Seroprevalence, Epidemiology and Genetic Characterization of Hepatitis C Virus, India
Hepatitis C virus (HCV) causes serious hepatic manifestations viz. chronic liver cirrhosis, necrosis and hepatocellular carcinoma. Globally 3% of the population is highly affected by HCV infection. A total of 751 HCV suspected samples collected from Primary Health Care centres, both from Private and Government hospitals in Tamil Nadu were screened with anti HCV antibodies-ELISA test revealed a prevalence of 0.5% of the population to have HCV diseases burden in different age groups. The pediatric age groups (1-5 and 6-12 years) were predominantly HCV affected and statistical analysis (student t-test) of the data revealed the significant differences between the age groups. The 28% of the blood transfusion cases showed HCV infections, followed by haemodialysis (12%), intravenous drug abuse (02%), tattoos and piercing (01%), sexual contact and abusement (08%), plasmapheresis (08%), contact to HCV infected material (01%), perinatal (02%), intravenous immunoglobulin treatment (03%), transplantation (18%) and unknown (17%). The predominant symptoms of HCV infection were jaundice (90%), fever (60%), dark urine (48%), hepatomegaly(35%), andspleenomegaly (20%). A severe impact of the Hepatitis C virus infections was on the biomarkers viz. bilirubin, SGOT, and SGPT which were found to be significantly elevated. The elevated levels of total bilirubin were 70%, serum glutamine oxalo transaminase (SGOT) (60%), serum glutamate pyruvic transaminase (SGPT) (60%), alkaline phosphatase (55%) and albumin (49%). Nested PCR amplification of the genomic RNA of the virus isolated from blood plasma samples of ELISA positive HCV cases yielded specific amplicons. The outer region primers of the HCV core protein yielded precise products of 417 bp while the inner region primers yielded 343bp of amplicons which confirmed the occurrence of HCV infections. The transfusion of blood and products between the donors and recipients are the chief sources and factors of HCV transmission in the population and therefore appropriate precautionary measures are paramount in the prevention of the HCV infections.
Introduction
Hepatitis C virus induced hepatocellular carcinoma and chronic liver infection is one of the major communicable diseases [1]. Nearly 200 million people are carriers of Hepatitis C virus, and 3.3% of world population has HCV infection [2]. The chronic hepatic C Virus infected patients have characteristic symptoms such as yellowish urine, severe upper abdomen pain and nausea, fatigue and muscle aches, persistent chronic hepatitis, fibrosis and liver cancer [3.4]. Hepatitis C virus infection has incubation period of 6 to 8 months and that causes mortality of thousands of people every year. Hepatitis C virus is classified into Non-A and Non-B types. It is a positive sense RNA virus belonging to the family Flaviviridae and genus Hepacivirus. Hepatitis C virus is highly variable and it’s genome has been classified into 6 variable genotypes [5]. Genotype 1, 2 and 3 are commonly distributed in all parts of the world. The 1a and 1b genotypes of the Hepatitis C virus are not only widely spread in Europe, USA and Japan and recently these subtypes are also found to occur in Tamilnadu, India [6]. The genotype 4 of the Hepatitis C virus is also expressed in Middle East and Central Africa. The genotype 5 of the Hepatitis C virus is found in South Africa while the genotype 6 has recently been identified in the South East Asia [7, 8]. The genome of Hepatitis C virus consisted of 2 essential regions viz., structural and nonstructural regions. The other essential regions of the Hepatitis C virus genome include core and envelope proteins and untranslated regions. The Hepatitis C virus infection was found in patients at acute and chronic stages of infection. The acute stage of Hepatitis C virus infections are known to be asymptomatic [9, 10]. In contrast, the chronic Hepatitis C virus infections were symptomatic jaundice with fever while HCV were failed to cause fulminant in immunocompetant patients. The patients with chronic Hepatitis C virus can lead to the development of liver cirrhosis [11]. However the chronic cirrhosis patients shall have high risk of progression on hepatocellular carcinoma [12]. The evaluation of the HCV prevalence in different age groups and gender over a period of time will clearly indicate the extend of spread of the HCV diseases burden which may in turn help to treat and control the disease and lead to development of necessary steps to solve the HCV issues. In view of the seriousness and importance of the HCV infections, the present study was undertaken to reckonate the seroprevalence of HCV in both sexes and different age groups of patients in and around Chennai, India from January to December 2014. Furthermore “ELISA”, nested PCR characterization of the core polypeptide gene was employed as a marker for HCV diagnosis.
Materials and Methods
Study Population
In the present study, HCV suspected samples were collected from patients who were admitted in antenatal clinics at government/ private hospitals in and around Chennai, as well as from other neighbouring districts, Tamil Nadu, India and appropriate HCV diagnostic tests were performed for the detection of the disease from January to December 2014. A total of 751 serum and plasma samples were collected from the highly suspected patients. Complete details of aetiology of patients such as physical examination, age, sex, contact history, date of onset of the symptoms of the disease, occupation and other risk factors were also recorded from the patients, with the help of lab request form (LRF). The Patients were segregated into different age groups in years viz. 0-1, 1-5, 6-12, 13-18, 19-30, and 31-45 and above 45. Data were analysed on the basis of gender, age and month wise distribution of samples in the year 2014.
Sample Processing
Serum and plasma from each of these blood samples from the patients were separated by centrifugation at 2000 rpm for 10 min. Each serum and plasma sample was properly labeled and stored at −20°C and −80°C respectively.
Enzyme Linked Immune Sorbent Assay (ELISA)
Serum samples from the patients were used to test for the presence of HCV IgG antibodies with kits obtained from Microlisa, India. ELISA tests were performed as per the manufacturer’s instructions. The high and low optical density of the antibody titre with the HCV suspected serum samples were determined and interpreted. High titre ELISA positive HCV cases were chosen for the viral RNA extractions in blood plasma of patients and were used for nested PCR tests.
RNA Extraction and Nested PCR
HCV viral (genome) RNA extractions from Plasma samples were done by using QIA amp Viral RNA extraction KIT (Qiagen), Germany. Further the presence of HCV in the blood plasma patients was confirmed by PCR tests by using nested PCR primers specific for HCV core protein genes. The PCR primers consisted of the conserved nature of these sequences. They are: Sc2- 5’GGGAGGTCTCGTAGACCGTGCACCATG3’ and Ac2- 5’GAG(AC)GG(GT)AT(AG)TA CCCCATGAG(AG)TCGGC3’ were the sense and antisense outer primers for the core region, respectively. S7-5’AGACCGTGCACCATGAGCAC 3’ and A5-5’TACGCCGGG GGTCA (TG) T(GA) GGGCCCCA 3’ were the sense and antisense primers, for the inner region primers for PCR were used to generate the amplicon for sequencing [13, 14, 15, 16, 17, 18]. The isolated viral RNA was processed with random hexamers which were found to be more efficient and primer specific to the 5'-UTR and reverse transcriptase. This was carried out using Maloney Murine Leukemia Virus Reverse Transcriptase (M-MLV RT; Promega) RT- PCR reactions were assembled as per manufacturer's instructions employing a constant amount of HCV RNA (10 μl of RNA in a 50 μl reaction) due to high percentage of GC content in HCV. The incubation temperature 45°C - 50°C were used for the conversion of cDNA synthesis. Synthesized cDNA was amplified with first set of HCV specific primers using 5μl template and then 1μl of the PCR product was used for a second round of amplification using HCV specific nested primers. Cycling conditions of the first-round PCR consisted of 35 cycles of denaturation at 94° C for 60 sec, annealing temperature at 53° C for 60 sec, and extension was at 72° C for 60 sec. The second PCR test was performed with 40 cycles of denaturation at 94° C for 45 sec, annealing at 53° C for 45 sec, and extension at 72° C for 45 sec. Carry over contamination was prevented as described by Kwok & Higuchi method 1989. PCR products were analyzed in 1.5% agarose gel electrophoresis. The gel was viewed under Alpha Imager (AlphaInnotechSan Diego, California, USA) and the resulting bands were captured with a Polaroid camera. In HCV infected patients, the liver function tests especially the predominant biomarkers viz. total bilirubin was determined by Malloy and Evelyn method, 1937 [19], Serum glutamine oxalo transaminase (SGOT) and Serum glutamate pyruvic transaminase (SGPT) was determined by Reitman and Frankel (1975) [20], Alkaline phosphatase and albumin were determined by Kind and King (1971) [21].
Statistical Analysis
The data obtained in the present study were statistically analyzed by the software SPSS.20 IBM version. Specific type distribution was assessed by Student t-test and standard deviation of sex, age, month- season wise and HCV positive samples were also performed.
Results and Discussion
A total of 751 HCV suspected blood samples was screened for the occurrence of Hepatitis C virus from January to December 2014 and the results of HCV susceptibility and distribution in males and females (gender), and different age groups, are presented in Figure 1.
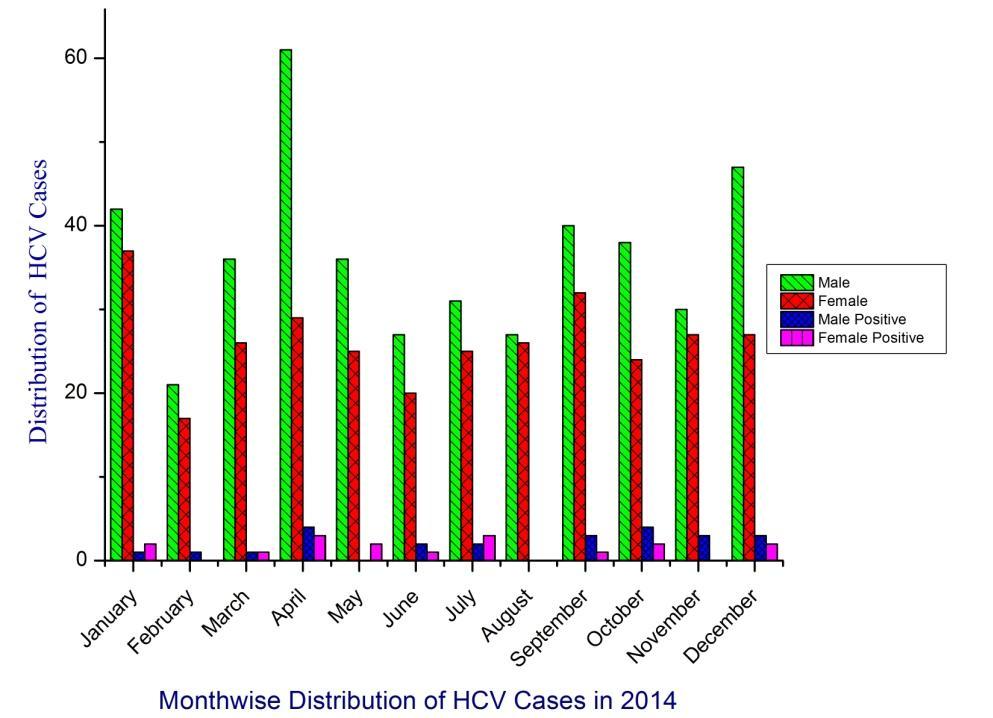
The overall susceptible case of Hepatitis C virus was found to be relatively more in the months of January, April and December 2014. The month wise analysis of HCV distribution was statistically analyzed by using the student t-test which has shown the distribution frequency to be significant and attained a value of 6.2±4.2 where the hypothesis was accepted as shown in the Table 1.
| One-Sample Test | |||||
|---|---|---|---|---|---|
| Parameters | Test Value = 0 | ||||
| t | Df | Sig. (2-tailed) | |||
| Month | 6.245 | 11 | 0 | ||
| Male | 11.813 | 11 | 0 | ||
| Female | 17.702 | 11 | 0 | ||
| Positive Male | 4.899 | 11 | 0 | ||
| Positive Female | 4.529 | 11 | 0.001 | ||
| 0 to 1 Yrs | 7.301 | 11 | 0 | ||
| 1 to 5 Yrs | 9.946 | 11 | 0 | ||
| 6 to 12 Yrs | 13.188 | 11 | 0 | ||
| 13 to18 Yrs | 2.862 | 11 | 0.015 | ||
| 19 to 30 Yrs | 3.532 | 11 | 0.005 | ||
| 31 to 45 Yrs | 4.241 | 11 | 0.001 | ||
| Above 46 Yrs | 5.206 | 11 | 0 |
Table 1: [INLINE_TABLE:3:0]
In the gender wise distribution, the male susceptible cases were elevated in the month of April and October. Similarly, the female gender cases for HCV were high in January, April and September. The statistical analysis of gender wise student t-test attained 11.8±2.9 and the hypothesis is statistically significant between male and female gender (17.7±2.2). The age wise distribution of suspected cases were segregated into 0-1,1-5,6-12,13- 18,19-30,31-45 years and above 45 years and the data are detailed in figure 1. The total number of HCV negatives was higher in the month of January, April, September and December. Among the age group 6-12 yrs, the numbers of HCV positives cases were very high, especially notable in the number of cases during the month of January, September and December. The other age group 19-30, 31-45 and above 45yrs showed a very high number of positive cases which were observed only in the month of April while in the rest of the months showed no significant number of HCV positive cases (Figure 2).
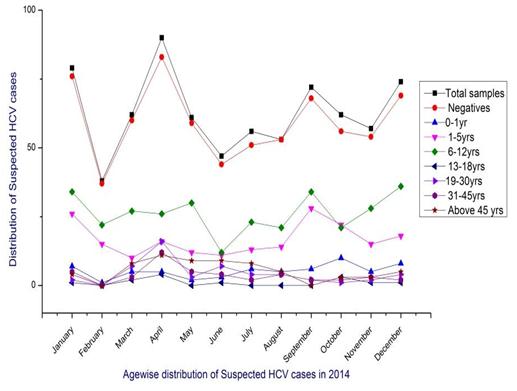
The statistically analyzed age wise frequency distribution of HCV cases, are shown in Table 1. The t-test values of the segregated age groups were attained as standard deviation 0-1 (7.3±1.5), 1-5 (9.9±1.6), 6-12 (11.1±2.6), 13-18 (2.8±1.0), 19-30 (3.5±1.3), 31-45 (4.2±1.6) and above 45 yrs (5.2±1.4). The sources and factors of HCV infections in all 751 patients were analyzed and calculated as percentage and the data are presented in Table 1. The factors such as blood transfusion among the hospitals hold 28%, haemodialysis (12%), intravenous drug abuse (02%), tattoos and piercing (01%), sexual contact and abusement (08%), plasmapheresis (08%), contact to HCV infected material (01%), perinatal (02%), intravenous immunoglobulin treatment (03%), transplantation (18%) and unknown (17%). Similarly the predominant symptoms of HCV virus infected patients are presented in Table 2. The results show that (90%) patients had jaundice, followed by (48%) dark urine, (60%) fever, (35%) hepatomegaly and (20%) spleenomegaly (Table 3).
| Sl.No. | Sources | Percentage of patients | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | Blood Transfusion and related products | 38 | ||||||
| 2 | Hemodialysis | 12 | ||||||
| 3 | Intravenous Drug abuse | 2 | ||||||
| 4 | Tattoos & Piercing | 1 | ||||||
| 5 | Sexual Contact | 8 | ||||||
| 6 | Plasmapheresis | 10 | ||||||
| 7 | Contact of HCV contaminated Material | 1 | ||||||
| 8 | Perinatal | 2 | ||||||
| 9 | Intravenous Immunoglobulin | 3 | ||||||
| 10 | Transplantation | 20 | ||||||
| 11 | Unknown | 28 | ||||||
| S | l.N | o | Symptoms | Percentage of patients | ||||
| 1. | Jaundice | 90 | ||||||
| 2. | Fever | 60 | ||||||
| 3. | Dark Urine | 48 | ||||||
| 4. | Hepatomegaly | 35 | ||||||
| 5. | Spleenomegaly | 20 |
Table 2: Symptoms and prevalence of Hepatitis C virus. The results of the liver function tests indicated a severe impact of the H

Figure 3: Liver function profiles of Hepatitis C virus manifestations. The total bilirubin observed was 70%, serum glutamine oxalo transaminase (SGOT) (60%), serum glutamate pyruvic transaminase (SGPT) (60%), alkaline phosphatase (55%) and albumin (49%). The liver parameters especially the total bilirubin and enzymatic parameters SGOT, and SGPT were found to be significantly elevated in the HCV infected patients. RNA of the HCV genotype isolated from the ELISA positive plasma samples were amplified with RT-PCR followed by nested PCR. There were 41 HCV ELISA positive cases which were also PCR positive and in these cases, the amplicon of HCV core protein region were amplified in the 5’ prime untranslated regions of the genome. The amplicons were profiled with the agarose gel electrophoresis as shown in Figure 4.
![Figure 4: PCR amplification of 343 & 417 bp core protein gene from Hepatitis C virus. M-Molecular (DNA-1Kb) ladder, S1 and S2 shows PCR amplified products 417 and 343 bp, S3 shows absence of amplified products, PC-Positive control shows amplified products and absent in negative control (NC) In all 15 samples, nested -PCR products were successfully amplified and consisted of a smaller 343 bp fragment corresponding to the inner primer pairs and also a larger 417bp fragment corresponding to the outer pair of primers of the viral core protein gene. Figure 4 shows two high positive cases with one negative sample which were also profiled along with positive and negative controls. In Tamil Nadu, India, the Hepatitis C virus is shown to be one of the most predominant viruses of the hepatitis group. The present study has shown the risk factors that influence the infection of hepatitis virus. They were the transfusion of blood and related products and transplantation which were found to be highly significant and higher in HCV infections than that of the other associated parameters. Similar such studies that were carried out in Brazil showed that the parameter blood transfusion alone was the highest positive risk factors for the transmission of the HCV [22]. The prevalence of the HCV infection in the sample population was evaluated in the age groups and was further identified and validated the most important risk factors that concerns in the epidemiology and etiology of Hepatitis C virus infection [23]. The present study revealed that the association of the HCV infections with that of the susceptibility factors, age, sex and symptoms. The student t-test and one sample univariate analysis of the data showed occurrence of significant differences between the groups. The age groups 1-5 and 6-12 years old pediatric patients in Tamil Nadu, India were shown to be the most susceptible age groups and to exhibit a higher positivity to anti-HCV antibody. In contrast, none of the other age groups exhibited such significant HCV infections within the groups. In the present study, the prevalence of HCV susceptibility was relatively very high in the month of April 2014. Moreover the study has shown statistically significant gender wise distributions. A high positivity of HCV infections was found in the males than in the females. These findings indicated that the susceptibility factors and possibilities of HCV transmission were very high possibly due to the impact of unique genetic factors, social behavior and frequent local migration and interaction of the hosts. Previous studies in Italy, reported a high positivity of HCV infections in the age group of above 45 years [24-26]. Subsequently some of the studies indicated that the migration of hosts didn’t influence the HCV transmission in susceptible cases [27]. In the present study, the factors and sources of Hepatitis C virus were so important for the transmission and infection. Among the factors the present study revealed that the transfusion of blood and related products were significantly important as a major lead factor/ in the HCV infection in Tamil Nadu, India. Likewise the predominant symptoms of HCV infection were found to be that of the fever and Jaundice which were shown to be statistically significant symptoms for the HCV infection [28,29]. Finally the present study portrays the development and use of biomarkers for the diagnosis of HCV infections. The 417bp and 343bp core region sequences of the RNA of the HCV 1b genome was identified to be unique in the Tamil Nadu, India which need further studies. The ELISA positive cases were further confirmed by core protein gene amplification the HCV positive cases were found to be confirmed by this core protein gene PCR amplification. Thus the core protein gene sequence 417bp and 343bp is strongly recommended for Nested PCR amplification to identify and diagnose the HCV infections. Eventually the investigation also suggests that the appropriate government agencies should take up the issue of HCV infections and diseases manifestation in different age groups and to provide awareness to all the people and community.](/fulltextimages/682/fig_4.jpeg)
Figure 4: PCR amplification of 343 & 417 bp core protein gene from Hepatitis C virus. M-Molecular (DNA-1Kb) ladder, S1 and S2 shows PCR amplified products 417 and 343 bp, S3 shows absence of amplified products, PC-Positive control shows amplified products and absent in negative control (NC) In all 15 samples, nested -PCR products were successfully amplified and consisted of a smaller 343 bp fragment corresponding to the inner primer pairs and also a larger 417bp fragment corresponding to the outer pair of primers of the viral core protein gene. Figure 4 shows two high positive cases with one negative sample which were also profiled along with positive and negative controls. In Tamil Nadu, India, the Hepatitis C virus is shown to be one of the most predominant viruses of the hepatitis group. The present study has shown the risk factors that influence the infection of hepatitis virus. They were the transfusion of blood and related products and transplantation which were found to be highly significant and higher in HCV infections than that of the other associated parameters. Similar such studies that were carried out in Brazil showed that the parameter blood transfusion alone was the highest positive risk factors for the transmission of the HCV [22]. The prevalence of the HCV infection in the sample population was evaluated in the age groups and was further identified and validated the most important risk factors that concerns in the epidemiology and etiology of Hepatitis C virus infection [23]. The present study revealed that the association of the HCV infections with that of the susceptibility factors, age, sex and symptoms. The student t-test and one sample univariate analysis of the data showed occurrence of significant differences between the groups. The age groups 1-5 and 6-12 years old pediatric patients in Tamil Nadu, India were shown to be the most susceptible age groups and to exhibit a higher positivity to anti-HCV antibody. In contrast, none of the other age groups exhibited such significant HCV infections within the groups. In the present study, the prevalence of HCV susceptibility was relatively very high in the month of April 2014. Moreover the study has shown statistically significant gender wise distributions. A high positivity of HCV infections was found in the males than in the females. These findings indicated that the susceptibility factors and possibilities of HCV transmission were very high possibly due to the impact of unique genetic factors, social behavior and frequent local migration and interaction of the hosts. Previous studies in Italy, reported a high positivity of HCV infections in the age group of above 45 years [24, 25, 26]. Subsequently some of the studies indicated that the migration of hosts didn’t influence the HCV transmission in susceptible cases [27]. In the present study, the factors and sources of Hepatitis C virus were so important for the transmission and infection. Among the factors the present study revealed that the transfusion of blood and related products were significantly important as a major lead factor/ in the HCV infection in Tamil Nadu, India. Likewise the predominant symptoms of HCV infection were found to be that of the fever and Jaundice which were shown to be statistically significant symptoms for the HCV infection [28, 29]. Finally the present study portrays the development and use of biomarkers for the diagnosis of HCV infections. The 417bp and 343bp core region sequences of the RNA of the HCV 1b genome was identified to be unique in the Tamil Nadu, India which need further studies. The ELISA positive cases were further confirmed by core protein gene amplification the HCV positive cases were found to be confirmed by this core protein gene PCR amplification. Thus the core protein gene sequence 417bp and 343bp is strongly recommended for Nested PCR amplification to identify and diagnose the HCV infections. Eventually the investigation also suggests that the appropriate government agencies should take up the issue of HCV infections and diseases manifestation in different age groups and to provide awareness to all the people and community.
Conclusion
In conclusion, the study revealed that the male gender had a higher incidence of HCV infection than in the female gender and the pediatric age groups 1-5 and 6-12 years old children were predominantly affected with HCV infection. The transfusion of blood and related products were the primary factors and sources of HCV infections. A pair of nested PCR amplified products was successfully detected consisting of 343 bp and 417bp sequences in the HCV infected cases and these were used in the HCV diagnosis along with ELISA test.
Acknowledgment
The authors (S. Magesh and Dr. G. Bupesh) acknowledge the funding agencies ICMR for the financial support to carry out this work at King Institute of Preventive Medicine and Research Chennai, India.
References
-
Saha K, Firdaus R, Biswas A, Mukherjee A, Sadhukhan PC (2014) A novel nested reverse-transcriptase polymerase chain reaction method for rapid hepatitis C virus detection and genotyping. Indian J Med Microbiol 32(2): 130-136.
-
Waheed Y, Shafi T, Safi SZ, Qadri I (2009) Hepatitis C virus in Pakistan: a systematic review of prevalence, genotypes and risk factors. World J Gastroenterol 15(45): 5647-5653.
-
Suzuki R, Sakamoto S, Tsutsumi T, Rikimaru A, Tanaka K, et al. (2005) Molecular determinants for subcellular localization of hepatitis C virus core protein. J Virol 79(2): 1271-1281.
-
Gao QJ, Liu DW, Zhang SY, Jia M, Wang LM, et al. (2009) Polymorphisms of some cytokines and chronic hepatitis B and C virus infection. World J Gastroenterol 15(44): 5610-5619.
-
Simmonds P, Holmes EC, Cha TA, Chan SW, McOmish F, et al. (1993) Classification of hepatitis C virus into six major genotypes and a series of subtypes by phylogenetic analysis of the NS-5 region. J Gen Virol 74(pt 11): 2391-2399.
-
Vennila S, Magesh S, Roohin R, Gunasekaran P, Kavita A, et al. (2014) Epidemiology and Molecular characterization of Hepatitis C virus in Tamilnadu (India) during the year 2013. Int J Adv Res 2(11): 935-943.
-
Ramia S, Eid FJ (2006) Distribution of hepatitis C virus genotypes in the Middle East. Int J Infect Dis 10(4): 272-277.
-
Monica MV, Camila MR, Michele SG, Maria FG, Flair JC, et al. (2010) Molecular Characterization, Distribution and Dynamics of Hepatitis C Virus Genotypes in Blood Donors in Colombia. J Med Virol 82(11): 1889-1898.
-
Panigrahi AK, Panda SK, Dixit RK, Rao KV, Acharya SK, et al. (1997) Magnitude of Hepatitis C virus infection in India. Prevalence in healthy blood donors, acute and chronic liver diseases. J Med Virol 51(3): 167- 174.
-
Sampietro M, Caputo L, Annoni G, Corbetta N, Ticozzi A, et al. (1998) High prevalence of clinically silent HCV infection in older people. J Am Geriatr Soc 46(8): 1057-1058.
-
Liang TJ, Rehermann B, Seeff LB, Hoofnagle JH (2000) Pathogenesis, natural history, treatment, and prevention of hepatitis C. Ann Intern Med 132(4): 296-305.
-
Fattovich G, Stroffolini T, Zagni I, Donato F (2004) Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology 127(5): S35-S50.
-
Enomoto N, Takada A, Nakao T, Date T (1990) There are two major types of hepatitis C virus in Japan. BiochemBiophys Res Commun 170(3): 1021-1025.
-
Ohno O, Mizokami M, Wu RR, Saleh MG, Ohba K, et al. (1997) New Hepatitis C Virus (HCV) Genotyping System That Allows for Identification of HCV Genotypes 1a, 1b,2a, 2b, 3a, 3b, 4, 5a, and 6a. J Clin Microbiol 35(1): 201-207.
-
Garson JA, Tedder RS, Briggs M, Tuke P, Glazebrook JA, et al. (1990) Detection of hepatitis C viral sequences in blood donations by ‘‘nested’’ polymerase chain reaction and prediction of infectivity. Lancet 335(8703): 1419-1422.
-
Garson JA, Ring CJ, Tuke PW (1991) Improvement of HCV genome detection with ‘‘short’’ PCR products. Lancet 338(8780): 1466-1467.
-
Bukh J, Purcell RH, Miller RH (1993) At least 12 genotypes of hepatitis C virus predicted by sequence analysis of the putative E1 gene of isolates collected worldwide. Proc Natl Acad Sci 90(17): 8234-8238.
-
Sandres-Saune K, Deny P, Pasquier C, Thibaut V, Duverlie G, et al. (2003) Determining hepatitis C genotype by analyzing the sequence of the NS5b region. J Virol Methods 109(2): 187-193.
-
Kwok S, Higuchi R (1989) Avoiding false positives with PCR. Nature 339: 237-238.
-
Malloy HT, Evelyn KA (1937) The determination of bilirubin with the photoelectric colorimeter. J Biol Chem 119: 481-490.
-
Kind PN, King EJ (1971) Invitro determination of serum alkaline phosphatase. J Clin Path 7: 322-336.
-
Reitman S, Frankel S (1975) Invitro determination of transaminase activity in serum. Am J Clin Path 28: 56- 58.
-
Toledo ACJ, Greco DB, Felga M, Barreira D, Gadelha M (2005) Seroprevalence of hepatitis B and C in Brazilian army conscripts in 2002. A cross-sectional study. Brazilian J Infect Dis 9(5): 374-383.
-
Osella AR, Sonzogni L, Cavallini A, Foti L, Guerra V, et al. (1993) Molecular epidemiology of hepatitis C virus infection in an area of hyperendemicity in Southern Italy: a population-based study. J Clin Microbiol 37(7): 2371-2372.
-
Osella AR, Misciagna G, Vito G, Silvana E, Giampiero B, et al. (2001) Hepatitis C Virus Genotypes and Risk of Cirrhosis in Southern Italy, Clin Infect Dis 33(1): 70- 75.
-
Osella AR, Misciagna G, Leone A, Di Leo A, Fiore G (1997) Epidemiology of hepatitis C virus infection in an area of Southern Italy. J Hepatol 27(1): 30-35.
-
Guadagnino V, Stroffolini T, Rapicetta M, Costantino A, Kondili LA, et al. (1997) Prevalence, risk factors, and genotype distribution of hepatitis C virus infection in the general population: a community- based survey in Southern Italy. Hepatology 26(4): 1006-1011.
-
Bellentani S, Tiribelli C, Saccoccio G, Sodde M, Fratti N, et al. (1994) Prevalence of chronic liver disease in the general population of Northern Italy: the Dionysos Study. Hepatology 20(6): 1442-1449.
-
Saran N, Bupesh G, Magesh S, Vennila S, Anandharaj B, et al. (2015) Epidemiological Studies and Molecular Characterization of Herpes Simplex Virus among Urban Population in Chennai, Tamilnadu. Epidemiology 5: 187.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions