was noted about 0.5 cm in the roof of the ethmoid along with exposure of the dura. The lacrimal sac was opened, its medial wall removed and a Crawford stent placed. Remnant of the mass was checked for with 0°, 30° and 70°endoscopes. The defect on the ethmoidal roof was repaired with a piece of temporalis fascia and surgicel. The sphenoid opening was enlarged and examined and found to be free from tumor mass. The resultant cavity was washed, and packed and suturing of the external incision was done. The pack was removed on the third postoperative day. The patient was discharged on the seventh post-operative day and routine follow-up of the patient after 1 year revealed a healthy cavity with no obvious recurrence, no diplopia or epiphora. The patient had nasal crusting till about 3 months which was treated by usual saline nasal douchings. The biopsy of the resected mass was consistent with an inverted papilloma and with no evidence of malignancy. Out of various sinonasal papillomas, such as exophytic and oncocytic; inverted papilloma has a characteristic and distinctive pattern of growth microscopically: it grows inwards proliferating below the basement membrane into the stroma (Figure 4) unlike other probabilities like squamous papilloma where further tests may be mandated for a definite diagnosis.
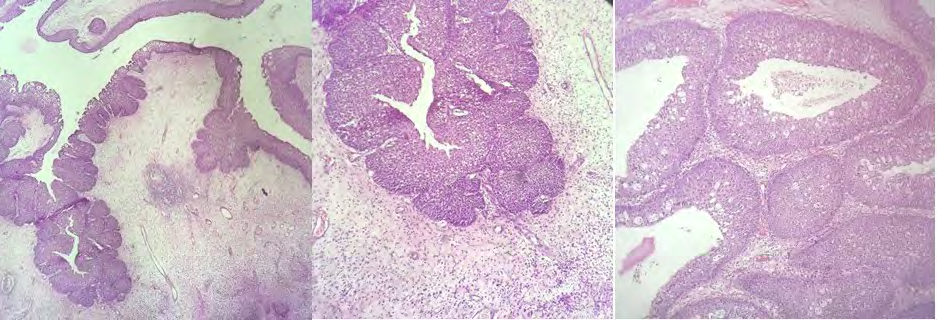
Figure 4: Histopathology of the Resected Specimen. A: Prominent Downward Endophytic Growth of Round to Elongated Interconnected Epithelial Nests with Smooth Outer Contour (H&E, X10); B: Invaginating Nests of Hyperplastic Epithelium, Respiratory Type with Focal Squamous Metaplasia (H&E,X40); C: Nests with Neutrophilic Microabscesses. Surrounding Stroma Shows Mild Edema with Chronic Inflammation (H&E, X10).
Discussion
Although endoscopic excision is now considered the gold standard for the removal of inverted papillomas, it is necessary that treatment be tailored for individual cases [17, 18]. The most important factor that the surgeon keeps in mind while planning an approach is to minimize recurrence. The recurrence rates have been quoted from 10 to 20% [17, 19] with endoscopic approaches showing a lower recurrence rate as compared to open approach [20, 21, 22]. Older studies have reported higher recurrence than newer studies probably due to better equipment, technique as well an array of endoscopes available to much experienced surgeons [23]. The experience of the surgeon has also been touted to decrease post-operative recurrence. In our case, having removed the mass along with the medial maxillectomy specimen, only the frontal portion remained which was subsequently removed via endoscope. The endoscope was also used to check the completeness of excision and to open the sphenoid sinus and clear it of retained secretions. Thus, the bulk of the tumor was removed by an open approach, and the more intricate work was done using an endoscope. This allowed us to comprehensively check for any residual tumor and also saved an open approach to the frontal sinus.
The attachment of inverted papilloma is crucial in that it needs to be completely removed and the underlying bone should be drilled. Imaging modalities, both CT and gadolinium enhanced MRI help to provide a clearer picture to identify this, which still may be difficult pre-operatively. Also, the frontal sinus, being an anatomically complex area can be more challenging. Not only is the anatomy but the functionality too is more intricate. It not only provides aesthetic appease to the forehead but also is in close relation to the frontal lobe of the brain. Thus, extension of the tumour to frontal sinus, makes for a challenging surgical procedure.
The highest numbers of recurrence cases are noted in the first 2-3 years but there have been reports of later recurrences too [24]. Still, a life-long follow-up is necessary for disease surveillance. Apart from recurrence, there are other minor post-operative morbidities like persistent pain, epiphora, nasal crusting, alar deformity, hypertrophied scar, hypoesthesia of the cheek and hypoesthesia of teeth. In our patient, there was nasal crusting and temporary hypoesthesia of the cheek. The patient was advised saline nasal douching and saline nasal drops postoperatively which decreased nasal crusting. Apart from this, the patient had an uneventful post-operative period. This case report stresses the importance of angled endoscopes for a comprehensive removal of tumour even if an open approach is necessary for its removal.
Conclusion
The incidence of recurrence has been attributed to an inability on the part of the surgeon to discern the attachment of inverted papilloma and thus the recurrence is actually residual disease in many cases. The attachment-oriented resection is considered to lessen the recurrence [25, 26]. In the present case, the extension of the disease warranted an open approach. The disease not only extended to the opposite nasal cavity via a septal perforation, but also to the orbit via a 2cm defect in the lamina papyracea, to the cheek via a small defect in the anterior maxillary wall, to both the frontal sinuses, and to the extradural space: Krouse stage IV. We opted for lateral rhinotomy and with the aid of various angled endoscope could remove the tumour in its entirety without the need for further extensions. Thus, endoscope aided open approach has proved to be a boon in such cases, and diminished the need for more aggressive surgery like an osteoplastic flap or a bicoronal incision to approach the frontal sinus.
References
-
Ward N (1854) A mirror of the practice of medicine and surgery in the hospitals of London: London Hospital: Follicular tumour involving the nasal bones, nasal processes of superior maxillary bone, and the septum of the nose; removal; death from pneumonia; autopsy. Lancet 64(1632): 480-482.
-
Durucu C, Baglam T, Karatas E, Mumbuc S, Kanlikama M (2009) Surgical treatment of inverted papilloma. J Craniofac Surg 20(6): 1985-1988.
-
Michaels L, Young M (1995) Histogenesis of papillomas of the nose and paranasal sinuses. Arch Pathol Lab Med 119(9): 821-826.
-
Beck JC, McClatchey KD, Lesperance MM, Esclamado RM, Carey TE (1995) Human papillomavirus types important in progression of inverted papilloma. Otolaryngol Head Neck Surg 113(5): 558-563.
-
Cheung FMF, Lau TWS, Cheung LKN, Li ASM, Chow SK, et al. (2010) Schneiderian papillomas and carcinomas: a retrospective study with special reference to p53 and p16 tumor suppressor gene expression and association with HPV. Ear Nose Throat J 89(10): E5-E12.
-
Hwang CS, Yang HS, Hong MK (1998) Detection of human papillomavirus (HPV) in sinonasal inverted papillomas using polymerase chain reaction (PCR). Am J Rhinol 12(5): 363-366.
-
Franzmann MB, Buchwald C, Jacobsen GK, Lindeberg H (1998) Expression of p53 in normal nasal mucosa and in sinonasalpapillomas with and without associated carcinoma and the relation to human papillomavirus (HPV). Cancer Lett 128(2): 161-164.
-
Sham CL, To KF, Chan PKS, Lee DLY, Tong MCF, et al. (2012) Prevalence of human papillomavirus, Epstein- Barr virus, p21, and p53 expression in sinonasal inverted papilloma, nasal polyp, and hypertrophied turbinate in Hong Kong patients. Head Neck 34(4): 520-533.
-
Han JK, Smith TL, Loehrl T, Toohill RJ, Smith MM (2001) An evolution in the management of sinonasal inverted papilloma. Laryngoscope 111(8): 1395-1400.
-
Nygren A, Kiss KV, Buchwald C, Bilde A (2016) Rate of recurrence and malignant transformation in 88 cases with inverted papilloma between 1998-2008. Acta Otolaryngol 136(3): 333-336.
-
Mirza S, Bradley PJ, Acharya A, Stacey M, Jones NS (2007) Sinonasal inverted papillomas: recurrence, and synchronous and metachronous malignancy. J Laryngol Otol 121(9): 857-864.
-
Yousem DM, Fellows DW, Kennedy DW, Bolger WE, Kashima H, et al. (1992) Inverted papilloma: evaluation with MR imaging. Radiology 185(2): 501-505.
-
Krouse JH (2000) Development of a staging system for inverted papilloma. Laryngoscope 110(6): 965-968.
-
Cannady SB, Batra PS, Sautter NB, Roh HJ, Citardi MJ (2007) New staging system for sinonasal inverted papilloma in the endoscopic era. Laryngoscope 117(7): 1283-1287.
-
Krouse JH (2001) Endoscopic treatment of inverted papilloma: safety and efficacy. Am J Otolaryngol 22(2): 87-99.
-
Vrabec DP (1994) The inverted schneiderian papilloma: A 25 year study. Laryngoscope 104(5): 582-605.
-
Attlmayr B, Derbyshire SG, Kasbekar AV, Swift AC (2017) Management of inverted papilloma: Review. J Laryngol Otol 131(4): 284-289.
-
Kim JS, Kwon SH (2017) Recurrence of sinonasal inverted papilloma following surgical approach: A meta-analysis. Laryngoscope 127(1): 52-58.
-
Busquets JM, Hwang PH (2006) Endoscopic resection of sinonasal inverted papilloma: A meta-analysis. Otolaryngol Head Neck Surg 134(3): 476-482.
-
Kamel RH, Fattah AFA, Awad AG (2014) Transnasal endoscopic medial maxillectomy in recurrent maxillary sinus inverted papilloma. Rhinology 52(4): 381-385.
-
Pasquini E, Sciarretta V, Farneti G, Modugno GC, Ceroni AR (2004) Inverted papilloma: Report of 89 cases. Am J Otolaryngol 25(3): 178-185.
-
Lawson W, Patel ZM (2009) The evolution of management for inverted papilloma: An analysis of 200 cases. Otolaryngol Head Neck Surg 140(3): 330-335.
-
Heathcote KJ, Nair SB (2009) The impact of modern techniques on the recurrence rate of inverted papilloma treated by endonasal surgery. Rhinology 47(4): 339-344.
-
Jiang XD, Dong QZ, Li SL, Huang TQ, Zhang NK (2017) Endoscopic surgery of a sinonasal inverted papilloma: Surgical strategy, follow-up, and recurrence rate. Am J Rhinol Allergy 31(1): 51-55.
-
Healy DY, Chhabra N, Metson R, Holbrook EH, Gray ST (2016) Surgical risk factors for recurrence of inverted papilloma. Laryngoscope 126(4): 796-801.
-
Landsberg R, Cavel O, Segev Y, Khafif A, Fliss DM (2008) Attachment-oriented endoscopic surgical strategy for sinonasal inverted papilloma. Am J Rhinol 22(6): 629- 634.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?