Environmental and Genetic Factors Modulating Immune Responses: A Preliminary Survey of Allergic Rhinitis and Co-Morbid Conditions in Immigrants to North America
Allergic rhinitis is an IgE mediated inflammation of the upper airway. It is a complex multi-factorial immune system response to environmental allergens that has been on the rise throughout the world, more so in the industrialized, affluent nations. However, the interaction between environmental and genetic factors in generating the susceptibility or tolerance to various allergens and the way it affects the immune response is poorly understood. We conducted a survey with the aim to examine whether change in environment by migration to North America affected individuals and made them prone to developing allergies and co morbid conditions. Study result indicated that 60% of the participants developed allergies only after migration with no prior experience of any allergic symptoms in their country of origin. Residence time seemed to have worsened the condition in all of these respondents. The study also showed that not all members of the migrant family showed similar sensitizations to allergens indicating that there may be genetic variations and underlying complex mechanisms of gene-environment interaction in breaking down an individual’s immune tolerance. However, the sample size relied on is small and not enough to provide statistical significance and solid conclusions.
Introduction
Allergic diseases are classified as the IgE mediated hypersensitivity reactions of the immune system resulting in inflammatory response to normally harmless allergens in the environment. These immune responses can range from mild and self-resolving, as in hay fever and seasonal Environmental and Genetic Factors Modulating Immune Responses: A Preliminary Survey of Allergic Rhinitis and Co-Morbid Conditions in Immigrants to North America allergies, to chronic conditions as in sinusitis, asthma and in some reactions such as anaphylaxis, it is life threatening. According to the White Book on Allergy published by World Allergy Organization (WAO) in 2011, allergic diseases account for a significant proportion of the chronic illnesses that affect the health and quality of life of the population worldwide [1]. Allergic diseases Virol Immunol J
such as rhinitis, food allergies, atopic dermatitis, asthma and chronic sinusitis triggered by allergies have been described as an epidemic that has increased both in prevalence and incidence over the last 20 years [1]. It is estimated that 1 in every 6 Americans or 50 million persons, approximately experience allergies including nasal, food, drug, skin and insect allergies and it has been reported to be increasing in all age groups for the past 15- 20 years [1]. Sensitization rates to one or more common allergens among school children are currently approaching 40-50%. In U.S alone, the national cost to health care and lost productivity is estimated to be over $7 billion and a staggering annual cost of nearly $25 billion, if burden of asthma is added to the picture [1]. Allergic rhinitis (AR) among these is the most common allergic disorder and affects 15% of the general population and up to 50% of adolescents as per WAO (2011) Traditionally, it was treated as seasonal and perennial, based on the persistence of symptoms from days to few weeks and to year around, respectively [1]. In 2001, new rhinitis nomenclature proposed by the ‘Allergic Rhinitis and its Impact on Asthma’ (ARIA), working group of the WHO, superseded the traditional seasonal or perennial classification of allergic rhinitis [2]. ARIA divides allergic rhinitis into intermittent (less than four days per week or less than four weeks in duration) and persistent (more than 4 days per week and over four weeks in duration) [2]. Intermittent and persistent allergic rhinitis are further sub-divided into mild (minimal symptoms) or moderate/severe (troublesome symptoms, sleep disturbance and impairment of daily activities) [2]. The symptoms with pollen exposure include intense itching of the nose, eyes, palate, ears and throat with repetitive bouts of sneezing, profuse watery nose, tearing and occasionally, allergen- induced wheezing in the form of hay asthma [2]. The seasonal allergens include tree pollens, grass pollens, wood pollens, mould spores depending on the time of the year. Persistent severe rhinitis symptoms however, include chronic nasal blockage, sinus congestion, post nasal drip, headaches and fatigue related to chronic house dust mite, pet exposure and occupational allergens [2]. Several previous studies on immigrants showed evidence for capacity of the environment to modulate inflammatory responses by altering the metabolic homeostasis and increasing the risk of allergies. Newbold in 2005 stated that immigrants undergo medical screening and exhibit a good health status, which is termed as `healthy immigrant effect’ [3]. However, when they move from areas of low to high prevalence of allergies, this status declines and converges to that of natives or even becomes worse. The changes of the immuno-modulation appear to occur overtime, in 10 years or so, after arrival and the disease susceptibility seem to manifest across age groups from children to adults, across countries and result in various inflammatory auto immune diseases such as allergies, type I diabetes, multiple sclerosis, depression and cancers [3, 4, 5, 6, 7, 8, 9, 10]. In the context of growing prevalence of allergic diseases, our objective of this study is to observe the occurrence of allergic rhinitis in selected migrant population to North America. The proposed hypotheses were as follows: Immigration is an environmental risk factor that causes allergies, Allergy conditions get worse with time and correlate to residence time, Family history plays a role in allergy status, Family members do not show similar allergy status and clinical presentation indicating underlying genetic and epigenetic variations, Observe hygiene hypothesis in the framework of the first two variables.
Methods
Participants
A total of hundred and nine participants from North America voluntarily participated in the medical research study. Of the hundred and nine participants, 46% were males and 54% were females ranging in ages from 16 to 66 years old. All participants were given the same questionnaire to complete by a non-random sampling method. The survey was open to all interested participants; however, immigrants to North America were particularly encouraged to take the survey. The only limitation to the study is that we did not have an opportunity to reach participants at primary care centers and allergy clinics.
Materials
Google Drive forms, was the tool used to construct and distribute the survey, which consisted of the consent form and the survey questionnaire. The link of the survey was distributed to the population by personal contacts, social networking sites (e.g., Face book), and emails. All responses collected were anonymous and the results were recorded on a spreadsheet through Google Docs.
Procedure
The participants were informed in the consent form that the aim of the study is to investigate the incidence and time on-set of allergic rhinitis in Immigrants. Following the consent form, the survey link provided a questionnaire that investigated demographic characteristics, environmental factors (supplements intake, decreased sleep, smoking and alcohol consumption), allergic symptoms, and genetic factors (Asthma history in the family, food allergies and lactose intolerance). The survey link was open for a period of four weeks to provide sufficient time for all the potential participants to take part in the survey. When the survey link was closed, all the data was automatically combined in a spreadsheet for further analysis.
Results
According to our Convenience sampling survey, there were 109 participants between the ages 16 to 66 years in the study. The country of origin of the participants with a total of 26 countries are: India (39%), USA (17%), Afghanistan (3%), Sri Lanka (4%), Egypt (4%), Canada (6%), Albania (1%), Bolivia (1%), Brazil (2%), Cameroun (1%), France (1%), Philippines (1%), Poland (1%), Guyana (1%), Iraq (2%), Jordan (1%), Kuwait (3%), Mexico (1%), Nigeria (3%), Norway (2%), Romania (1%), Saudi Arabia (2%), Togo (1%), Turkey (4%), Vietnam (1%), and Yemen (1%). Out of the 109 participants, 82 migrated to North America and 27 participants were born in North America and therefore did not migrate to North America. For further analysis, gender breakdown included 40 males and 42 females in the migrated participants and 10 males and 17 females in the non- Immigrants. Results in Table 1 showed the gender, age, occupation, and the allergy status among the participants. The most predominant age group and occupation in both the immigrant and non-immigrant categories are between the ages of 21 to 25 and students, respectively. A total of 23 out of 82 immigrants had allergies and 18 out of 27 non- immigrants had allergies. These data helped in the interpretation of allergy status from the demographic of the participants who migrated and those who did not migrate.
| Demographics on Migrant Participants | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GENDER | FEMALE | (%) | MALE | (%) | TOTAL | (%) | ||||||||||||||
| Number of participants | 42 | 51% | 40 | 49% | 82 | |||||||||||||||
| AGE (YRS) | ||||||||||||||||||||
| <20 | 4 | 5% | 2 | 2% | 6 | 7% | ||||||||||||||
| 21-25 | 20 | 24% | 17 | 21% | 37 | 45% | ||||||||||||||
| 26-30 | 6 | 7% | 7 | 9% | 13 | 16% | ||||||||||||||
| 31-35 | 4 | 5% | 2 | 2% | 6 | 7% | ||||||||||||||
| 36-40 | 3 | 4% | 4 | 5% | 7 | 9% | ||||||||||||||
| >41 | 5 | 6% | 8 | 10% | 13 | 16% | ||||||||||||||
| OCCUPATION | ||||||||||||||||||||
| Business | 5 | 6% | 1 | 1% | 6 | 7% | ||||||||||||||
| Engineer/IT | 1 | 1% | 9 | 11% | 10 | 12% | ||||||||||||||
| House Wife | 4 | 5% | 0 | 0% | 4 | 5% | ||||||||||||||
| Student | 20 | 24% | 19 | 23% | 39 | 48% | ||||||||||||||
| Public Service | 0 | 0% | 1 | 1% | 1 | 1% | ||||||||||||||
| Healthcare | 2 | 2% | 2 | 2% | 4 | 5% | ||||||||||||||
| Teacher | 2 | 2% | 0 | 0% | 2 | 2% | ||||||||||||||
| Self Employed | 0 | 0% | 1 | 1% | 1 | 1% | ||||||||||||||
| Other | 8 | 10% | 8 | 10% | 16 | 20% | ||||||||||||||
| Allergy Status | ||||||||||||||||||||
| Yes | 10 | 12% | 13 | 16% | 23 | 28% | ||||||||||||||
| No | 32 | 39% | 27 | 33% | 59 | 72% |
Table 1: Demographics of the immigrant and non-immigrant participants. Out of the 23 people that had allergies, 14 people develop
| Demographics Of Non-Immigrant Participants | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GENDER | FEMALE | ( %) | MALE | (%) | TOTAL | (%) | ||||||||||||||
| Number of participants | 17 | 63% | 10 | 37% | 27 | 100% |
Table 2: Demographics of the immigrant and non-immigrant participants. Out of the 23 people that had allergies, 14 people develop
| AGE(YRS) | ||||||
|---|---|---|---|---|---|---|
| <20 | 1 | 4% | 2 | 7% | 3 | 11% |
| 21-25 | 13 | 48% | 4 | 15% | 17 | 63% |
| 26-30 | 3 | 11% | 2 | 7% | 5 | 19% |
| 31-35 | 0 | 0% | 0 | 0% | 0 | 0% |
| 36-40 | 0 | 0% | 1 | 4% | 1 | 4% |
| >40 | 0 | 0% | 1 | 4% | 1 | 4% |
| OCCUPATION | ||||||
| Student | 11 | 41% | 2 | 7% | 13 | 48% |
| Healthcare | 0 | 0% | 1 | 4% | 1 | 4% |
| Transportation | 1 | 4% | 0 | 0% | 1 | 4% |
| Engineer | 0 | 0% | 2 | 7% | 2 | 7% |
| Administration | 1 | 4% | 1 | 4% | 2 | 7% |
| N/A | 4 | 15% | 3 | 11% | 8 | 30% |
| Allergy Status: | ||||||
| Yes | 14 | 52% | 4 | 15% | 18 | 67% |
| No | 3 | 11% | 6 | 22% | 0 | 33% |
Table 3: Demographics of the immigrant and non-immigrant participants. Out of the 23 people that had allergies, 14 people develop
Table 1: Demographics of the immigrant and non-immigrant participants. Out of the 23 people that had allergies, 14 people developed allergies after migration, shown in Table 2. All 14 people that developed allergy after migration reported that the condition developed after migration to North America. This accounted for 60% of the total respondents with allergies in the migrant status group.
| Development of Allergy after Migration | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Immigrants | Number of People | |||||||||||||
| YES | (%) | NO | (%) | |||||||||||
| First Time Allergy After Migration | ||||||||||||||
| 14 | 17% | 68 | 83% | |||||||||||
| Condition After Migration | Number of People | |||||||||||||
| Worse | 14 | |||||||||||||
| Better | 5 | |||||||||||||
| Not Applicable | 63 |
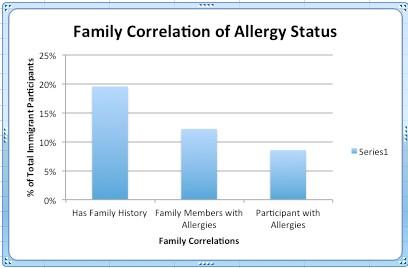
Table 4: Development of allergy after migration. Analysis of family correlation with allergy status in immigrants is shown in fig
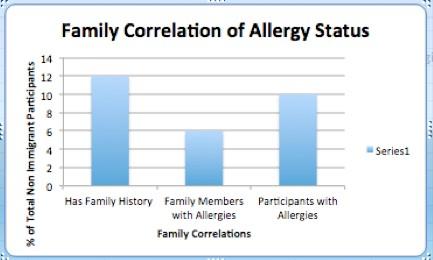
Table 2: Development of allergy after migration. Analysis of family correlation with allergy status in immigrants is shown in figure 1. From the 82 participants, 16 people stated they had family history of allergies. Out of the 16 people, 7 allergy respondents stated that they had corresponding family member with allergies as well and 10 people who did not have allergies stated they had a family member that developed allergies. Result in figure 2 shows family correlation in allergy status in non- immigrants. From the 27 participants, 12 allergy respondents had family history of allergies. Out of the 12 people, 10 participants who had allergies stated that they had corresponding family members with allergies and 6 stated that did not have allergies but the family members had allergies.
- There are other factors on which data was collected
- Different Factors Affecting Allergies in Participants
- Immigrants
- Number of People
- Allergic Participants
- YES
- (%)
- NO
- (%)
- YES
- CYO
- NO
- (%)
- Asthma History in Family
- 16
- 20%
- 66
- 80%
- 5
- 22%
- 18
- 78%
- Supplements
- 16
- 20%
- 66
- 80%
- 5
- 22%
- 18
- 78%
- Food Allergies
- 10
- 12%
- 72
- 88%
- 7
- 30%
- 16
- 70%
- Lactose Intolerance
- 10
- 12%
- 72
- 88%
- 6
- 26%
- 17
- 74%
- Decreased Sleep
- 4
- 5%
- 78
- 95%
- 4
- 17%
- 19
- 83%
- Smoking
- 3
- 4%
- 79
- 96%
- 0
- 0%
- 23
- 100%
- Alcohol
- 28
- 34%
- 54
- 66%
- 10
- 43%
- 13
- 57%
- Non-Immigrants
- Number of People
- Allergic Participants
- YES
- ( %)
- NO
- ( %)
- YES
- ( %)
- NO
- (%)
- Asthma History in Family
- 7
- 26%
- 20
- 74%
- 6
- 33%
- 12
- 67%
- Supplements
- 7
- 26%
- 20
- 74%
- 3
- 17%
- 15
- 83%
- Food Allergies
- 5
- 19%
- 22
- 81%
- 4
- 22%
- 14
- 78%
- Lactose Intolerance
- 3
- 11%
- 24
- 89%
- 2
- 11%
- 16
- 89%
- Decreased Sleep
- 5
- 19%
- 22
- 81%
- 4
- 22%
- 16
- 89%
- Smoking
- 1
- 4%
- 26
- 96%
- 1
- 6%
- 17
- 94%
- Alcohol
- 16
- 59%
- 11
- 41%
- 7
- 39%
- 11
- 61%
Table 5: Different factors affecting allergies.
Discussion
Result from our study, showed that 14 respondents (60%) out of the 23 participants who had allergies developed the condition only after migrating to North America, suggesting that change in environment is the main risk factor in these individuals. Increase in allergen prevalence over the last 25 years is likely due to changes in our environment or lifestyle because changes in our genetic makeup would take more than several generations to occur. When looking at environment factors and allergic prevalence, “susceptibility” factors should also be taken into consideration. This includes populations at risk, known risk factors, and preventative measurements to know potential interactions [11]. It has been reported that though immigrants had less family history of Type I Hypersensitivity, once in a new environment, they were severely affected [12]. They were reported to have a higher rate of mono sensitivity [11]. Perhaps, a longitudinal study may reveal further information on the pathogenic role of local environmental conditions in sensitized individuals.
Further studies consistently found that immigrants tended to develop allergies at different rates with symptoms often appearing 3 to 5 years after settlement into new environment [13]. This was observed in our study as more migrants in our study reported developing allergy after migration. As allergies are classified as heterogeneous, different forms can be found from different geographic locations; for example the inner city or rural area may affect different populations, genders, and ages differently and sometimes severely than the local population [14]. Environmental factors affecting the older population may include indoor and outdoor air pollution, occupational exposures, and active and passive smoking [14]. This is because older adults have smaller airways than younger adults, thus their bronchi is more hyper-responsive to such environmental pollutants; for example, cigarette smoking heightens the production of IgE antibodies which then stimulates the production of inflammatory markers. This immune mechanism causes persons with existing allergies to have hyperinflation in turn causing hypersensitivity to already existing asthma issues [14]. In our study, none of the immigrants with allergy reported smoking while only one participant reported smoking among non-immigrants. A study done on older women associated with occupations in various fields (e.g., art, decorating, technology, health professions), in Northern California was shown to be correlated with the appearance of allergic symptoms, such as asthma. The same study was done in developing countries such as India; older women were affected by asthma or other allergic symptoms due to association with the use of biomass fuels for cooking and heating purposes, as well as the fact that most stoves and sleeping quarters were within one room [14]. The majority of our study participants are students and some refuse to mention their occupation. The development of allergic reactions can be contributed by both genetic and environmental determinants. Immigrant population is a unique group that experiences a sudden and permanent shift in their physical and social environment with exposure to new life style, diet, pollutants, living conditions, and medical services. In our study, out of the 23 respondents who had allergies, 60% reported as having developed allergies after migration to North America and their condition worsened over the years; however, asthma history in the family is among the highly reported factors among immigrant and non-immigrant population in our study. Numerous studies have concluded that any mutations or changes to genetic background would take many years and would affect the next generation whereas environmental conditions such as pollution, variability in microbiota and quite possibly genetically modified foods would account for the increasing development of allergic reactions [13, 14]. In our study, alcohol consumption was the most reported factor among immigrant and non- immigrant population, while food allergies, decrease sleep and lactose intolerance were also reported. Epigenetics is an indication that environmental changes can affect the function of immunity irrespective of genetic background [15]. There is now evidence that these environmental exposures can modify early immune gene expression through potentially heritable epigenetic changes [11, 15]. Vitamin D also known as the “sunshine hormone” plays an important role in both adaptive and innate immune functions involved in the development and progression of allergic diseases [13, 16]. Various studies, both clinical and experimental, over the years have been done to investigate whether vitamin D insufficiency has a role in allergic prevalence [measured as serum 25 hydroxy vitamin D–25(OH)D] [16]. Vitamin D is known to mimic various immune cells, monocytes, dendritic cells, T and B cells, and various functions of epithelial cells thus forming a barrier against allergens and controlling and promoting regulatory immune response and defense [12, 13, 16]. Early exposure to vitamin D may prove to be beneficial and may promote mucosal defense and allergen tolerance and in turn help maintain healthy microbial immune system [13, 16]. Although more patients in our study reported taking supplement among the factors affecting allergies, majority of our sampled patients reported that they do not take supplement.
Limitations of the Study
In our study, we attempted to observe, if there is any correlation between area of residence and sensitization to allergens, particularly in the Northern part of the US & Canada with winter conditions and comparatively less exposure to sun. Due to limited sample size and lack of proper response to the question by all participants, we could not draw any meaningful conclusions. In addition, time available to conduct the survey, small sample size and recall bias from the participants hampered our ability to establish statistical significance and observe the hypotheses.
Conclusion
Allergic rhinitis and complications have been on the rise at a significant cost to public health. Immigration to allergy-prevalent countries is associated with a higher prevalence of allergies and asthma and therefore a risk factor for immigrants, as compared to the prevalence of atopy in their countries of origin. Studies on immigrants support the notion that in western industrialized countries, lifestyle and environmental factors facilitate atopy and asthma. The effect is time-dependent and the development of allergy is influenced by the age at the time of immigration and length of stay. Compared with the local population, recent immigrants have higher levels of IgE, which gradually decrease to the levels of the general population and increase the prevalence of allergic diseases. There is a need for more consistent epidemiological research in immigrant population to North America to gather valuable information on the role of environmental factors in the development of allergic rhinitis and confirm the studies done in other countries. Interaction of genetic factors with environment and variations in immune responses would help identify risk groups. Combining studies that also focus on gene-environment interactions and epigenetic mechanisms in the disease process observed in immigrant population may reveal interesting insights. A proper understanding of susceptibility and pathogenesis in these risk groups would allow development of proper prevention protocols.
References
-
Pawankar R, Canonica GW, Holgate ST, Lockey RF (2011) World Allergy Organization (WAO) white book on allergy. Wisconsin: World Allergy Organisation 1-220.
-
Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, et al. (2008) Allergic rhinitis and its impact on asthma (ARIA) 2008. Allergy 63(s86): 8-160.
-
Newbold KB (2005) Self-rated health within the Canadian immigrant population: risk and the healthy immigrant effect. Social science & medicine 60(6): 1359-1370.
-
Bodansky HJ, Staines A, Stephenson C, Haigh D, Cartwright R (1992) Evidence for an environmental effect in the aetiology of insulin dependent diabetes in a transmigratory population. BMJ 304(6833): 1020-1022.
-
Kalyoncu AF, Stålenheim G (1992) Serum IgE levels and allergic spectra in immigrants to Sweden. Allergy 47(4): 277-280.
-
Leung RC, Carlin JB, Burdon JGW, Czarny D (1994) Asthma, allergy and atopy in Asian immigrants in Melbourne. The Medical Journal of Australia 161(7): 418-425.
-
Leung R (1996) Asthma and migration. Respirology 1(2): 123-126.
-
Hammond SR, English DR, McLeod JG (2000) The age- range of risk of developing multiple sclerosis: evidence from a migrant population in Australia. 123(5): 968-974.
-
Grüber C, Illi S, Plieth A, Sommerfeld C, Wahn U (2002) Cultural adaptation is associated with atopy and wheezing among children of Turkish origin living in Germany. Clinical & Experimental Allergy 32(4): 526-531.
-
Pinheiro PS, Sherman RL, Trapido EJ, Fleming LE, Huang Y, et al. (2009) Cancer incidence in first generation US Hispanics: cubans, Mexicans, Puerto Ricans, and new Latinos. Cancer Epidemiology and Prevention Biomarkers 18(8): 2162-2169.
-
Marcon A, Cazzoletti L, Rava M, Gisondi P, Pironi V, et al. (2011) Incidence of respiratory and allergic symptoms in Italian and immigrant children. Respiratory medicine 105(2): 204-210.
-
Gibson PG, Henry RL, Shah S, Powell H, Wang H (2003) Migration to a western country increases asthma symptoms but not eosinophilic airway inflammation. Pediatric pulmonology 36(3): 209-215.
-
Lombardi C, Passalaqua G, Canonica GW (2009) ''United Airways Disease'' and phenotypic peculiarities of respiratory allergy in immigrants. World Allergy Organization Journal 2(2): 13.
-
Yeatts K, Sly P, Shore S, Weiss S, Martinez F, et al. (2006) A brief targeted review of susceptibility factors, environmental exposures, asthma incidence, and recommendations for future asthma incidence research. Environmental health perspectives 114(4): 634-640.
-
Prescott S, Saffery R (2011) The role of epigenetic dysregulation in the epidemic of allergic disease. Clinical epigenetics 2(2): 223-232.
-
Reinholz M, Ruzicka T, Schauber J (2012) Vitamin D and its role in allergic disease. Clinical & Experimental Allergy 42(6): 817-826.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions