Epidemiological Profile and Diagnostic Aspects of Pediatric Ear, Nose and Throat (ENT) Pathologies at the Renaissance University Hospital Center in N’Djamena, Chad
Background: Pediatric ENT pathologies form an important part that encompasses a wide range of medical conditions, primarily infections, which pose as a significant public health challenge. In developing countries like Chad, the absence of precise epidemiological data hampers the development of effective prevention and treatment strategies. The objective of this study is to describe the epidemiological profile and diagnostic aspects of pediatric ENT pathologies among patients at the Renaissance University Hospital Center in N’Djamena, Chad. Methods: This prospective, cross-sectional study which was conducted from January 2021 to December 2022. It included all children aged 0 to 17 years, who were consulted in the ENT department of the Renaissance University Hospital Center, whose parents had given their consent. Various ENT examinations, including audiometry, radiology and laboratory tests were performed according to patients’ symptoms. Results: This study had a prevalence of 25.1% of ENT pathologies among children, with a slight male predominance and a sex ratio of 1.3. The most affected children were aged 0 to 6 years, presenting symptoms such as hearing loss, otalgia, cough, and rhinorrhea. Common conditions included nasopharyngitis, tonsillitis, and various forms of otitis. Infections and inflammations accounted for 78.2% of cases. The ear was affected in 46.8% of cases, followed by the pharynx in 33.8% of cases. The peaks in the pathologies were observed in March, September and October. Children with atopic diseases were more susceptible to these conditions. Conclusion: The study highlights a high prevalence of ENT pathologies among children, with infectious and inflammatory conditions being the most common. Their occurrence is influenced by immunological, climatic, and social factors. The findings underscore the importance of prevention and appropriate management, considering local specificities.
Taoussi AA¹*, Babou F¹, Attimer KA² and Yusra AA³
¹Department of Otolaryngology (ENT)/Head & Neck Surgery, Renaissance University Hospital Center, Chad ²Pediatrics Department, Mother and Child University Hospital Center, Chad ³Department of Internal Medicine, Renaissance University Hospital Center, Chad
Abbreviations
ENT: Ear, Nose and Throat; VRA: Visual Reinforcement Audiometry; CPA: Conditioned Play Audiometry: SPSS: Statistical Package for the Social Science.
Introduction
Pediatric otorhinolaryngological pathologies encompasses a wide range of conditions affecting children’s ears, nose, and throat. These conditions can be infectious, inflammatory, traumatic, tumorous or congenital. Among these, ENT infections are particularly prominent in pediatric literature [1, 2].
Infectious ENT diseases in children represent a significant public health problem. They cover a broad spectrum of pathologies, ranging from mild or self-resolving disorders to severe or potentially fatal diseases, featuring complications and morbidity. These conditions can impair fundamental physiological functions such as hearing, smelling, tasting, phonation and respiration and may potentially lead to permanent disabilities [3]. Common diseases include acute otitis media, sinusitis, tonsillitis and nasopharyngitis.
The pediatric population in developing countries are severely affected by various ENT disorders, largely due to the widespread of poverty. In Africa, pediatric ENT pathologies account for more than 25% of the overall ENT conditions [4, 5]. They are often dominated by infections and trauma, although the nature of these conditions varies from one country to another. Acute and chronic otitis media, otitis externa, tonsillitis and foreign bodies are particularly common [4, 5, 6, 7]. These conditions can have significant consequences on children’s health and development, making their diagnosis and treatment essential.
Pediatric ENT pathologies represent a crucial medical field, particularly in developing countries like Chad, where epidemiological data are very limited. The lack of epidemiological data on pediatric ENT pathologies in Chad poses as a major challenge for healthcare professionals. Without a clear understanding of the prevalence and characteristics of these conditions, it is difficult to develop effective prevention and treatment strategies.
This study aims to describe the epidemiological and diagnostic aspects of pediatric ENT pathologies at the Renaissance University Hospital Center in Chad. By providing precise and current data on these pathologies, this research can guide public health policies and clinical interventions. Additionally, it will help raise awareness among health authorities and local communities about the importance of these conditions and the need for adequate management.
Materials and Methods
This prospective, cross-sectional study was conducted from January 1, 2021, to December 31, 2022, at the ENT and Head and Neck Surgery Department of the Renaissance University Hospital Center in Chad. The study included patients aged 0 to 17 years, regardless of gender, whose parents had given their consent. Exclusion criteria were patients aged 18 and over, children without parental consent, and patients with significant comorbidities referred for consultation.
Data were collected using a pre-established survey form, which included results from clinical, audiological, biological and radiological examinations. The variables studied encompassed sociodemographic data (age, gender, residence), medical and surgical history, clinical variables (reason for consultation, ENT and general examinations), audiological data (pure tone and speech audiometry, tympanometry, specific hearing tests for children under 6 years), results of biological and radiological examinations, and diagnosis (positive, etiological, and topographical).
Information was gathered through direct observation of patients during consultations. Each patient, accompanied by at least one parent, underwent a thorough interview to identify the reason for consultation, onset of symptoms, medical and surgical history, and tobacco exposure, followed by ENT and general examinations.
All patients underwent a comprehensive examination, including otoscopy, anterior rhinoscopy, and inspection of the oral and oropharyngeal cavities, as well as the skin of the neck and face. Nasofibroscopy was performed for children with upper respiratory disorders or dysphonia. Depending on their age, patients with hearing loss underwent visual reinforcement audiometry (VRA), conditioned play audiometry (CPA), or conventional tone and speech audiometry, along with tympanometry if there was no tympanic perforation. In cases of otorrhea, a sample was taken for cytobacteriological examination. Radiography of the neck and/or thorax were conducted if foreign body inhalation was suspected. A computed tomography scan was requested for congenital deafness, suspected chronic middle ear cholesteatomas or certain cervicofacial tumors.
Data analysis was performed using SPSS version 26.0. Qualitative data were presented as percentages, while quantitative variables were summarized as means with standard deviations or as medians with extreme values. The chi-square test was used to explore associations between atopic diseases, tobacco exposure and the different regions of the ENT sphere affected. Additionally, it was also used to explore between etiological and topographical diagnosis and sex, and between etiological diagnosis and the regions affected. A p-value of less than 0.05 was considered statistically significant.
The study received approval from the management of the Renaissance University Hospital Center and the Dean of the Faculty of Human Health Sciences in the University of N’Djamena. A verbal consent was obtained from all parents of the patients for participation in this study and publication of the data. The study adhered to the ethical principles outlined in the 2013 Declaration of Helsinki.
Results
During the study period at the Renaissance University Hospital Center in N’Djamena, Chad, 2,590 patients attended ENT consultations of which 650 were children, representing a prevalence of 25.1%. Among these children, 363 were males (56%) and 286 were females (44%), resulting in a sex ratio of 1.3.
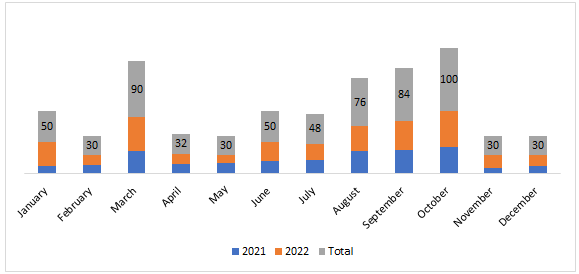
The children’s ages ranged from 8 days to 17 years, with a median age of 6 years and an average age of 7.3 ± 5.1 years. The age distribution was as follows; 282 children (43.4%) were between 0 to 6 years old, 222 children (34.1%) were between 6 to 12 years old, and 146 children (22.5%) were between 12 and 18 years old. A significant majority, 96.6% (628 cases) of the children lived in urban areas. Additionally, 11.1% (72 cases) had a history of atopy, and 4% (26 cases) were exposed to tobacco. The monthly distribution of cases (Figure 1) showed peaks in October (100 cases), March (90 cases), and September (84 cases).
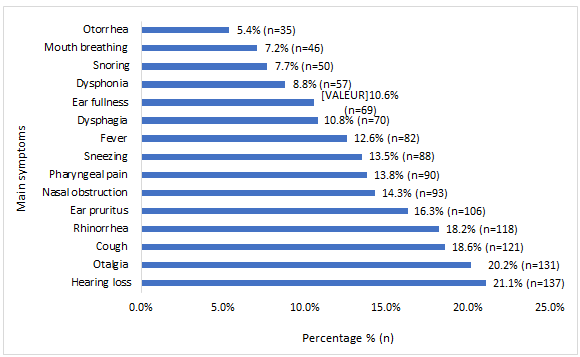
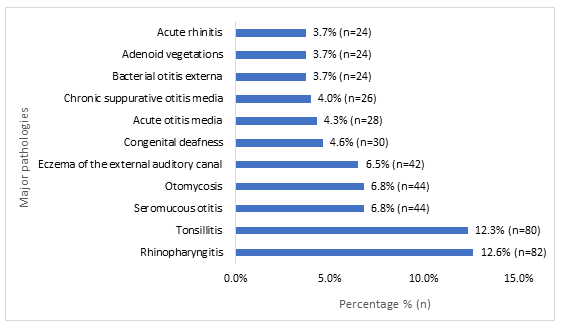
The primary symptoms observed included 21.1% hearing loss (137 cases), 20.2% otalgia (131 cases), 18.6% cough (121 cases), 18.2% rhinorrhea (118 cases) and 16.3% ear pruritus (106 cases). Additional symptoms are detailed in Figure 2. Table 1 provides a comprehensive breakdown of all pathologies and their frequency by sex, with the main pathologies illustrated in Figure 3.
| Otological pathology | Sex | ||
|---|---|---|---|
| Male (n) | Female (n) | Total (n) | |
| Infection – inflammation | |||
| Seromucous otitis | 20 | 24 | 44 |
| Otomycosis | 16 | 28 | 44 |
| Eczema of the external auditory canal | 26 | 16 | 42 |
| Acute otitis media | 14 | 14 | 28 |
| Chronic suppurative otitis media (CSOM) | 14 | 12 | 26 |
| Bacterial otitis externa | 12 | 12 | 24 |
| Mastoiditis | 6 | 4 | 10 |
| Cholesteatomatous chronic otitis media | 2 | 0 | 2 |
| Congenital disease | |||
| Congenital deafness | 20 | 10 | 30 |
| Preauricular fistula | 2 | 6 | 8 |
| Otosclerosis | 0 | 2 | 2 |
| Post-infectious sequelae | |||
| Post-infectious deafness* | 8 | 4 | 12 |
| Tympanic membrane perforation / CSOM | 0 | 4 | 4 |
| Ear plug | |||
| Earwax plug | 14 | 0 | 14 |
| Trauma | |||
| Auricular trauma / cotton swab | 4 | 2 | 6 |
| Acoustic trauma | 2 | 0 | 2 |
| Foreign body | |||
| Ear foreign body | 2 | 2 | 4 |
| Drug toxicity | |||
| Ototoxic hearing loss | 0 | 2 | 2 |
| Total | 162 | 142 | 304 |
Table 1: Link between atopic terrain, passive smoking, and the different regions of the affected ENT sphere.
* Meningitis (n=2); measles (n=8); chickenpox (n=2) Table 1a: Grouping of otological pathologies by sex.
| Pharyngeal pathology | Sex | ||
|---|---|---|---|
| Male (n) | Female (n) | Total (n) | |
| Infection – inflammation | |||
| Rhinopharyngitis | 52 | 30 | 82 |
| Tonsillitis | 40 | 40 | 80 |
| Adenoid vegetations | 16 | 8 | 24 |
| Tonsillitis + adenoids | 12 | 10 | 22 |
| Pharyngitis | 4 | 4 | 8 |
| Enlarged obstructive palatine tonsils | 4 | 0 | 4 |
| Total | 128 | 92 | 220 |
| Rhinosinus pathology | Sex | ||
| Male (n) | Female (n) | Total (n) | |
| Infection – inflammation | |||
| Acute rhinitis | 16 | 8 | 24 |
| Rhinosinusitis | 10 | 10 | 20 |
| Chronic rhinitis | 2 | 4 | 6 |
| Idiopathic disease | |||
| Idiopathic epistaxis | 6 | 4 | 10 |
| Congenital disease | |||
| Septal deviation | 4 | 0 | 4 |
| Partial choanal atresia | 2 | 0 | 2 |
| Foreign body | |||
| Nasal foreign body | 2 | 0 | 2 |
| Total | 42 | 26 | 68 |
Table 2: Link between atopic terrain, passive smoking, and the different regions of the affected ENT sphere.
Table 1b: Grouping of pharyngeal pathologies by sex.
Table 1c: Grouping of rhinosinus pathologies by sex.
| Lower respiratory tract pathology | Sex | ||
|---|---|---|---|
| Male (n) | Female (n) | Total (n) | |
| Foreign body | |||
| Bronchial foreign body | 6 | 0 | 6 |
| Laryngeal foreign body | 2 | 2 | 4 |
| Tracheal foreign body | 2 | 0 | 2 |
| Infection – inflammation | |||
| Laryngitis | 4 | 0 | 4 |
| Congenital disease | |||
| Laryngomalacia | 0 | 2 | 2 |
| Total | 14 | 4 | 18 |
Table 3: Link between atopic terrain, passive smoking, and the different regions of the affected ENT sphere.
Table 1d: Grouping of lower respiratory tract pathologies (larynx, trachea, bronchi) by sex.
| Oral cavity pathology | Sex | ||
|---|---|---|---|
| Male (n) | Female (n) | Total (n) | |
| Congenital disease | |||
| Ankyloglossia | 0 | 8 | 8 |
| Infection – inflammation | |||
| Stomatitis | 2 | 0 | 2 |
| Total | 2 | 8 | 10 |
| Pathology of the neck and face | Sex | ||
| Male (n) | Female (n) | Total (n) | |
| Infection – inflammation | |||
| Cervical adenophlegmon | 8 | 0 | 8 |
| Maxillary abscess | 0 | 4 | 4 |
| Trauma | |||
| Traumatic wound of the cheek | 4 | 0 | 4 |
| Labial oris trauma | 0 | 4 | 4 |
| External buccal traumatic wound | 0 | 2 | 2 |
| Tumor | |||
| Cervical hemangioma | 0 | 2 | 2 |
| Cervical dermoid cyst | 0 | 2 | 2 |
| Congenital disease | |||
| Thyroglossal tract cyst | 4 | 0 | 4 |
| Total | 16 | 14 | 30 |
Table 4: Link between atopic terrain, passive smoking, and the different regions of the affected ENT sphere.
Table 1e: Grouping of oral cavity pathologies by sex.
Table 1f: Grouping of neck and face pathologies by sex.
The affected regions of the ENT sphere (Figure 4) were the ear 46.8% (304 cases), the pharynx 33.8% (220 cases), the nose and sinuses 10.5% (68 cases) and the lower respiratory tract 2.8% (18 cases).
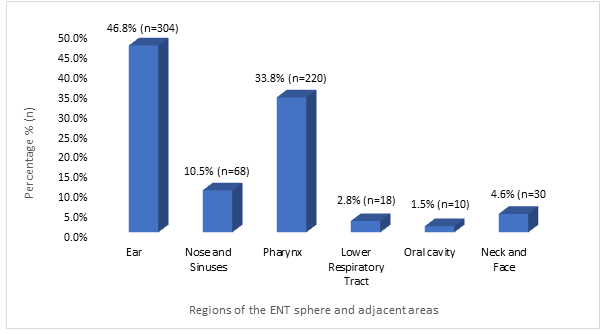
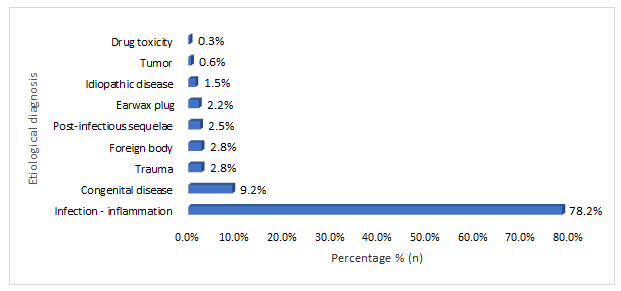
Figure 5 categorizes the nature of the conditions, infections and inflammations constituted 78.2% (508 cases), followed by congenital conditions 9.2% (60 cases), and trauma and foreign bodies, both accounting for 2.8% (18 cases) each.
Children with atopic conditions were more prone to developing rhinosinusitis (p=0.0001), otological (p=0.001), and pharyngeal (p=0.037) conditions (Table 2).
| Atopic predisposition | ||||
|---|---|---|---|---|
| No | Yes | Total | p-value | |
| Ear | 288 | 16 | 304 | 0.001* |
| Nose and sinuses | 46 | 22 | 68 | 0.0001* |
| Pharynx | 188 | 32 | 220 | 0.037* |
| Lower respiratory tract | 16 | 2 | 18 | 0.995 |
| Oral cavity | 10 | 0 | 10 | 0.3 |
| Neck and face | 30 | 0 | 30 | 0.040* |
| Total | 578 | 72 | 650 | |
| Passive smoking | ||||
| No | Yes | Total | p-value | |
| Ear | 290 | 14 | 304 | 0.45 |
| Nose and sinuses | 64 | 4 | 68 | 0.4 |
| Pharynx | 214 | 6 | 220 | 0.25 |
| Lower respiratory tract | 16 | 2 | 18 | 0.15 |
| Oral cavity | 10 | 0 | 10 | 0.55 |
| Neck and face | 30 | 0 | 30 | 0.3 |
| Total | 624 | 26 | 650 |
Table 5: Link between atopic terrain, passive smoking, and the different regions of the affected ENT sphere.
*p<0.05 Table 2: Link between atopic terrain, passive smoking, and the different regions of the affected ENT sphere.
Gender did not significantly influence the affected regions, except for oral cavity pathologies, which were more common in females than males (p=0.017; Table 3).
Additionally, Table 4 indicates that earwax plugs were more frequent in males (p=10-3), while tumors were more frequent in females (p=0.017).
| Affected regions | Sex | |||
|---|---|---|---|---|
| Male (n) | Female (n) | Total | p-value | |
| Ear | 162 | 142 | 304 | 0.3 |
| Nose and sinuses | 42 | 26 | 68 | 0.4 |
| Pharynx | 128 | 92 | 220 | 0.41 |
| Lower respiratory tract | 14 | 4 | 18 | 0.075 |
| Oral cavity | 2 | 8 | 10 | 0.017* |
| Neck and face | 16 | 14 | 30 | 0.7 |
| Total | 364 | 286 | 650 | |
| Etiological diagnosis | Sex | |||
| Male (n) | Female (n) | Total | p-value | |
| Infection – inflammation | 280 | 228 | 508 | 0.4 |
| Congenital disease | 32 | 28 | 60 | 0.6 |
| Trauma | 10 | 8 | 18 | 0.7 |
| Foreign body | 14 | 4 | 18 | 0.07 |
| Post-infectious sequelae | 8 | 8 | 16 | 0.75 |
| Earwax plug | 14 | 0 | 14 | 0.001* |
| Idiopathic disease | 6 | 4 | 10 | 0.925 |
| Tumor | 0 | 4 | 4 | 0.017* |
| Drug toxicity | 0 | 2 | 2 | 0.2 |
Table 6: Link between the different regions of the ENT sphere affected and sex.
*p<0.05 Table 3: Link between the different regions of the ENT sphere affected and sex.
*p<0.05 Table 4: Relationship between etiological diagnosis and sex.
predominantly affected by infections and inflammations, the lower respiratory tract by foreign bodies, and the cervicofacial region by trauma, tumors, and infections.
| Etiological diagnosis | Ear | Nose and sinuses | Pharynx | Lower respiratory tract | Oral cavity | Neck and face | |
|---|---|---|---|---|---|---|---|
| n (p-value) | n (p-value) | n (p-value) | n (p-value) | n (p-value) | n (p-value) | Total | |
| Infection – inflammation | 220 (0.001) * | 50 (0.400) | 220 (0.0001) * | 4 (0.001) * | 2 (0.001) * | 12 (0.001) * | 508 |
| Congenital disease | 40 (0.001) * | 6 (0.925) | 0 | 2 (0.700) | 8 (0.0001) * | 4 (0.300) | 60 |
| Trauma | 8 (0.800) | 0 | 0 | 0 | 0 | 10 (0.0001) * | 18 |
| Foreign body | 4 (0.037) | 2 (0.975) | 0 | 12 (10-5) * | 0 | 0 | 18 |
| Post-infectious sequelae | 16 (0.001) * | 0 | 0 | 0 | 0 | 0 | 16 |
| Earwax plug | 14 (0.001) * | 0 | 0 | 0 | 0 | 0 | 14 |
| Idiopathic disease | 0 | 10 (0.0001) * | 0 | 0 | 0 | 0 | 10 |
| Tumor | 0 | 0 | 0 | 0 | 0 | 4 (0.0001) * | 4 |
| Drug toxicity | 2 (0.200) | 0 | 0 | 0 | 0 | 0 | 2 |
| Total | 304 | 68 | 220 | 18 | 10 | 30 | 650 |
The study identified a 25.1% prevalence of ENT pathologies among children at the Renaissance University Hospital Center in N’Djamena, Chad, which was closely aligning with the 25.8% observed in Benin [4], in Sudan, the prevalence is slightly higher at 26.4% [8], while in Nigeria, in two different studies it reached 36.7% and 39.6% [5, 9]. These variations can be attributed to differences in healthcare systems, access to healthcare, climatic conditions, and pollution levels. It is essential to consider these factors when interpreting the results and developing prevention and treatment strategies tailored to each local context. The study also shows a sex ratio of 1.3, with a predominance to males for ENT pathologies, although sex does not influence the affected ENT sphere regions. This finding is consistent with some previous research, although variations exist depending on the studies and regions [4, 5, 10, 11, 12]. The male predominance could be due to geographical, cultural, biological and environmental factors influencing healthcare- seeking behaviors and susceptibility to ENT pathologies.
In our study, the median age of children with ENT pathologies was 6 years, with a 43.4% of children aged 0 to 6 years. These results are similar to those found in Senegal [10], In contrast, in Nigeria, 43.7% of children were between 0 to 4 years old [5], and in Zambia, 50.3% were under 5 years old [13]. In India, the majority of children 45% were between 6 to 15 years old [14]. These variations may be due to differences in inclusion criteria, data collection methods, as well as demographic and health conditions.
The study observed peaks in ENT pathologies among children in October, March, and September, corresponding to the start of the school year, the intense heat in N’Djamena, and the end of the rainy season. These periods favor the transmission of infections due to school gatherings, heat weakening the immune system, and humidity conducive to pathogens. A study in Madagascar [7], also showed an increase in ENT infections during hot and rainy seasons, confirming the influence of climatic and social factors on these pathologies.
In our study, the most frequently observed symptoms were hearing loss (21.1%), otalgia (20.2%), cough (18.6%), and ear pruritus (16.3%). These findings confirm that otitis and upper respiratory tract infections are prevalent among children [7, 15].
We discovered that 46.8% of the children had ear pathologies, a result that aligns with several studies from Africa, including those in Benin [4], Nigeria [5, 16], and Zambia [13], which also reported high prevalence rates. Similar trends were observed in studies from India [11], Nepal [12], and Bangladesh [15], these results suggest that ear pathologies are common in children globally, regardless of geographical and socioeconomical differences. However, a study in Senegal [10], noted a higher prevalence of rhinosinus conditions, likely due to differences in medical practices and diagnostic criteria.
In our study, 78.2% of ENT pathologies in children were infections and inflammations, predominantly localized in the pharynx, with rhinopharyngitis and tonsillitis being the most common. The primary ear pathologies included seromucous otitis, otomycosis, and eczema of the external auditory canal. These findings align with studies conducted in Madagascar [7], Guinea [6], India [17], and Nepal [12], despite variations due to geographical, climatic and socioeconomic factors. The comparison highlights significant similarities, particularly the prevalence of pharyngeal and ear infections. Several factors explain our results. Firstly, the hot and dusty climate of N’Djamena promotes respiratory and ear infections. Secondly, limited access to healthcare and preventive treatments contributes to the high incidence of infections and inflammations. Lastly, cultural practices and living conditions also play a role in the spread of ENT infections among children.
Our findings reveal a significantly higher incidence of earwax plugs in males. This aligns with the study by Dy AES, et al. [18], which also identified a link between male gender and increased earwax issues, especially in individuals with Down syndrome. This correlation may be attributed to anatomical or behavioral differences between the sexes.
Additionally, we noted a higher frequency of tumors in females. However, no previous studies corroborate this trend, indicating a potential local peculiarity or the need for further research to understand this disparity.
Atopic children in our study were more prone to developing rhinosinusitis, otological, and pharyngeal conditions. These findings are consistent with existing literature, which reports a higher prevalence of ENT conditions in atopic children. The more reactive nasal and pharyngeal mucosa in atopic children likely contributes to easier development of infections and inflammations [19, 20].
Conclusion
A study conducted at the Renaissance University Hospital Center in N’Djamena, Chad, highlights a significant prevalence of ENT pathologies among children, with a slight male predominance and a sex ratio of 1.3. The most affected age group was 0 to 6 years. Infections and inflammations are the most common pathologies observed, children with atopic diseases were particularly vulnerable. Climatic and social factors may contribute to the occurrence of these conditions. Notable gender differences include a higher frequency of earwax plugs in males and tumors in females. These findings underscore the importance of prevention and appropriate management of ENT pathologies, considering local specificities and the rationale of applying evidence-based medicine, effective and cost-effective diagnosis, curative and preventative approaches. This study endeavor aims to deepen the understanding of the epidemiology of these diseases. Such investigations could guide the refinement of healthcare approaches targeting ENT-related ailments.
Declarations
Conflict of Interest: The authors have nothing to declare. Funding: The authors received no financial support from any organization for this study.
References
-
Scasso F, Ferrari G, DE Vincentiis GC, Arosio A, Bottero S, et al (2018) Emerging and re-emerging infectious disease in otorhinolaryngology. Acta Otorhinolaryngol Ital 38(1): 1-106.
-
DeAntonio R, Yarzabal JP, Cruz JP, Schmidt JE, Kleijnen J (2016) Epidemiology of otitis media in children from developing countries: A systematic review. Int J Pediatr Otorhinolaryngol 85: 65-74.
-
Aljehani MJA, Alrasheed SK, Ahmed HM, Fallatah NE (2016) The prevalence and attitude of ear nose throat (ent) infections\problems among medical students. Taibah University, Al-madinah Al-munawara, Kingdom of Saudi Arabia (KSA). Int J Adv Res 4: 751-759.
-
Do Santos Zounon A, Avakoudjo F, Capo-Chichi L, Guezo D, Adjibabi W, et al. (2019) ENT pathologies in children: Epidemiological-clinical aspects and primary prevention. The African Journal of ENT and Head and Neck Surgery 19(2): 43-50.
-
Briggs DC, Ikenga VO, Oparaodu UA, Mbak E (2022) The pattern of paediatric otorhinolaryngological disorders seen at the Rivers State University Teaching Hospital, South-south Nigeria: a 3-year review. Pan Afr Med J 42: 94.
-
Diallo AO, Kolie D, Itiere Odzili FA, Keita A, Dalamou A, et al. (2017) Epidemiological and clinical profiles of pediatric ENT emergencies at the Ignace Deen National Hospital (Conakry University Hospital). Black Med Afr 64(5): 287-293.
-
Randrianandraina MP, Rasamimanana NG, Rakotomalala RS, Rasoanantenaina MG, Randaoharison PG, et al. (2020) Epidemiological-clinical profile of otolaryngological infections in children. Rev Malg Ped 3(1): 90-97.
-
Wail N, Osman M, Inas MAE (2013) Common Ear, Nose & Throat Problems in the Under- Five Sudanese Children. Gezira J Health Sci 9(1).
-
Onotai L, Osuji A, Mbalaso O, Nwankwo B (2020) Evaluation of Common Ear, Nose and Throat Diseases in Rivers State, Nigeria. Ann Clin Otolaryngol 5(1): 1043.
-
Tall H, Bah FY, Nasser T, Sambou A, Diallo BK (2017) Ear, nose and thorat disorders in pediatric patients at a rural hospital in Senegal. Int J Pediatr Otorhinolaryngol 96: 1-3.
-
Gupta V, Gupta A (2019) Pattern of paediatric ear, nose and throat disorders in a district hospital. Int J Otorhinolaryngol Head Neck Surg 5(2): 403-407.
-
Chaudhari B, Gautam D, Pantha T, Arun K, Sharma A (2018) Spectrum of ear, nose and throat disorders among children reporting to the out patient department of a tertiary care center, Nepal. Int J Otorhinolaryngol Head Neck Surg 4: 1125-1129.
-
Kamfwa AM, Mwanakasale V (2016) Pattern of paediatric Ear, Nose and Throat diseases at Arthur Davison Children´s Hospital, Ndola, Zambia. Asian Pac J Health Sci 3(3): 201-208.
-
Surapaneni H, Sisodia SS (2016) Incidence of ear, nose and throat disorders in children: a study in a teaching hospital in Telangana. Int J Otorhinolaryngol Head Neck Surg 2(1): 26-29.
-
Khanam A, Akhtar G, Hossain F, Chowdhury NN, Rahman MA (2017) Pattern of Otolaryngological Diseases among Paediatric Population Attending ENT OPD in a Tertiary Care Centre, Dhaka. Delta Med Coll J 5(1): 30-34.
-
Adegbiji W, Amutta S (2018) Ear Diseases among Primary School Children in Ibadan Metropolis, Southwestern Nigeria. Asian J Med Health 12(3): 1-7.
-
Raju MRK, Fareeduddin M (2020) Prevalence of ear, nose and throat disorders in children at government district hospital Vizianagaram. Int J Otorhinolaryngol Head Neck Surg 6(3): 497.
-
Dy AES, Lapeña JFF Jr (2018) External Auditory Canal Dimensions, Age, and Cerumen Retention or Impaction in Persons with Down Syndrome. Ann Otol Rhinol Laryngol 127(4): 253-257.
-
Gokani SA, Espehana A, Pratas AC, Luke L, Sharma E, Mattock J, et al (2023) Systematic Review of Protein Biomarkers in Adult Patients with Chronic Rhinosinusitis. Am J Rhinol Allergy 37(6): 705-729.
-
Turner JH, Li P, Chandra RK (2018) Mucus T helper 2 biomarkers predict chronic rhinosinusitis disease severity and prior surgical intervention. Int Forum Allergy Rhinol 8(10): 1175-1183.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?