Epilepsy and Psychiatric Disorders in Children and Teenagers in the Psychiatric Department of the Conakry University Teaching Hospital
Introduction: The purpose of this study was to: determine the prevalence, describe the socio-demographic characteristics of patients with psychic disorders and epilepsy, and highlight the different psychic disorders encountered in epileptic patients. Material and methods: This was a descriptive transverse retrospective study of a duration of ten (10 years) (from January 1, 2013 to December 31, 2022) of all children and teenagers aged 19 and above of any sex and regardless of the origin of epilepsy and psychic disorders monitored in the Department who received an EEG during the study period. Results: The prevalence of epilepsy and psychic disorders in children and teenagers was 12.5%. The average and big adolescence were the most affected about 25.1% and 23%; the medical history of malaria and hyper-pyretic seizures was predominant about 43.7% and 32.2%; for the majority of parents and relatives psychic disorders of epilepsy were synonymous with devil’s disease in 52.5% of cases. The most represented psychic manifestations were behavioral, psychomotor, and language disorders. The temporal seat was the most predominant, representing 51% of cases. Carbamazepine was the most prescribed anti-epileptic drug about 58.5%. Conclusion: A broader study in the general population would be needed for better management.
Introduction
Epilepsy is a set of clinical manifestations associated with the episodic and recurrent occurrence of abnormal discharges of a population, more or less extended, of neurons within neural networks [1]. In fact, we should talk about “epilepsies” as the clinical manifestations, the causes and the repercussions on development are varied [2].
The psychic disorders observed during epilepsies are paroxysmal or critical phenomena (confusional state, crepuscular states, psychomotor automatisms, dream states); inter-critical or sub-acute disturbances (mental confusion, acute delusional psychosis, mood disorders) and permanent mental disorders that mainly concern the personalities of patients with epilepsy [3].
The numerous and varied manifestations are represented by: movements (jerks, tremors, and stiffness), sensitivity and senses disorders (tingling, numbness, auditory and visual hallucinations ...), vegetative disorders (redness of the face, cyanosis of the lips, salivation, loss of urine) and psychic disorders (e.g. anxiety, memory impairment, loss of consciousness).
The diagnosis of epilepsy is essentially clinical, often difficult and poses a problem of differential diagnosis with many psychopathological disorders in children and teenagers. The existence of epilepsy in children and teenagers can disrupt the different lines of their development and cause a disruption of the structure of their personality. It is a source of psychic and socio-economic difficulty [4].
The prevalence of epilepsy is between 6 and 8 per 1000 inhabitants. Hauser W [5] and Dulac O [6] estimate its annual incidence at 1.2 per 1000 hbts in the first year of life and then 0.4 per 1000 population in subsequent years.
The early and severe epilepsies of the child are neurological pathologies for which the somato psychic entanglements were very early emphasized by many authors [7]. In the United States, an epidemiological study conducted in Minnesota shows that 19% of people with newly discovered epilepsy whose age is between 5 and 6 years have learning difficulties and have psychosocial problems [8]. In France, the incidence is related to age with a higher bimodal distribution in children and after 60 years. About 50% of epilepsies begin before the age of 10.
In Africa, authors have been interested in the question, so in Tunisia it is estimated at 6 per thousand the frequency of mental disorders during epilepsy and its average incidence in children is 0.6 to 1.2 for thousand [9]. A prospective study conducted in Togo in 2007 in patients aged at least 18 years reported a frequency of 4.81 ± 0.55 anxiety and 4.42 ± 0.40 depression in subjects with epilepsy Balogou AAK, et al. [10].
In Guinea [11] reported 26.04% of mental disorders of epilepsy in children and teenagers and Cisse A [12] in his doctorate thesis in medicine reported 50% of mental disorders of epilepsy in children.
Epilepsy is the subject of many interpretations according to societies and cultures. Its management requires some skills in the practitioner to make a psychopathological examination, because the choice of antiepileptic drug is not easy, it must rely on many elements that are the age of the child, its development and neurological examination [13].
The objectives of this study were to determine the prevalence of psychic disorders and epilepsy in children and teenagers, to describe the socio-demographic characteristics of patients, to highlight the various psychic disorders encountered.
Patients and Methods
We conducted a descriptive and transversal retrospective study of a duration of ten (10) years from January 1, 2013 to December 31, 2022, in the Psychiatry Department of the Donka National Hospital, Conakry University Teaching Hospital.
During the study period 1465 children and teenagers were seen in consultation among whom 183 had psychic disorders and epilepsy. Included in our study were all children and teenagers up to the age of 19, of any sex, and regardless of the origin of epilepsy and psychic who received an EEG during the study period. Data were collected from the registers (consultation and hospitalization) and individual patient files. The study was based on children’s and teenagers files received during the study period for epilepsy and psychic disorders.
Results
The prevalence of psychic disorders in children and teenagers was 12.5%. The middle adolescence was the highest age represented 25.10%, followed by the late adolescence 23% and the early adolescence 21.30% (Figure 1).
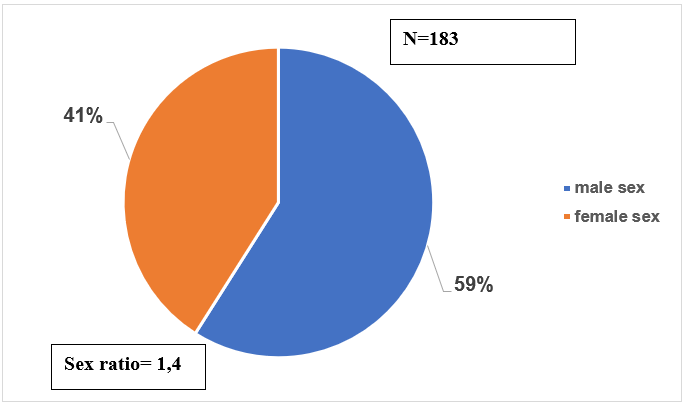
Concerning sex, we noted a male predominance 59% against 41% female with a sex ratio Male / Female equal to 1.4 (Figure 2).
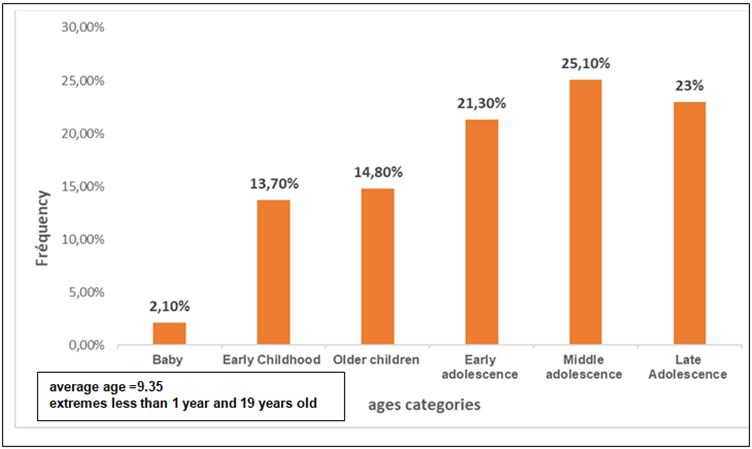
Figure1: Distribution of the 183 patients followed in psychiatry for epilepsy and mental disorders from January 1, 2013 to December 31, 2022 by age.
| Origin | N | % |
|---|---|---|
| City of Conakry | 136 | 74,3 |
| Lower Guinea | 20 | 10,9 |
| Middle Guinea | 15 | 8,2 |
| Upper Guinea | 8 | 4,4 |
| Forest Guinea | 4 | 2,2 |
| Total | 183 | 100 |
Table 1: Distribution of the 183 patients followed in psychiatry for epilepsy and mental disorders from January 1, 2013 to Decemb
In terms of origin, the majority of our patients came from the city of Conakry equivalent to 74.4% of cases, followed by other regions, Lower Guinea (10.9%), Middle Guinea (8.2%), Upper Guinea (4.4%) and Forest Guinea (2.2%) (Table 1).
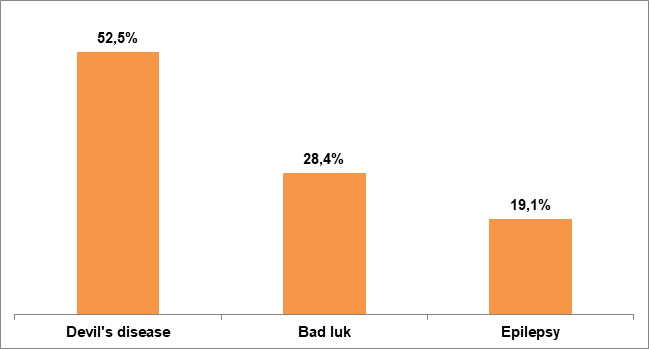
According to psychic disorders associated with epilepsy, we noted a predominance of psychomotor disorders (39.9%), language disorders (26.8%), perceptual disorders (18%) and sphincteric control disorders (13.6%). At the evolution level before the first consultation, the majority had an evolution between 1- and 5-years equivalent to 50.3% followed 26,8% which had an evolution higher than 5 years. Among the clinical forms, secondary generalized epilepsy was the most common clinical form 64.5%, followed by primary secondary generalized epilepsy 21.9%. Depending on the seat of the lesion, the temporal seat was the most recovered, i.e. 51% of cases, followed by the frontal seat 31%. Permanent mental disorders were the most predominant at 53%, followed by critical mental disorders (27.9%) and intercritical mental disorders (15.3%) ; Intellectual disability and depression were the most common comorbidities, respectively 12.6% and 7.1%. Regarding cultural interpretation, in 52.5% of cases the disease was considered to be due to devils, 28.4% as a bad luck. Meat was the most prohibited mentioned food 20.2% of cases followed by other associations 14.2% (Figure3).
In the majority of cases there was no food ban 38.3% against 20.2% where meat was prohibited, 10.4% milk, 10.4% okra, 6.5% bananas (Table 2).
| Forbidden food | N | % |
|---|---|---|
| No forbidden | 70 | 38,3 |
| Meat (mutton, goat, chicken) | 37 | 20,2 |
| Milk | 19 | 10,4 |
| Okra | 19 | 10,4 |
| Banana | 12 | 6,5 |
| Food Association | 26 | 14,2 |
| Total | 183 | 100 |
Table 2: ** Distribution of the 183 patients followed in psychiatry for epilepsy and mental disorders according to the forbidden
Others ** (palm oil, cassava leaf, lemon, spices). Table 2:** Distribution of the 183 patients followed in psychiatry for epilepsy and mental disorders according to the forbidden food.
Discussion
During the study period 1465 children and teenagers were seen in consultation among whom 183 had psychic disorders and epilepsy, a prevalence of 12.5% oriented towards traditional healers (healers, marabouts) than towards modern medicine. -No age group is exempted during epilepsy and mental disorders. However, teenagers were the most affected.
Marcelli D [4] reported that epilepsies appear at the end of adolescence with a frequency of 70%. This predominance of the seizures appearance in the adolescence period may be explained by the hormonal changes that occur during this period of psychological development and may be responsible for triggering certain seizures.
Both sexes were affected with a male predominance [15]. This predominance is explained by the fact that psychopathological disorders of the child are common in boys rather than girls on the one hand and, on the other hand, the under-declaration of epilepsy in girls when they are at the age of getting married [16].
-Epilepsy and psychic disorders can be found in all environments but their predominance in the city of Conakry could be explained by the presence of the child psychiatry unit. -The origin of its academic difficulties is certainly multi- factorial, the socio-familial context on the one hand, and the cognitive difficulties encountered a decrease in the speed of processing information and working memory, especially in demand situations as well as any attention control issues. This predominance of mothers with no education and low educational level could be explained by the influence of the customs and traditions that hinder girls’ schooling and those who go to school drop out of school to devote themselves to household activities.
Like most child health problems, children with epilepsy were accompanied by their mothers. In Mali Maiga Y, et al. [17], in a community study on the knowledge and attitude of epileptic children’s parents reported that 61% of patients were accompanied by their mothers. The predominance of mothers accompanying their children reflects the traditional role in our society of women alongside children and especially those who are sick to provide psychosocial support.
-This high frequency of patients who had an evolution before the 1st extended psychiatric consultation of (1-5 years or more) could be explained by the erroneous cultural interpretation which surrounds epilepsy and which leads to a therapeutic wandering. The use of specialized structures is late.
Secondary and primary generalized epilepsies were the most common types of epilepsy in our patients.
Cissé A [12] and Condé S [11] reported respectively 47% and 43% of primary generalized epilepsy. According to Marcelli D [4] primary generalized epilepsy characteristic of the big child and the teenager is always cryptogenic and its prognosis is quite favorable. Secondary generalized epilepsy is essentially represented by West syndrome and Lennox Gastaut is a provider of major behavioral disorder.
This high frequency of secondary generalized epilepsy could be explained by the duration of the study and the size of the sample on the one hand and on the other hand because of the delay in the treatment (1 to 5 years) some forms of partial or focal epilepsy that can generalize secondarily.
Regarding the comorbidity more than half of our patients had no comorbidity. According to some authors Beauschen H, et al. [18] and Association of CHI Poissy [19] statistical assessments of psychiatric disorders are extremely variable, depending both on the recruitment criteria and the criteria for assessment. Nevertheless, all epilepsies appear to have about 50% psychiatric morbidity compared to 21% in the general population.
The interest in the study of mental disorders of epilepsy is steadily increasing due to significant progress in a number of areas De Toffol B [20]. Epileptic disorders can have many relationships with psychiatric disorders (depression, anxiety) Venault P, et al. [21] and Verceuil L [22]. Whatever disease, it is impossible to detach it from the social and cultural context in which it comes. Each community has a particular vision which has a repercussion on the answers provided, that is to say on the support. Thus in our study epilepsy was considered by the parents of patients and their relatives as a disease of the devil or a bad luck child, this interpretation varies from one community to another.
In Senegal, in the investigation of Adotevi and Stephanie conducted among the Wolofs, it appears that epilepsy is related to an attack by a jinn (spirit) that often manifests itself as a whirlwind of wind. A supernatural cause is given to Cameroon [23].
Given the importance of our customs and the misinterpretation of epilepsy, some foods are incriminated in genesis or considered as triggers. That is why in our study sheep, goat, chicken, okra, milk, and banana meat were forbidden foods with our patients. Food taboos observed during epilepsy are an African peculiarity that varies from one region to another and from one community to another.
Thus, in Togo, goat meat, chicken meat, fish, food used during ceremonies, food and water having stayed for more than one day in the concession are forbidden to epileptics [24]. In Wolof community, sticky foods are forbidden to epileptics.
Traoré H, et al. [25] in Mauritania noted that too spicy, too salty foods were considered to cause epilepsy while Avode D, et al. [26] in Benin, the traditional healers considered that the combination of these salty foods with red oil beans and red beans decreased the effectiveness of their therapy, hence their prohibition.
Regarding the therapeutic route, the majority of our patients resorted to a mixed treatment (modern and traditional). In sub-Saharan Africa the treatment of epileptics is closely linked to the socio-cultural representation of this pathology.
In the Republic Central Africa, Preux, et al. [23] reported that 35.8% of their patients received modern treatment, 28.3% traditional treatment and 11.2% under mixed treatment. Adriantseheno LM, et al. [27] in Antanarivo found that 66.2% of the patients consulted a doctor and 26.2% went to the traditional practitioner or the religious.
This high frequency of mixed treatment in our study can be explained on one hand by the fact that the therapeutic route always begins with the traditional therapists and with the recurrence of the crises, the opinion of the doctors is solicited, on the other hand the parents of epileptics are looking for a definitive solution to the problems, hence the combination of the two types of treatment.
-As for the management of our patients, Carbamazepine was the most used antiepileptic drug and Clonazepam was the tranquillizer the most associated with antiepileptic drugs, ie 27.3%. Diop AG, et al. [38] in a study of the care chain in Africa noted that phenobarbital was prescribed in 57-85% of cases in intertropical Africa [29] in rural India noted that 50% of epileptics were on phenobarbital, and in other countries such as Zimbabwe, India, and Mali, phenytoin was the most prescribed [30]. The use of phenobarbital appears to be conditioned by economic factors, its availability rather than its efficacy and relevance Commission (III and IV) on Antiepileptic Drugs of the International League Against Epilepsy. Availability and Distribution of Epileptic Drugs in Developing Countries Epilepsia [31]. The high frequency of the prescription of carbamazepine and sodium valproate in our study is explained by their indication and by their accessibility (Carbamazepine on the national list of essential drugs) but also by their efficiency.
Conclusion
Although epilepsy is a chronic neurological pathology, it is associated with psychiatric disorders that often cause physical and mental disability in children and adolescents. We found a prevalence of 12.5% of epilepsy and psychic disorders in children and adolescents. The average adolescence was the most affected with a male predominance. Most of our patients came from the city of Conakry. Primary education and patients with no referral source were the most represented. The majority of cases had a history of malaria and hyper pyretic convulsions. This condition, often a source of academic difficulties, leads to major disorders generally interpreted by the entourage as a supernatural phenomenon or devil, hence the delay in medical care. The permanent and critical mental disorders were the most represented and the EEG was the complementary reference examination for all patients. In view of all these factors, a broader study of the social and cultural aspects of the general population would be necessary to improve treatment [32, 33, 34, 35, 36, 37].
Conflicts of Interest
The authors state that they have no conflicts of interest.
References
-
Auclair L, Jambaque I, Sieroff E, Dulac O, Laberge D (2003) Preparatory Attention and Frontal Epilepsy in School-Aged Children. New Data in Epileptic Children ANAE 74-75: 210-218.
-
Bulteau C, Jambaque I, Viquier D, Kieffer V, Dellatolas G, et al. (2000) Epileptic Syndrome, Cognitive Assessment and School Placement: A Study of 251 Children. Dev Med Child Neurol 42(5): 319-27.
-
Guelfi JD, Patrice B, Silla C, Rene OM (2007) Basic Punch. University Press of France December Page pp: 286-288.
-
Marcelli D (1996) The Ages of Life In: 10th (Edn). Elsevier Masson.
-
Hauser W (1991) Prevalence and Incidence of Convulsive Disorders in Children. Epilepsia 35: 1-6.
-
Dulac O (1991) Epilepsies and Seizures: EMC 4091(A10): 27.
-
Beauchesnes H (1976) Epileptic children and adolescents. A clinical and psychopathological approach. Psychiatr Enfant 19(2): 429-494.
-
Trosle JA, Hauser WA, Sharbrough FW (1989) Psychological And Social Adjustment To Epilepsy In Rochester, Minnesota. Neurology 39(5): 633-637.
-
Jammoussi A (1982) Contribution to The Study Of Epilepsy In Tunisia. About 591 Cases Followed In Hospital. Phd Thesis In Medicine, Tunis, Africa.
-
Balogou AK, Assogba K, Agbobli A, Djassoa G, Grunitzky EK (2010) Anxiety, Depression and Quality of Life of Epileptics in Urban Areas in a Developing Country: Togo. Epilepsies 22(1): 79-83.
-
Conde S (2004) Epidemiological and Clinical Aspects of Mental Disorders of Epilepsy in Children and Adolescents in the Psychiatric Ward of Conakry University Hospital. Conakry, pp: 76.
-
Cisse A (2009) Epidemiological Aspects and Diagnosis of Mental Disorders of Epilepsy in Children in the Psychiatric Ward of the Donka National Hospital, Conakry University Teaching Hospital pp: 68.
-
Motte J (1997) Practical Conduct of Anti-Epileptic Treatment in Children and Pediatric. Paris 44(1): 59-68.
-
Vuillemier P, Jallon P (1998) Epilepsy And Psychiatric Disorders: Epidemiological Data. Neurological Review (Paris) 154(4): 305-317.
-
Ey H, Al (2010) Epilepsy- Epileptics; In: Manual of Psychiatry 6th (Edn.), Masson pp: 273.
-
Woman and Epilepsy (2012) Edmonton Epilepsy Association.
-
Maiga Y, Napon C, Dicko F, Fofana T, Traore B, et al. (2008) Knowledge about Epilepsy and Attitudes of Child Parents in Mali: A Community Study. Neurological Review I64 (SA49-A91): (A15).
-
Beauschene H, Broussarr G (1995) Epilepsy in Children In Lebovici S.
-
Association of Continuous Medical Training of Chi De Poissy and Poissy Ville (1987) Seminar of Neurology and Psychiatry. Epilepsy, Some Simple Questions ... Answers That Try To Be. Review -Prat 57-65.
-
Toffol B (2005) Epilepsy And Psychiatry. Epilepsy 17: 3.
-
Venault P, Chapoutier G (2005) Relationships Between Psychiatric Disorders and Epilepsy: the Contribution of Studies on Rodents. Epilepsy 17: 4-9.
-
Vercueil L (2005) Psychopathology of Pharmaco- Resistant Partial Epilepsies. Epilepsy 17: 10-16.
-
Preux PM (2000) Contribution to Epidemiological Knowledge of Sub-Saharan Epilepsy. Phd Thesis in Public Health, University of Limoges pp: 395.
-
Grunitzky Ek, Balogou Aak, Dodzro Ck (1998) Clinical and Epidemiological aspects of Traditional Therapeutic Sarifications in Epileptics in Togo. Bull Soc Pathol Exot 93(4): 251-254.
-
Traore H, Diagana M, Debrock A, Baa, Algad B, Preux Pm (1998) Socio Cultural Approach of Epilepsy in Mauritania. Med Trop 58(4): 365-836.
-
Avode Dg, Houinato D (2000) Cultural Factors and Epilepsy in Benin. Rev Neurol 156: 64-66.
-
Adriantseheno LM, Rakotoariuony MC (1998) Sociocultural Aspects of Epilepsy in Malagasy. C.A.P Survey done in Antananarivo. Bull Soc Pathol Exot 93(4): 247-250.
-
Diop AG, Ndiaye M, Diagne M, Thiam A, Sene Diouf F, Diallo AK (1988) Antiepileptic Care Lines in Africa. Epilepsy 10: 115-121.
-
Mani KS, Rangan G, Srimivas HV, Soundharan VS, Subbakrihna DK (2001) Epilepsy Control with Phenobarbital or Phenytoin in Rural South India: The Yelandur Study. The Lancet Neurol 357: 1316-1320.
-
Uchoa E, Corin E, Bibeau G, Koumare B (1993) Cultural Representations and Social Disqualification. Epilepsy in Three Ethnic Groups in Mali. Psychopathology Africa 25: 33-57.
-
(1985) Commission (3&5) On Antiepileptic Drugs of the International League Against Epilepsy. Epileptic Drugs in Developing Countries. Epilepsia 26: 117-121.
-
Villeneuve N, Laguitton V, Mancini J (2004) Evaluation of the Schooling.
-
Doukoure M, Soumaoro K, Samoura M, Saint Andre S, Te Bonle M, et al. (2008) Epidemiological and Clinical Aspects of Child Psychosis at the Conakry Psychiatry Department. Medical Guinea 62: 1-7.
-
Loiseau P, Jallon P (1984): Epilepsies 3rd Edition; Paris; Masson.
-
Ngoungou Eb, Dulac O, Poudiougou B, Druet-Cabanac M, Dicko A, et al. (2006) Epilepsy As A Consequ Ence Of Cerebral Malaria In Mali West Africa. Epilepsia 45(5): 873-879.
-
Rutter M, Graham P, Yutte W (1970) A Neuropsychiatric Study in Childhood Hood Clinics in Developmental Medicine Nos. 35 -36 London: S.I.M.P With Heinemann Medical.
-
Fleury V, Vercueil L, Minotti Al (2004) Ictal Compulsive Obsessive Behavior: Intracranial Study. Epilepsia 45 (Addition 3): 13.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis