Attic Cholesteatoma and High Riding Jugular Bulb: a Rare Cause of Conductive Hearing Loss
The jugular bulb corresponds to the most cranial part of the internal jugular vein and is intimately related to the middle ear forming its floor or fundus tympani. In the embryological development, different anatomical alterations of this region can be manifested, such as a high riding and dehiscent jugular bulb, a protruding bulb with preservation of its bony structure or jugular bulb diverticulum. This anatomical variant is asymptomatic in most cases. However, depending on the size of the jugular height and its relationships, it could generate otologic symptoms such as tinnitus, fullness and, more rarely, conductive hearing loss. We report a case of a pathological association consisting of an attic cholesteatoma and a high riding jugular bulb in the left ear of a female patient who consulted for conductive hearing loss, aural fullness and pulsatile tinnitus. In this case, endoscopic intervention of the attic cholesteatoma was decided, taking care to avoid inadvertently injuring the venous gulf. Thus, the removal of the incus, the head of the malleus and the cholesteatoma was performed in a transcanal fashion. Subsequently, tragus cartilage was placed to repair the attic and over the stapes head to improve sound transmission.
Introduction
The jugular bulb corresponds to the most superior part of the jugular vein and is located in the jugular foramen. Anatomically, the upper part of the jugular bulb is in intimate relationship with the inferior wall of the middle ear (fundus tympani). In rare cases, this may extend superiorly and raise the floor of the hypothympanum and become involved with the middle ear, contacting structures such as the round window, the promontory or the incudo-stapedial joint.
This scenario is defined as a high-riding jugular bulb, and it is considered a common venous anomaly with an incidence of 2 to 7% of the temporal bones and a prevalence of 5 times higher in patients with associated audiologic symptoms. It can present as two distinct entities: through a dehiscence in the sigmoid plate (middle ear floor) generating a protrusion into the middle ear through this defect or as a congenital variant that associates the high riding bulb with an integrated sigmoid plate. This situation can generate massive hemorrhage in otologic surgeries if not recognized by the surgeon [1, 2, 3, 4]. The main difference between a high- riding jugular bulb and a dehiscent jugular bulb is the lack of bony plate in the latter one. This condition needs to be clarified with the use of CT scan before the surgery in order to avoid bleeding.
Page reports, in 1914, the first case of high riding jugular bulb in a 10 month old child when a large hemorrhage was observed following myringotomy for acute otitis media which at the time could be controlled with plugging of the external auditory canal [1].
If the developmental relationship between the temporal bone and the surrounding venous sinuses is analyzed from an embryological point of view, the transverse and sigmoid sinuses appear in the eighth week of gestation, and by the tenth week of gestation they are almost fully developed.
The ossification progresses from the squamous part of the temporal bone to the zygomatic process in the 8th week of gestation, and the ossification of the tympanic cavity appears between 9 and 10 weeks of gestation. The skull base ossifies rapidly at the end of the month. This means that the vascular system is formed before the complete bony case is achieved. Consequently, an abnormality in bone formation does not generate an abnormality in blood vessel development, but an abnormality in blood circulation may occur before bone formation. The anatomical reason behind the dominance of the sigmoid sinus or jugular gulf on the right side compared to the left is explained by the venous vascularization that reaches the right atrium.
The right internal jugular vein, upon joining the subclavian vein, forms the angle of Pirogoff, and continues as the brachiocephalic venous trunk to form the superior vena cava together with the left brachiocephalic venous trunk. The latter has a more oblique direction and a longer course, causing the atrial systoles and the small retrograde flow to have a longer course and therefore less venous stasis in the region of the left jugular bulb. Thus, on the right side, due to venous transmission and blood remora, the homolateral bulb or sinus is usually wider.
Despite the fact that a high riding jugular bulb can produce conductive hearing loss, it is also associated with the appearance of an attical cholesteatoma. The latter one develops due to a blockage of the tympanic isthmus or the Von Tröltsch pouch which aerates the epitympanum and Prussak’s space respectively. In cases of a tympanic isthmus blockage, the positive air pressure coming from the Eustachian tube can not reach the epitympanic space giving place to a condition called selective epitympanic dysventilation syndrome. This can be clinically addressed by the presence of attic retraction pockets with or without epidermic cells.
Case Report
We present a 36-year-old female patient with fullness, pulsatile tinnitus and hearing loss of the left ear.
Otomicroscopy showed accumulation of detritus in the atical region and a noticeable bluish stain due to transparency of the eardrum occupying almost all the middle ear cleft. Tuning fork tests were consistent with a conductive pattern. The patient had no active suppuration, nor history of repeated otitis. The right ear was without relevant pathology .
The patient’s study was complemented with pure tone audiometry, speech audiometry and tympanoimpedance audiometry. A high-resolution cone beam tomography of both petrous bones was also requested.
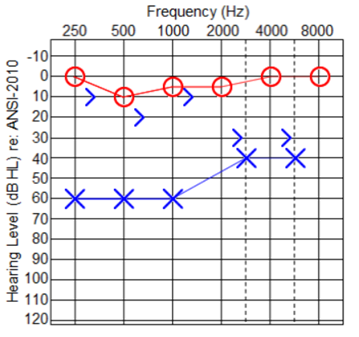
The audiometry showed conductive hearing loss with a maximum air bone gap (60dB) in low and medium frequencies, a logoaudiometry displaced to the right with 100% discrimination, tympanometric curves of affected ear type B and healthy ear A, as shown in Figure 1.
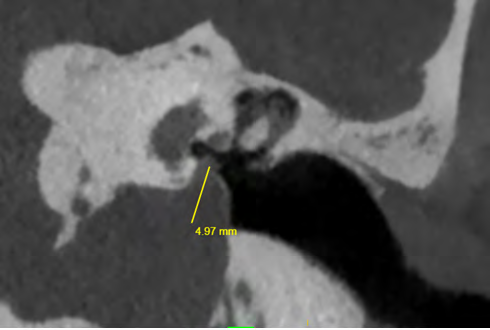
The CT scan showed an increase in the size of the jugular bulb in cephalic direction, protruding in great proportion to the middle ear, approximately 4.97mm of invasion. An aticoantral occupation of soft tissue density with signs of lateral wall erosion and part of the body of the incus was also evident, as shown in Figure 2.
Otologic surgery was proposed to the patient due to the presence of cholesteatomatous tissue in an anatomically unfavorable ear because of the presence of the high jugular bulb. In this sense, the time of evolution of the disease, which was relatively short, had to be optimized in order to avoid progression of the tumor size and thus avoid a more aggressive approach that could damage the venous structure.
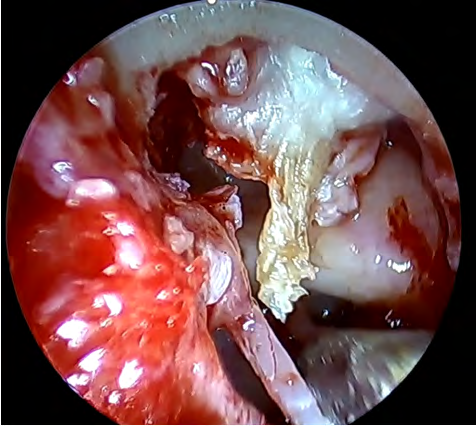
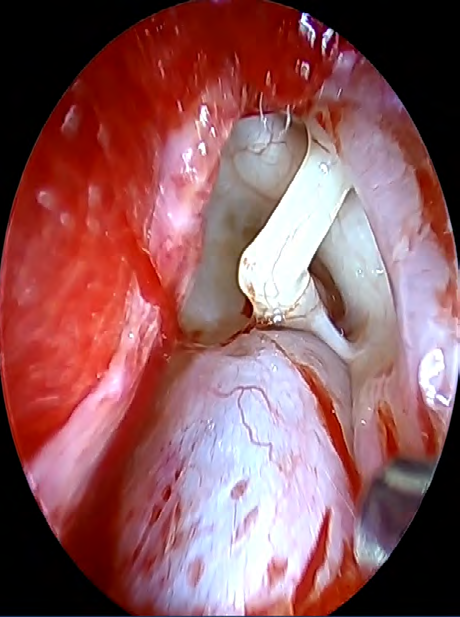
A transcanal endoscopic approach was performed, the tympanomeatal flap was raised, making circumferential and radial incisions. The tympanic annulus was elevated to expose the middle ear cavity. The presence of a high jugular bulb (Figure 3), in contact with the incudostapedial joint was found, which was later disconnected to avoid excessive transmission into the inner ear. Upon removal of the incus, erosion of the lateral aspect of the body was observed. Afterwards, with a diamond burr, part of the remanent scutum was removed. This revealed the presence of a cholesteatoma sac which was followed to the aditus ad antrum (Figure 4). The head of the malleus was removed to verify the indemnity of the anterior epitympanic space. Subsequently, tragus cartilage was obtained and used to reconstruct the scutum. Another small cartilage was placed in the capitellum of the stapes to improve transmission. The authors decided not to put any type of partial ossicular replacement prosthesis (PORP) because of the risk of extrusion and possibility of erosion of the bony plate of the jugular bulb by contact.
The endoscopic approach was preferred since it generates less surgical trauma compared to the retroauricular approach, shorter surgical and recovery times and a clearly better exposure of the middle ear structures that provide the surgeon and the rest of the surgical team (residents, fellows, scrubs) a greater view and therefore more delicate movements.
The patient was discharged the same day as the intervention with a local dressing with sterile gauze. After seven days, the gauze was removed and ear drops with ofloxacin were prescribed. After a month, the tympanic membrane was completely healed with a subjective improvement in the hearing and a positive Rinne test at 256 and 512 Hz.
Surgical video can be seen at: https://www.youtube.com/watch?v=NBcm9TgIVww
Discussion
The jugular bulb usually has a thin bony covering. Between 6-36% of the bulb is described as high and procurrent, and dehiscent as such 3.9%. When these premises are present in concomitance, it generates tinnitus in up to 50% of cases and an incidence of conductive hearing loss of 3%. Dehiscence and procidence of the jugular bulb do not restrict surgery, however, great care must be taken not to injure noble structures [5, 6, 7].
Nakano Y, et al. [2] report two cases of high jugular bulb and attic cholesteatoma. Both patients had a sclerosus right mastoid and a high jugular bulb with an anterior anatomic situation. The authors propose that, due to the presence of the high bulb, the epitympanic ventilation routes would become ineffective generating a hypoplasia of the attic mainly of its lateral wall, thus creating retraction pockets with squamous content that will eventually become a cholesteatoma.
Among the mechanisms proposed to generate conductive hearing loss, Koo, et al. [3] highlight: contact of the jugular bulb with the tympanic membrane generating greater impedance, contact with the incudo-stapedial joint, obliteration of the round window and a blockage of the vestibular aqueduct in the case of a possible mixed hearing loss.
Takata Y, et al. [6] describes the first case of the association between high jugular bulb, dehiscent and cholesteatoma treated surgically under endoscopic vision with the underwater technique. The middle ear is completely filled with saline perfusion, which is useful not only to have a clear and visible surgical field, but also to avoid possible aeroembolism secondary to unexpected jugular gulf injury.
Conclusion
This case required a difficult decision that had to be made together with the patient, since the risk of massive bleeding in the middle ear was high, but on the other hand, the presence of cholesteatomatous tissue in the attic represented a potential problem in the future.
Regarding the use of an endoscope, this was preferred because of the magnification and clarity of the image it provides, thus avoiding the blind spaces that are typical of microscopic use.
The association of high jugular gulf and concomitant cholesteatoma is rarely reported in the literature despite being relatively conventional pathologies.
Decision making should be personalized to minimize risks and achieve functional results.
References
-
Page JR (1914) XIX. A Case of Probable Injury to the Jugular Bulb following Myringotomy in an Infant Ten Months Old. Annals of Otology, Rhinology & Laryngology 23(1): 161-163.
-
Nakano Y, Igarashi Y (1999) High Jugular Bulb with Attic Cholesteatoma. Practica Oto-Rhino-Laryngologica 92(12): 1305-1309.
-
Overton SB, Ritter FN (1973) A High Placed Jugular Bulb In The Middle Ear: A Clinical And Temporal Bone Study. The Laryngoscope 83(12): 1986-1991.
-
Prasad KC, Basava CH, Gopinathan PN (2018) A Revisit to High Jugular Bulb: A Newer Clinical Grading. Indian J Otolaryngol Head Neck Surg 70: 527-530.
-
Koo YH, Lee JY, Lee JD, Hong HS (2018) Dehiscent high- riding jugular bulb presenting as conductive hearing loss: A case report. Medicine (Baltimore).
-
Takata Y, Anzai T, Hara S, Okada H, Matsumoto F, et al. (2021) Cholesteatoma Surgery With a Dehiscent High Jugular Bulb Treated With Surgery Assisted With Underwater Endoscopy: A Case Report. Ear, Nose & Throat Journal.
-
Barr JG, Singh PK (2016) A rare cause of conductive hearing loss: High lateralized jugular bulb with bony dehiscence. Ear Nose Throat J 95(6): 227-229.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?