Attitudes towards Risk-Taking at the Beginning of the Covid-19 Pandemic: A Cross-Cultural Study
This study reveals cross-cultural differences in risk-taking attitudes between Asians and Europeans at the onset of the Covid-19 pandemic. It included 2,617 participants aged between 18 and 80 from three Asian (China, India, and Indonesia) and three European (Bulgaria, Germany, and Hungary) countries. The goal is to reveal whether respondents’ attitudes toward risk-taking are affected by cultural context, gender, age, and some demographic characteristics. Results show that Asian participants demonstrate stronger risk-taking attitudes, while Europeans tend to be risk-averse (61.6% vs. 38.4%). Furthermore, Asian women, compared to all other gender groups, are the most prone to risk-taking in conditions of uncertainty (p<0.001). Results also reveal that risk-taking attitudes of individuals vary across age groups being highest among young people and gradually declining with age. Additionally, it is shown that in both Asian and European cultures, the level of education is not a significant factor influencing individuals’ risk-taking attitudes (p>0.05). However, representatives of both cultures who have biological or adopted children in their families are equally likely to avoid the risk, whereas childless Asians, compared with childless Europeans, are more likely to take the risk. There are also significant cultural differences regarding individuals’ marital status, where risk-taking attitudes are stronger for single Asians compared to unmarried Europeans. As another characteristic of individuals, religiosity also influences their attitudes toward risk-taking. One of the findings shows that when the degree of religiosity of Asians decreases, their propensity to take risks increases, whereas the opposite trend is observed for Europeans.
Introduction
Perceived Risk and Risk-Taking Behavior
The critical, life-threatening situation emerging after the outbreak of the Covid19 pandemic in early 2020 is putting individuals’ health behavior to the test. People around the world had to choose whether to take seriously enough the looming danger or to accept that this was fake news overexposed by mainstream media. So that after the pandemic breakout, people around the world faced the choice of either accepting this threat as a real risk to their health and engaging in protective behavior or rejecting the latter and choosing risky behavior. In fact, issues related to risky behavior and risk-taking are part of people’s everyday lives, which explains why such issues are studied in the scientific fields of psychology, sociology, economics, management, and anthropology [1, 2, 3, 4, 5, 6, 7]. Issues of security and risk are permanent and can never be definitively resolved, as today’s security may turn into tomorrow’s insecurity. Or, as Roubini [8] argues, although humanity today is in a period of relative stability, an era of severe instability, conflict, and chaos lies ahead. Arguably, such instability and insecurity were common during the Covid-19 pandemic, and it directed many scholars toward studying people’s risky behavior [9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19]. Such research aims to explore methods and ways to effectively manage people’s health behavior in situations of health uncertainty.
In health-threatening situations such as pandemics, individuals (as well as social groups) are an object of management, as their behavior is generally controlled by external factors such as the state, institutions, dominant value systems, leaders, managers, etc. At the same time, however, individuals can make decisions and manage their actions thanks to their free will and relative autonomy. In other words, the risk behavior of the individual, as a whole, is subject to two types of control – external (social) control, imposed by objective, independent sources /authorities, and internal, subjective control (self-control). Self-control is grounded on the pieces of experience and knowledge of individuals on which they develop their mental models, senses, inner visions, or general attitudes toward risk. However, people’s risk attitudes are generally changeable and can be influenced by characteristics of external situations triggered by extreme social events, natural disasters, or extreme pandemics [10, 20, 21, 22, 23].
In general, authors believe that people may engage in risky behavior because they are unaware of the consequences or because of tolerance to the risk [24]. Others suggest that the reason for engaging in risky behavior is people’s belief that the benefits of their involvement will outweigh the harm [25]. However, people’s choice to engage or not in risky behavior depends on many factors, and above all, on the way they perceive the threat and the risk situation in general. The fact that perceived risk determines the risk behavior of individuals motivated many researchers to investigate the process of risk perception at the beginning of the Covid-19 pandemic [13, 26, 27, 28].
Risk-taking refers to the subjective assessment of the danger arising from an event that has already occurred or will come in the future. Individuals rate events as dangerous and risky depending on whether they affect their important needs and depending on the extent to which they harm their well-being or threaten their lives. It is reasonable to assume that if the expected event endangers the health or survival of people, they will perceive the situation (event) as extremely risky and will engage in protective behavior. Therefore, it should be kept in mind that it is perceived risk that mediates engaging in risky behavior or engaging in protective behavior. In this sense, the way in which a hazard is perceived may increase or decrease the likelihood of engaging in risky behavior [29, 30, 31].
The thesis that risk-taking behavior is dependent on perceived risk is not new. Many authors have argued that engagement in risky behavior depends on how individuals perceive risk and the extent to which they believe they are threatened by potential danger [25]. Different perspectives converge around the view that perceived risk and individuals’ responses to danger are mediated by psychological, social, and cultural factors. For example, Kasperson, et al. [32] argue that hazards interact with psychological, social, institutional, and cultural processes, whereas the characteristics of this interaction determine risk perception and risk-taking behavior.
The resulting situation of uncertainty, created by the Covid-19 pandemic, was a trigger that activated the risk- taking behavior of individuals, and they had two alternatives before them - either to comply with the impending life- threatening danger or to ignore it. They had to decide whether to engage in protective behaviors by complying with the enforced official measures of limiting contacts, keeping their distance, wearing masks, lockdown, and future vaccination or to reject all these measures and engage in risk-taking behaviors. The choice, in this case, was not only influenced by the pressure of external factors such as the media, governments, and medical institutions, but at the same time, it was dependent on the existing characteristics of individuals, on their pre-formed risk-taking attitudes.
Although the essential role of the media should be emphasized, it is necessary to state that media effects on individuals are not generally mechanical, and the media does not directly influence risk-taking behavior. As mentioned, all external influences on individuals are mediated through previously developed mental models, senses, inner visions, or general attitudes toward risk. This means that at the moment of the outbreak of the pandemic, despite media influence and government control, each individual had a preformed attitude on how to act in a situation of danger, whether to engage in or reject risk-taking behavior.
To effectively manage the behavior of individuals in extreme situations it is essential to know to what extent they are likely to engage in risky behavior and whether their risk- taking attitudes are influenced by factors such as culture, gender, age, education, etc. To answer these questions, we conducted the present cross-cultural study. An indicator used in the current study to judge risk behavior in a viral threat situation is the personal readiness of individuals to avoid risk by vaccination or to engage in risk-taking behavior by refusing vaccination. Although the vaccines against Covid-19 did not exist at the beginning of 2020, at the time of the pandemic outbreak people had prior attitudes towards vaccines and vaccination in general [33]. Therefore, exploring these attitudes would contribute to the successful management of risk behavior during pandemic situations in the future.
Materials and Methods
Purpose of the study and hypotheses Based on the analysis presented above, the study aims to show whether, in a situation of extreme health uncertainty caused by the Covid-19 pandemic, people tend to take a risk by refusing to vaccinate against the virus and also to show whether the attitudes of individuals to take this risk are influenced by the cultural context, gender, age, and certain demographic characteristics.
In accordance with the purpose of the study, the following hypotheses were formulated: Hypothesis 1. In situations of health uncertainty such as that generated by the Covid-19 pandemic, risk-taking attitudes are higher among members of collectivistic cultures than among members of individualistic cultures. Hypothesis 2. Gender differences mediate risk-taking behavior, and as a result, in situations of health uncertainty, like the Covid-19 pandemic, the risk-taking attitudes among men are higher than in women. Hypothesis 3. In situations of health uncertainty, the tendency toward health-risk behaviors varies across age groups and is stronger among younger people. Hypothesis 4. In situations of health uncertainty, such as the Covid-19 pandemic, risk-taking attitudes across cultures are influenced differently by certain demographic factors.
Participants The subjects of the study were representatives of two cultural groups drawn from Europe and Asia. The total number of participants included 2617 subjects, aged between 18 and 80 (M = 37.98, SD = 15.20), 1412 of which were drawn from Asia (45.9% identified as women, 49.6% as men, and 4.5% preferred not to answer), and 1205 were representatives of Europe (64.6% identified as women, 34.5% as men, and 0.9% preferred not to answer). The average age of the participants from Asia was 32 years (M = 31.50, SD = 12.77). The average age of the participants from Europe was 45 years (M = 44.96, SD = 14.51).
The distribution of participants in the study is as follows: Asia: The study included representatives of three countries – China (N = 500), India (N = 500), and Indonesia (N = 412). These are the three Asian countries, influenced by collectivistic values with the largest populations but different religious systems – namely Buddhism, Hinduism, Islam, Taoism, Confucianism, and Catholicism.
Europe: The study included participants from Bulgaria (N = 405), Germany (N = 400), and Hungary (N = 400). These three countries, in general, are typical representatives of European Christian civilization and culture.
The respondents differed in age, education, financial status, qualifications, marital status, religious beliefs, and different party affiliations, which reflects appropriately the cultural characteristics of the two groups.
Materials and Procedure
The study was conducted online from April to June 2020. Participants were asked to complete an internet-based version of a short questionnaire that described the extreme Covid-19 pandemic situation. The items were related to the main characteristics of the virus and the pandemic situation, such as the virus origin, functions of the virus, desire for vaccination, precautions against infection, etc. Subjects had to present their answers on a six-point Likert scale. One of the items was related to risky behavior and aimed to measure subjects’ attitudes toward risk-taking at the beginning of the Covid-19 pandemic. We reasoned that by examining individuals’ attitudes toward vaccines and vaccination as a means of avoiding life-threatening danger, we could identify risk-taking tendencies. The wording of this item is as follows: Even if I am likely to get infected with a dangerous disease, I would not get vaccinated in advance because the vaccines are too suspicious.
It was expected that in answering this question, a proportion of the subjects would prefer the risk-taking of contracting a contagious disease rather than getting vaccinated. In addition, another portion of the subjects was expected to be inclined to vaccinate to avoid the risk, despite the possibility that the vaccines were questionable.
The results received had to reveal the attitudes of separate groups, differentiated according to sex, age, cultural context, and some specific demographic characteristics, to risk-taking in an extreme situation like the Covid-19 pandemic. For this purpose, respondents had to answer questions separated into a section, including demographic characteristics, as follows: sex, age, profession, family status, biological or adopted children, number of children in a family, severe childhood illnesses, current employment, financial status, religion, political orientation, etc. To reveal the influence of age on risk-taking attitudes, the subjects were divided, according to the concept of [34], into three age groups, as follows: Early Adulthood – up to 35 years; Midlife – from 36 to 50; Mature Adulthood – over 50.
To examine the hypotheses, the following statistical methods were employed: descriptive statistics, independent samples T-test, One-Way and Two-Way ANOVAs, and post hoc tests.
To conclude this section, it is necessary to specify once again that the subject of the present study is the preliminary attitudes (predispositions) of individuals towards risk- taking at the beginning of a pandemic outbreak when there is still no medical countermeasure to the virus. The Research Ethics Approval Procedure was not applied in this study, as the survey was anonymous, and respondents completed the online questionnaire voluntarily.
Results
Examination of risk-taking and the factors this depends on in health uncertainty situations is essential to the successful management of the health behaviors of individuals. The present study reveals trends in risk- taking and risk avoidance early in the Covid-19 pandemic and answers the question of whether risk-taking attitudes are mediated by cultural context, gender, age, and some demographic characteristics. According to Hypothesis 1, at the onset of the Covid-19 pandemic, attitudes of individuals toward risk-taking are higher among representatives of the collectivistic culture compared to representatives of the individualistic culture.
The frequency distribution analysis in the representatives of the two cultures with low and high risk-taking tendencies confirms Hypothesis 1. The results show that in the Asian sample, compared to the European, most individuals surveyed demonstrate a greater propensity to engage in risky behavior – 61,6% vs. 38,4% (Table 1). The data clearly shows that during the initial period of the Covid-19 pandemic, Europeans are characterized by a tendency to avoid taking risks by getting vaccinated, despite the claim that vaccines are dubious, while this trend is exactly the opposite for Asians.
| Europe & Asia | Total | ||||
|---|---|---|---|---|---|
| Europe | Asia | ||||
| Even if I am likely to get infected with a dangerous disease, I would not get vaccinated in advance because the vaccines are too suspicious. | Low risk-taking tendency | Count | 825 | 794 | 1619 |
| % | 51% | 49% | 100% | ||
| High risk-taking tendency | Count | 380 | 610 | 990 | |
| % | 38.40% | 61.60% | 100% | ||
| Total | Count | 1205 | 1404 | 2609 | |
| % | 46.20% | 53.80% | 100% |
Table 1: Trends in risk-taking attitudes across cultures.
This conclusion is supported by the results obtained from the application of the Independent-Samples T-Test, which shows that at the beginning of the Covid-19 pandemic, the average level of risk-taking propensity is higher in Asia – n=1404, x=1.43, SD=0.50, compared to Europe – n=1205, x=1.32, SD=0.47, with the differences being statistically significant – t(2587)=-6.33, p<0.001, d=0.25.
Hypothesis 2 assumes that gender differences mediate risk-taking, in situations of uncertainty, like the Covid-19 pandemic, and as a result, the risk-taking attitudes among men are higher compared to women. Comparing data obtained for males and females in the entire sample shows that there is no statistically significant difference between them – t(2534)=-1.67, p=0.096, n.s. This means that formulated Hypothesis 2 must be rejected, but the opposite hypothesis cannot be accepted either, although the average for women – x=2.98, is slightly higher than that for men – x=2.87.
To assess cross-cultural variations in gender differences, a One-Way ANOVA was used with the independent variable “gender X type of culture” and the dependent variable “risk-taking/risk aversion”. The results show that there are statistically significant differences between men and women from different cultures in terms of risk-taking attitudes – F(3,2539)=18.14, p<0.001, η=0.14. Descriptive statistics are presented in Table 2.
Even if I am likely to get infected with a dangerous disease, I would not get vaccinated in advance because the vaccines are too suspicious N Mean Std. Deviation Std. Error 95% Confidence Interval for Mean Minimum Maximum Lower Bound Upper Bound Male EU 416 2.52 1.714 0.084 2.35 2.68 1 6 Female EU 777 2.8 1.77 0.064 2.67 2.92 1 6 Male ASIA 704 3.09 1.57 0.059 2.97 3.2 1 6 Female ASIA 646 3.2 1.577 0.062 3.08 3.33 1 6 Total 2543 2.94 1.676 0.033 2.87 3 1 6 Table 2: Gender differences in risk-taking attitudes.
Since Levene’s test revealed inequality in between-group – F(3,2539)=9.75, p<0.001, the Games-Howell post hoc test was applied to assess differences in means.
Statistically significant differences were found between the means of all groups studied, except for the group of men and women from Asian cultures - p>0.05, n.s. In other words, the highest levels of risk-taking tendency are characteristic of representatives of Asian culture, regardless of their gender affiliation, followed by European women and finally by European men (Table 2).
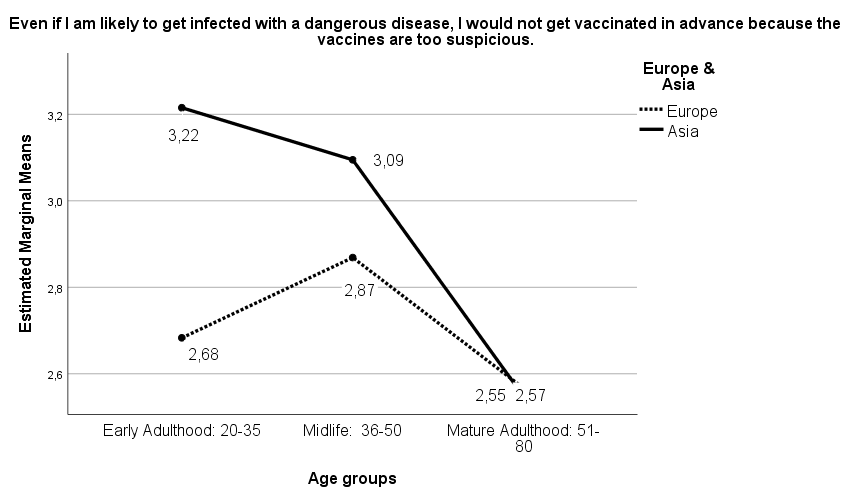
An important research task was to reveal whether, at the onset of the Covid-19 pandemic, the tendency of risk- taking varies across age groups. Consistent with Hypothesis 3, we presupposed that this trend varies across age groups and is highest among young adults. Applying One-Way ANOVA shows that age has a statistically significant effect on the level of risk-taking – F(2,2474)=18.83, p<0.001, η=0.12. Since Levene’s test demonstrated the equality of variances – F(2,2474)=1.54, p=0.215, Scheffe’s post hoc test was used to determine differences in means between the groups. The results reveal that the 20-35-year-olds have the highest risk-taking values – x=3.07, followed by the 36-50-year-olds – x=2.95, and finally, the 51-80-year-olds are positioned – x=2.56. The contrast group is the oldest because it statistically differs most significantly from both younger groups of respondents – p<0.001. Therefore, the tendency towards risk-taking decreases with increasing age. Two-Way ANOVA with independent variables “age” and “type of culture” and dependent variable “level of risk- taking” shows that there are both statistically significant independent effects of age – F(2,2477)=11.01, p<0.001, η=0.09 and culture – F(1,2477)=10.38, p<0.001, η=0.06, as well as their combined effect on the variability of risk-taking attitudes – F(2,2477)=4.69, p<0.01, η=0.06. The results are visualized in Figure 1.
It is noteworthy that while in Asian cultures, with increasing age, risk-taking tendency decreases, among European nations, risk-taking trends peak in the mid-life cycle. The differences between the two cultures are most pronounced in the period of Early Adulthood [20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35], where there is a stronger risk-taking tendency among Asian respondents. Towards the end of the life course, cross- cultural differences are minimized and neutralized, and the risk-taking tendency decreases (Figure 1).
According to Hypothesis 4, across cultures, certain demographic factors affect risk-taking attitudes differently in situations of uncertainty. We accept that education is an essential factor influencing people’s risk-taking attitudes. To reveal the extent to which education influences risk-taking attitudes, respondents were asked to provide information on their level of education by indicating one of the following educational levels: primary education, secondary education, bachelor’s degree, master’s degree, doctoral degree, or higher. As educational degrees in Europe and Asia are not identical, we judged that the length of training best reflects the education level. For this reason, mentioned degrees were divided into two groups, indicating low and high educational levels. The first group included primary and secondary education, and the second included bachelor’s, master’s, doctoral or higher degrees. To prove that educational level affects risk-taking, the differences in the mean values of the low and high-education groups had to be statistically significant.
Application of Independent Samples T-test shows that the difference in means between the two educational groups – “primary and secondary education” – x=2.91, and “bachelor’s, master’s, and doctoral degree” – x=2.95, in terms of risk attitudes, are not statistically significant – t(2584)=- 0.48, p=0.631, n.s.
The two-factor effects between education and culture type on attitudes towards risky behavior were also not statistically significant – p>0.05. Figure 2 visualizes the obtained results.
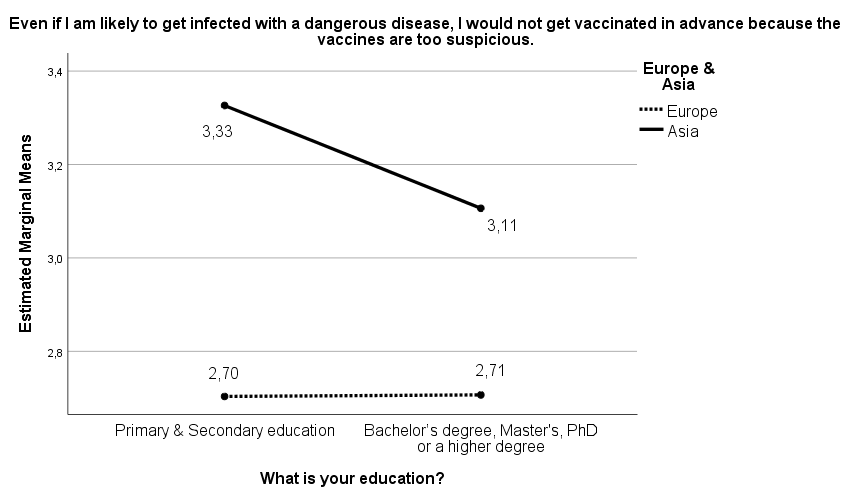
Although there are no statistically significant differences between the two cultures, the results reveal that while education is not a factor influencing the risk-taking attitudes of Europeans, in relation to Asians there is a tendency, which shows that increasing the educational level of individuals decreases their readiness to engage in Risk-taking behavior.
Risk-taking in a life-threatening situation is an action that affects not only separate individuals but also their families, so marital status was identified as an essential demographic characteristic in the study. According to this characteristic, subjects were divided into four groups – I am single, I am married, I am divorced, and I live with a partner in cohabitation. Data for individuals falling into the latter two categories were pooled in statistical processing. This was necessary because the subjects included in the category I live with a cohabiting partner were few compared to the participants in the others.
After recording the marital status variable into three groups (I am single, I am married, and I am divorced/I live with a partner in cohabitation) and applying One-Way ANOVA, the following results were obtained – F(2,2575)=6.59, p<0.001, η=0.07. This result indicates that marital status is a significant factor in the variation in risk-taking attitudes in the COVID-19 situation. The highest average value is the group of singles – x=3.09, followed by the group of married – x=2.86, and finally, the group of divorced and cohabiting persons is positioned – x=2.81. Since Levene’s test showed inequality of variances – F(2,2575)=8.56 at p<0.001, Games- Howell’s post hoc test was used to compare means. It reveals that the singles are statistically significantly different from the other two groups of respondents.
In Two-Way ANOVA, the variable “type of culture” has statistically significant independent effects – F(1,2587)=22.00, p<0.001, η=0.09, as well as two-factor effects, between cultural characteristics and marital status, on risk-taking attitudes – F(2,2587)=4.59, p<0.01, η=0.06. However, the independent influence of the “family status” factor is not statistically significant - F(2,2587)=0.61, p>0.05.
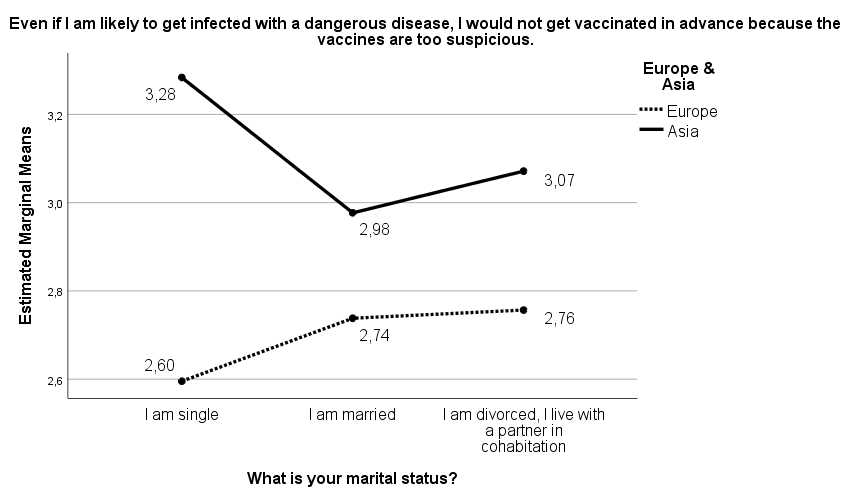
The obtained results are visualized in Figure 3. Results show that the greatest cross-cultural distance is observed between single Asians, for whom the value of risk-taking attitudes is the highest, and single Europeans, for whom this value is the lowest.
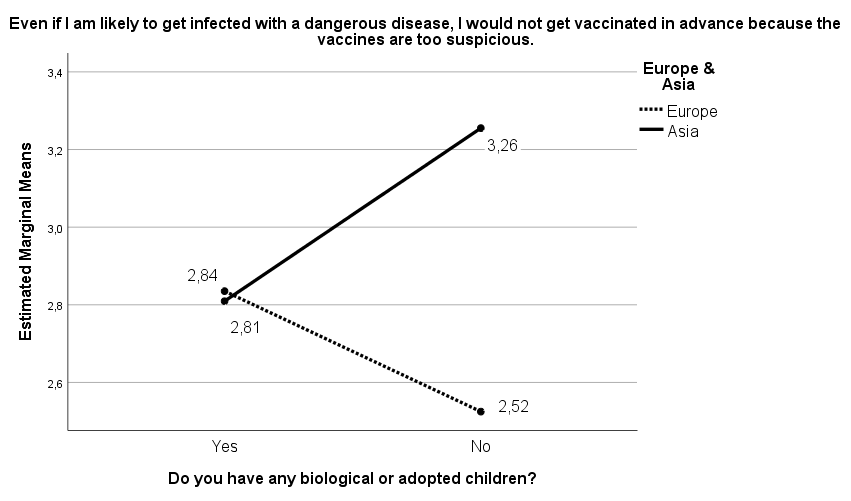
We considered that an important characteristic that influences risk-taking in situations of uncertainty is the presence or absence of children in the family. The combined effects of having children in the family and culture type on the degree of perceived risk were statistically significant – F(1,2580)=28.47, p<0.001, η=0.1. However, while cultural affiliation registered independent statistically significant effects – F(1,2580)=24.72, p<0.001, η=0.1, the effects were not statistically significant for the other factor variable, the presence of children – F(1,2580)=0.91, p>0.05, n.s. Figure 4 gives an interesting perspective on the results.
We assumed that religiosity is an important characteristic that mediates risk-taking in situations of uncertainty. In processing the data, the religiosity variable was recoded into three degrees – I am religious/I am deeply religious, I have moderate religious feelings, and I believe in something indefinite/I am an atheist. It turned out that in the situation of uncertainty created by the Covid-19 pandemic, religiosity did not significantly influence the risk-taking attitudes of individuals – F(2,2577)=2.44, p=0.087, n.s.
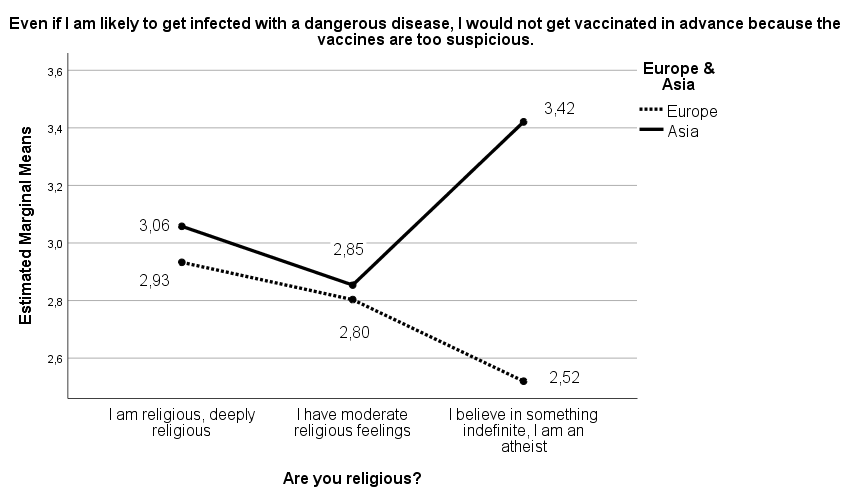
Two-Way ANOVA analysis shows the independent effects of religiosity were also not statistically significant – F(2,2580)=2.31, p=0.10, n.s. However, the combined effects with the “type of culture” had a statistically significant impact (F(2,2580)=19.24, p<0.001, η=0.12) on risk-taking attitudes. The independent effects of “type of culture” also have a statistically significant impact on risk-taking attitudes – F(1,2580)=28.78, p<0.001, η=0.10. Figure 5 presents the inferred trends.
The data shows that between Europeans and Asians who are religious and deeply religious, there are no significant differences in risk-taking attitudes in situations of uncertainty. The same trend applies to Europeans and Asians with moderate religious feelings. However, there is a significant difference between Asians and Europeans, who are atheists and believe in something undefined. Asians belonging to this group have strong attitudes to risk-taking in situations of uncertainty, while Europeans from the same group do not have such attitudes. Figure 5 shows that there is a further trend to bear in mind, namely: for Asians, risk- taking attitudes increase as religiosity decreases, while for Europeans, risk-taking also decreases as religiosity decreases.
Discussion
The survey results presented in the previous section (Table 1) show that at the beginning of the pandemic, people’s risk-taking attitudes were higher among Asians than Europeans. Data for Europeans show a clear tendency to avoid risk to their health by demonstrating readiness for vaccination, even though vaccines are questionable, while Asians demonstrate the opposite attitude. Differences between the features of Asian collectivist and European individualistic culture could explain the greater readiness of Asians to take risks in situations of uncertainty and the willingness of European to avoid them. As it is known, according to the cultural perspective, societies can be divided into two main types – individualistic and collectivist [35, 36, 37, 38, 39, 40, 41, 42, 43]. Individuals in individualistic societies are loosely connected to each other and their attention is focused primarily on themselves, whereas in collectivistic societies individuals are closely connected to the group, loyal to it, and rely on mutual support [44, 45].
Since European culture is defined as individualistic and Asian culture is traditionally perceived as collectivist, it is hypothesized that the differences in risk-taking attitudes between Europeans and Asians are due to the different characteristics of the two cultures. For example, from a cultural perspective, it can be assumed that members of the European individualistic culture, in general, tend to perceive hazardous situations primarily as risky only to their well- being or that of their families. Conversely, representatives of Asian culture perceive such situations as a threat not only to their own and their families’ well-being but also to the well-being of the group to which they belong (organization, society). In this sense, the risk-taking tendency of Asians differs from that of Europeans, as the former has a pre- existing risk-taking attitude with a much broader scope than the latter. This willingness to take risks, not only for oneself but also for others, the group, and society as a whole, is built into the personality of Asians and is an integral part of Asian self-identity. This pre-cultivated risk-taking attitude is activated when extreme situations arise, which increases levels of stress and anxiety in individuals about their safety, the safety and well-being of the group, and society, as a whole. We suppose that it is this pre-formed risk-taking attitude of Asians that was maximally aroused at the onset of the Covid-19 pandemic, which in part can account for the cross-cultural differences mentioned above.
However, the different trends between European and Asian representatives in terms of risk-taking attitudes can also be explained by the phenomenon of power distance, which is defined as the extent to which individuals accept that the power in society is distributed unequally [46]. The extent to which people perceive that power in society is distributed unequally is measured by the so-called Power Distance Index (PDI), introduced by G. Hofstede [43]. According to this index, societies can be conventionally divided into two groups - low and high-power distance societies. In the former, power is assumed to be equally distributed, and there is a low distance between those at the top of the power hierarchy and those at the bottom. Inherent in these societies is a flatter power structure, greater decentralization, and greater trust in those in power. Conversely, high power distance societies are characterized by strict hierarchies, large bureaucracies, tolerance of inequality, and less trust in those in power. There are numerous studies of the Power Distance phenomenon and its relationship to other phenomena such as cultural context, social identity, political culture, organizational effectiveness, etc. [47, 48, 49, 50]. Studies generally find that low power distance is inherent in most societies with an individualistic culture, whereas high power distance dominates in most societies with a collectivist culture. From this perspective, we hypothesize that high power distance in collectivist societies, characterized by low trust in those in power, may be one of the reasons for high risk-taking attitudes and lack of willingness to vaccinate at the onset of the Covid-19 pandemic. On the contrary, the low distance of power inherent in individualistic societies implies the presence of higher trust in the rulers, as a result of which there is a tendency to agree with them and avoid risk-taking behavior by accepting the vaccination.
The third reason that could explain the differences between the risk-taking attitudes of the two samples, the Asian and the European, can be explained by the fact that still at the beginning of the Covid-19 pandemic, the world media spread the information that it was Western companies which had advanced in their research and would very soon offer life-saving vaccines. This information was subsequently confirmed when FDA authorized the Janssen/Johnson & Johnson, Pfizer-BioNTech, and Moderna COVID-19 vaccines. In this case, it could be assumed that the greater mistrust of Asians towards the above-mentioned Western companies, compared to the greater trust of Europeans towards them, is one of the reasons for the different risk-taking tendencies found.
In conclusion, it can be claimed that the trends in risk- taking and risk avoidance early in the Covid-19 pandemic, found in the present study, are most likely caused by the differences between types of cultures, individualistic and collectivist, combined with differences between the power distance and the degree of trust in the West.
According to Hypothesis 2, we hypothesized that gender differences affect the health behavior of individuals and expected risk-taking attitudes among men to be higher than those of women at the beginning of the Covid-19 pandemic. This assumption is based on the fact that, in general, men, compared to women, are more prone to risky behavior – they are prone to aggression, need to dominate over others, seek challenges, participate in fights, make wars, etc. Due to their traditional role of raising children and caring for the family, women are more conservative and are not prone to risky behavior. However, analysis of the results for the entire sample shows that there is no statistically significant difference between men and women in terms of their risk- taking attitudes. Therefore, formulated Hypothesis 2 must be rejected, but at the same time, the opposite hypothesis cannot be accepted. However, the data of the comparison between the two samples shows that there are statistically significant differences between women and men as representatives of Asian and European cultures. For example, Asian women, compared to all other groups, are the most prone to risk- taking in conditions of uncertainty. The same is true for Asian men versus European women and men. This is a logical result since, as stated above, both Asian men and Asian women are equally affected by the features of collectivist culture, combined with the aforementioned high-power distance and distrust of the West.
The analysis of the data, related to the proof of the third hypothesis, shows that at the beginning of the Covid-19 pandemic, attitudes toward risk-taking varied among different age groups, being the highest among young people and gradually decreasing with advancing age. This result is not surprising as young people have physiological and psychological resources to engage in risky behaviors. They have a low tolerance for submission and servility, and as agents of social change, they are ready to face any challenge in situations of uncertainty. As a reason for these results, the unprecedented influence of the mass media on the Mature Adulthood group must be taken into account. It was the media that suggested, at the very beginning of the pandemic, that the only way for the elderly to survive was voluntary self-isolation and obligatory vaccination.
While the trend of decreasing risk-taking attitudes with age increasing is not surprising, what is quite surprising is the result obtained when comparing the age dynamics between the two cultures. While there is a strong tendency among young Asians to risk contracting the virus by refusing vaccination, the opposite is true among young Europeans. These results can be explained not only by differences between the two cultures but also by differences between young Europeans and young Asians concerning the phenomenon of power distance and trust in medical institutions. Young Europeans have risk-averse and vaccine- accepting attitudes due to high trust in medical institutions and western companies developing life-saving vaccines, while young Asians have the opposite tendency.
The results of the study show that at the onset of the Covid-19 pandemic, risk-taking attitudes in Asian and European cultures were influenced differently by certain demographic factors. Regarding the education factor, however, this assumption has not been proven. Although no statistically significant differences are found between the two samples, different trends emerge regarding the two cultures. The findings show (Figure 2) that attitudes towards risk-taking behavior in the Asian sample decrease as the level of education increases, while in the European sample, individuals’ attitudes towards risk-taking are not affected by their level of education.
The results of the study show that marital status has a significant impact on individuals’ risk-taking attitudes. Singles demonstrate a strong attitude toward risk-taking (Figure 3), which sets them apart significantly from married people or those who are divorced or cohabiting. This can be explained by the fact that the risk for them is only personal, as they are not tied to families and children who depend on them. Another reason for this trend lies in the young age of unmarried individuals who, as stated above, possess the physiological and psychological readiness to engage in risky behavior. The significant differences observed between single Asians with high risk-taking attitudes, and single Europeans with low risk-taking attitudes, can again be explained by cultural differences, as well as by differences between them in relation to the phenomenon of Power distance and the level of trust in medical institutions and Western companies developing life-saving vaccines.
The results obtained concerning the factor of biological or adopted children show that both Asians and Europeans who have children in their families have similar risk-taking attitudes. Obviously, for parents, risk-taking is not only a personal act, as they are also dependent on the presence of children in the family. In this case, it is interesting to pay attention to the difference between members of the two cultures who do not have children (Figure 4). Among Asians in this group, there is a strong tendency towards risk-taking, whereas childless Europeans’ attitudes towards risk-taking and refusal to vaccinate are significantly weaker. The high risk-taking tendency among Asians can again be explained by their cultural characteristics and, above all, by their distrust of medical institutions and the fact that it is Western companies which develop life-saving vaccines.
Results of the research also show that, in some cases, people’s attitudes toward risk-taking are influenced by their level of religiosity (Figure 5). For example, among Asians, there is a clear tendency to weaken their risk-taking attitude with increasing levels of religiosity. This tendency can be explained by the fact that in a situation of uncertainty, religious individuals are not inclined to risky behavior because they believe that God is the one who will help them to avoid impending danger. The opposite trend is evident for Europeans, although it is not strongly expressed. Atheist Asians, however, demonstrated strong attitudes about taking the risk of contracting the virus and avoiding vaccination, differing significantly from European atheists who did not have such attitudes. The explanation, in this case, can also be linked to the lack of sufficient trust of Asian atheists in the government, medical institutions, and Western companies developing life-saving vaccines.
In conclusion, we should note that a number of other demographic characteristics were included in the demographic section, such as occupation, financial status, childhood illnesses, encounter with death, etc., but the results showed that they did not have a significant impact on individuals’ attitudes towards risk-taking in a situation of uncertainty.
Conclusion
This study generally sheds light on cross-cultural differences in risk-taking in the face of uncertainty, drawing on data from research conducted in Asia and Europe at the beginning of the Covid-19 pandemic. Based on the research data, we can summarize that at the beginning of the pandemic, people’s attitudes toward risk-taking were higher among Asians than among Europeans, that risk- taking attitudes vary across age groups being highest among young people and gradually decreasing with age, and that in general, gender differences do not influence individuals’ risk- taking attitudes. Furthermore, findings suggest that certain demographic characteristics affect individuals’ risk-taking attitudes differently. For example, findings suggest that at the onset of the Covid-19 pandemic, people’s educational level did not influence their readiness to engage in risk-taking behavior, whereas demographic characteristics such as marital status, the presence of biological or adopted children in the family, and the degree of religiosity of individuals influenced risk-taking attitudes. Based on the cross-cultural analysis, Asians who are young, less educated, less religious, unmarried, and have no biological or adopted children, compared to Europeans with the same characteristics, have stronger attitudes towards risk-taking in situations of uncertainty.
Strengths, weaknesses and future research goals The strongest side of this study is that the results obtained answer the question of what the attitudes of representatives of the two cultures, Asian and European, are towards taking risks to their health by refusing future vaccinations at the onset of the Covid-19 pandemic. Findings that both cultural context and differences in gender, age, education, marital status, presence of children in the family, and degree of religiosity influenced risk-taking attitudes at the onset of the Covid-19 pandemic will help to effectively manage people’s risk-taking behavior in future situations of health uncertainty. The weakness of the work is that, due to the limited number of participants in the national samples, no comparative analysis has been made across countries, and only the cross-cultural aspect of the issue of risk-taking has been analyzed.
References
-
Boholm A (2015) Anthropology and Risk. Routledge, London.
-
Gigerenzer G (2015) Simply rational: Decision making in the real world. Oxford University Press.
-
Hopkin P (2010) Fundamentals of Risk Management: Understanding, Evaluating and Implementing Effective Risk Management. London: Kogan Pag.
-
Kahneman D (2011) Thinking, Fast and Slow. Farrar, Straus, and Giroux. New York, ISBN 978-0374275631.
-
Slovic P (1987) Perception of risk. Science 236(4799): 280-285.
-
Slovic P (2010) The Feeling of Risk: New Perspectives on Risk Perception. Routledge, London.
-
Walaski P (2011) Risk and Crisis Communications: Methods and Messages. New York: John Wiley & Sons, Incorporated.
-
Roubini N (2022) MegaThreats: Ten Dangerous Trends That Imperil Our Future, And How to Survive Them. Little, Brown and Company, ISBN-13: 9780316284059.
-
Adachi M, Murakami M, Yoneoka D, Kawashima T, Hashizume M, et al. (2022) Factors Associated with the Risk Perception of COVID-19 Infection and Severe Illness: A Cross-Sectional Study in Japan. SSM Popul. Health 18: 101-105.
-
Chan HF, Skali A, Savage DA (2020) Risk attitudes and human mobility during the COVID-19 pandemic. Sci. Rep 10: 19931.
-
Cipolletta S, Andreghetti GR, Mioni G (2022) Risk Perception towards COVID-19: A Systematic Review and Qualitative Synthesis. International Journal of Environmental Research and Public Health 19(8): 4649.
-
Fersch B, Schneider-Kamp A, Breidahl KN (2022) Anxiety and trust in times of health crisis: How parents navigated health risks during the early phases of the COVID-19 pandemic in Denmark, Health, Risk & Society 24(1-2): 36-53.
-
Dryhurst S, Schneider CR, Kerr J, Freeman ALJ, Recchia G, et al. (2020) Risk perceptions of COVID-19 around the world. Journal of Risk Research 23(7-8): 994-1006.
-
Heydari ST, Zarei L, Sadati AK, Moradi N, Akbari M, et al. (2021) The effect of risk communication on preventive and protective Behaviours during the COVID-19 outbreak: Mediating role of risk perception. BMC Public Health 21(1): 54.
-
Patterson NJ, Paz-Soldan VA, Oberhelman R (2022) Exploring perceived risk for COVID-19 and its role in protective behavior and COVID-19 vaccine hesitancy: a qualitative study after the first wave. BMC Public Health 22: 503.
-
Petherick A, Goldszmidt R, Andrade EB (2021) A worldwide assessment of changes in adherence to COVID-19 protective behaviours and hypothesized pandemic fatigue. Nat Hum Behav 5: 1145-1160 17. Siegrist M, Luchsinger L, Bearth A (2021) The Impact of Trust and Risk Perception on the Acceptance of Measures to Reduce COVID-19 Cases. Risk Analysis 41: 787-800.
-
Tsai CI, Zeng Y (2021) Risky but alluring: Severe COVID-19 pandemic influence increases risk taking. Journal of Experimental Psychology: Applied 27(4): 679-
-
Yang XY, Gong RN, Sassine S, Morsa M, Tchogna AS, et al. (2020) Risk Perception of COVID-19 Infection and Adherence to Preventive Measures among Adolescents and Young Adults. Children 7(12): 311.
-
Abatayo AL, Lynham J (2020) Risk preferences after a typhoon: An artefactual field experiment with fishers in the Philippines. Journal of Economic Psychology 79: 102195.
-
Hanaoka C, Shigeoka H, Watanabe Y (2018) Do risk preferences change? evidence from the great east Japan earthquake. Am Econ J 10: 298-330.
-
Trautmann ST, van de Kuilen G (2018) Higher order risk attitudes: A review of experimental evidence, European Economic Review 103: 108-124.
-
Li KK, Huang B, Tam T, Hong Y (2020) Does the COVID-19 Pandemic Affect People’s Social and Economic Preferences? Evidence from China pp: 1-23.
-
Galizzi M, Tempesti T (2015) Workers’ Risk Tolerance and Occupational Injuries. Risk Analysis 35: 1858-1875.
-
Weber EU, Blais AR, Betz NE (2002) A domain-specific risk-attitude scale: measuring risk perceptions and risk behaviors. J. Behav. Decis. Mak 15: 263-290.
-
Abeysinghe S, Amir V, Huda N, Humam F, Lokopessy AF, et al. (2022) Risk and responsibility: lay perceptions of COVID-19 risk and the ‘ignorant imagined other’ in Indonesia, Health, Risk & Society 24(5-6): 187-207.
-
Dyer ML, Sallis HM, Khouja JN, Dryhurst S, Munafò MR (2022) Associations between COVID-19 risk perceptions and mental health, wellbeing, and risk behaviours, Journal of Risk Research 25(11-12): 1372-1394.
-
Schneider CR, Dryhurst S, Kerr J, Freeman ALJ, Recchia G, et al. (2021) COVID-19 Risk Perception: A Longitudinal Analysis of Its Predictors and Associations with Health Protective Behaviours in the United Kingdom. Journal of Risk Research 24 (3-4): 294-313.
-
De-Juan-Ripoll C, Chicchi Giglioli IA, Llanes-Jurado J, Marín-Morales J, Alcañiz M (2021) Why Do We Take Risks? Perception of the Situation and Risk Proneness Predict Domain-Specific Risk Taking. Frontiers in Psychology 12: 562381.
-
Mills B, Reyna VF, Estrada S (2008) Explaining Contradictory Relations between Risk Perception and Risk Taking. Psychological Science 19(5): 429-433.
-
Millstein SG, Halpern-Felsher BL (2002) Perceptions of risk and vulnerability. J Adolescent Health 31(1): 10-27.
-
Kasperson RE, Renn O, Slovic P, Brown HS, Emel J, et al. (1988) The social amplification of risk: A conceptual framework. Risk Analysis 8(2): 177-187.
-
Johnson BB (2023) Factors in intention to get the COVID-19 vaccine change over time: Evidence from a two-wave U.S. study, Health, Risk & Society pp: 151-179.
-
Armstrong T (2019) The Human Odyssey: Navigating the Twelve Stages of Life. Ixia Press.
-
Gudykunst WB, Gao G, Schmidt KL, Nishida T, Bond M, et al. (1992) The influence of individualism-collectivism, self-monitoring, and predicted-outcome value on communication in ingroup and outgroup relationships. Journal of Cross-Cultural Psychology 23: 196-213.
-
Lee HO, Boster EJ (1992) Collectivism-individualism in perceptions of speech rate: A cross-cultural comparison. Journal of Cross-Cultural Psychology 23(3): 377-388.
-
Kemmelmeier M, Burnstein E, Krumov K, Genkova P, Kanagawa C, et al. (2003) Individualism, collectivism and authoritarianism in seven societies. Journal of Cross- Cultural Psychology 34(3): 304-322.
-
Krumov K, Larsen K (2013) Cross-cultural psychology: why culture matters. IAP - Information Age Publishing, PO Box 79049 Charlotte, NC 28271 USA.
-
Matsumoto D, Weissman M, Preston K, Brown B, Kupperbusch C (1997) Context-specific measurement of individualism-collectivism on the individual level: The IC Interpersonal Assessment Inventory (ICIAI). Journal of Cross-Cultural Psychology 28(6): 743-767.
-
Singelis TM, Triandis HC, Bhawuk DPS, Gelfand MJ (1995) Horizontal and vertical dimensions of individualism and collectivism: a theoretical and measurement refinement. Cross-cultural Research 29(3): 240-275.
-
Triandis HC (1995) New directions in social psychology: Individualism and collectivism. Boulder CO: Westview Press.
-
Triandis HC, Bontempo R, Villareal MJ, Asai M, Lucca N (1988) Individualism and collectivism: Cross-cultural perspectives on self-in group relationships. Journal of Personality and Social Psychology 54(2): 323-338.
-
Triandis HC, McCusker C, Hui CH (1990) Multimethod probes of individualism and collectivism. Journal of Personality and Social Psychology 59(5): 1006-1020.
-
Hofstede G (1991) Cultures and Organizations: Software of the Mind. London/New York: McGrawHill.
-
Hofstede G (2006) What did GLOBE really measure? Researchers’ minds versus respondents’ minds. Journal of International Business Studies 37: 882-896.
-
Hofstede G (1985) The interaction between national and organizational value systems. Journal of Management Studies 22: 347-357.
-
Daniels MA, Greguras GJ (2014) Exploring the Nature of Power Distance: Implications for Micro- and Macro- Level Theories, Processes, and Outcomes J. Manag 40(5): 1202-1229.
-
Eylon D, Au KY (1999) Exploring empowerment cross- cultural differences along the power distance dimension. International Journal of Intercultural Relations 23(3): 373-385.
-
Gong Z, Swol LV, Xu Z, Yin K, Zhang N, et al. (2019) High- Power Distance Is Not Always Bad: Ethical Leadership Results in Feedback Seeking. Front. Psychol 10: 2137.
-
Zhang K, Wang Y, Tang N (2022) Power distance orientation and perceived insider status in China: a social identity perspective. Asia Pacific Business Review 29(1): 89-113.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis