Management of Rheumatoid Arthritis and Effectiveness of Disease Modifying Anti-Rheumatic Drug Therapy
Background: Rheumatoid arthritis is the most common form of polyarticular arthritis, where the body’s own defense system targets the joint linings, bones and cartilage that ultimately leads to disability. The study aims to observe the effectiveness of disease modifying anti-rheumatic drugs therapy in the management of rheumatoid arthritis and to access disease compliance with adviced life style changes. Methods: A prospective, observational and questionnaire based study was conducted during July 2017 to August 2017 in different hospitals of Lahore, Pakistan. 200 patients with Rheumatoid arthritis were selected by convenient random sampling. The questionnaire was filled during face to face interviews with patients. The collected data was analyzed, tabulated and presented in the form of graphs and tables. Results: The results showed that 76% were females and 24% were males. 80% having major symptom of morning stiffness while 10% having swelling. 81%were using disease modifying anti-rheumatic drugs therapy.74% patients were using Plaquin HCQ, 3% Deltacortil and 45.5% Methotrexate (45.5%). Patients compliance was 67.9% with disease modifying anti-rheumatic drugs therapy. Conclusion: It was concluded that the managerial therapies used for rheumatoid arthritis treatment were satisfactory with disease modifying anti-rheumatic drugs therapy. Moreover, healthier lifestyle modifications slow down the disease progression.
Introduction
Rheumatoid Arthritis (RA) is a chronic inflammatory disorder that can affect the joints linings, bones and cartilage. RA occurs when the body’s own defense system attacks the synovium, the lining of the membranes that surrounds the joints. It results in inflammation that thickens the synovium [1]. Furthermore, it can destroy the bone cartilage and affects the extra-articular structures resulting in pain, swelling, disability, deformity and mortality [2]. Most commonly affected joints are joints of hands, feet, wrists, elbow, knees, shoulder and ankles. The resulting joint inflammation can also affect the non-joint structures, including the skin, eyes, lungs, heart and blood vessels [3]. RA is characterized as systemic autoimmune disease which affects around 1% of world population [4]. In Pakistan, prevalence of RA is about 0.5% [5]. Throughout world, the number of females having RA is far greater than that of males, as male to female ratio is 1:2. The risk of developing RA is 3.6% in females and 1.7% in males. RA starts between the age of 30-60 in females but somewhat later in males. In both genders, Hormones can play a significant role either in preventing or triggering it. However, RA can occur at any age, even the children under 10 years can get it (Juvenile arthritis) [6]. Studies found that people with a specific genetic marker called HLA (Human Leukocyte Antigen) shared epitope have five times greater chances of developing RA from those which are without marker. The site of genetic HLA controls immune responses [7]. Other factors that might playing the role are under investigation that include infectious agents such as bacteria or viruses, response of body to stressed events, environmental factors such as cigarette smoking, air pollution, insecticides and occupational exposures to silica and mineral oil. Most joint symptoms are identifying factor to RA which includes vague pain, tenderness, redness, swelling or stiffening of joints for one month or longer. Symptoms may affect the joints on both sides of the body. Many patients may feel fatigue in physical work, loss of appetite which can lead to weight loss, weakness and a low-grade fever with intervals [8]. Continuation in high level inflammation can also lead to problems in whole body which includes pain and redness of eyes, dryness of eyes and mouth, rheumatoid nodules formation and anemia [9]. It can be difficult to diagnose RA in its early stages because the early signs and symptoms resemble those of many other diseases. Ultimately, RA is diagnosed by combinations of clinical presentations including joint swelling, stiffness in the morning, presence of blood rheumatoid factor (RF test or RA test) and anti-cyclic citrullinated peptide (anti-CCP test), as well as findings of rheumatoid nodules near to joints and radiographic testing (X-ray) [10, 11]. The degree of inflammation can be measured by blood tests i.e. ESR (erythrocyte sedimentation rate), ANA (anti-nuclear antibodies), CRP (C-reactive protein) [12]. Over the last 30 years, several effective treatments have been developed but none cured RA. Two classes of medications are used in the treatment of RA, first-line drugs include NSAIDs that are useful adjuvant therapy for the symptomatic management of RA, as this class of medications can reduce joint swelling, tenderness, and pain [13]. The slow-acting, second-line drugs include disease modifying anti-rheumatic drugs (DMARDs) that are used to prevent progressive joint destruction [14]. Corticosteroids and steroids reduce inflammation and pain and slow down the joint damage. Combination therapy with biological agents can be highly effective in patients who have risk factors such as high level of anti- CCP, RF, joint damage and deformity. If the medications are not sufficient to prevent the joint damage, then surgery is considered effective that may include removal of inflamed synovium (synovectomy), joint fusion, tendon repair and totally joint replacement [15]. Due to increase in prevalence of disease in worldwide population, Rheumatology has gained a lot of importance rapidly. Expert pharmacists can play a role in educating people to understand the disease, in providing multidisciplinary access to self-management and disease management programs of rheumatoid arthritis, which is both clinically and costly effective [16]. The study aims to observe the effectiveness of disease modifying anti-rheumatic drugs therapy in the management of rheumatoid arthritis and to access disease compliance with advised life style changes.
Materials and Methods
A prospective, observational and questionnaire based study was conducted using convenient random sampling technique, during July 2017 to August 2017 in four major hospitals of Lahore, Pakistan (Sheikh Zayed Hospital, Jinnah Hospital, Shalimar Hospital, Services Institute of Medical Sciences, Lahore). 200 patients with RA were included and those patients not having rheumatoid arthritis were excluded. A data collection tool (questionnaire) was designed covering aspects related to complications, different alternate treatments, life style changes, medications, side effects and compliance rate among rheumatoid arthritis patients. Data was collected by filling questionnaire in face to face interviews with patients and health care providers. Collected data was compiled, analyzed and results were presented in the form of tables and graphs.
gender, the number of female patients were 152 (76)% while male patients were 48 (24%). Results showed that most of signs and symptoms observed in patients were morning stiffness 160 (80%), swelling 20 (10%), fever 8 (4%), fatigue 8 (4%), and weight loss 4 (2%). A total of 56 (28%) were suffering from different joints deformity and 25 (12.5%) were smokers. In table-1, laboratory findings revealed that majority of the patients were found with positive blood rheumatoid (RA) factor and Anti-CCP test (Anti-cyclic citrullinated peptide) and they were seropositive (78.5%). Others who gave both tests negative, were seronegative (21.5%). Only 40% patients were diagnosed with increased ESR (erythrocyte sedimentation rate). Life style changes showed that, 40.5% patients were involved in avoiding non-protein food but 59.5% patients were not following any diet chart and 61% of patients were not following any physical activity or exercise.
Ethical Considerations
This study was approved from Institute of Pharmacy, Lahore College for Women University Lahore with all components of research protocol. Before data filling, participants were asked about their willingness or unwillingness. Confidentiality and privacy was insured for information collected from study participants.
Results
200 patients were included in the study. Demographic characteristics of patients are depicted in Table-1. A total of 3 (1.5%) were under 10 years of age suffering from juvenile rheumatoid arthritis, 51 (25.5%) were between10-30 years, 55.5% (111) were between 31- 50years, and 35 (17.5%) were more than 50 years. The mean age of rheumatoid arthritis patients (who were being treated) was found to be 31 years. According to
- Parameters
- Variables
- Frequency (n=200)
- Percentage %
- Under 10 years
- 3
- 1.50%
- 10-30 years
- 51
- 25.50%
- 31-50 years
- 111
- 55.50%
- 50 years or above
- 35
- 17.50%
- Age
- Gender
- Male
- 48
- 24%
- Female
- 152
- 76%
- Morning stiffness
- 160
- 80%
- Swelling
- 20
- 10%
- Fever
- 8
- 4%
- Fatigue
- 8
- 4%
- Weight loss
- 4
- 2%
- Symptoms
- Joint deformity
- Yes
- 56
- 28%
- No
- 144
- 72%
- Smoking
- Smokers
- 25
- 12.50%
- Non-smokers
- 175
- 87.50%
- Seropositive
- 157
- 78.50%
- Seronegative
- 43
- 21.50%
- Increased ESR
- 80
- 40%
- Blood tests
- Non-Protein Diet
- Yes
- 81
- 40.50%
- No
- 119
- 59.50%
- Physical exercise
- Yes
- 78
- 39%
- No
- 122
- 61%
Table 1: Demographic characteristics of patients.
79% patients and corticosteroids were prescribed to 49.5% patients of RA.
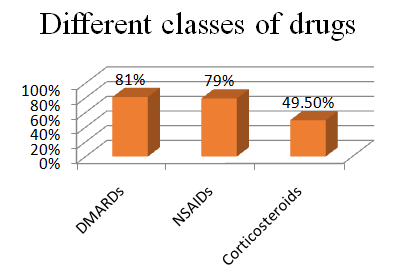
Figure 1: Different classes of drugs used. Figure-2 revealed that in the DMARDs therapy, Plaquin HCQ was prescribed in higher percentage i.e. 74% to patients, Methotrexate 45% and other medications prescribed were Lefora 6%, Delta Cortril 73%, Supplements 49%, Salazodine EC 49.5%, Gevolox500mg 22.5% and Supplements 49% and only 3% were prescribed with proton pump inhibitors.
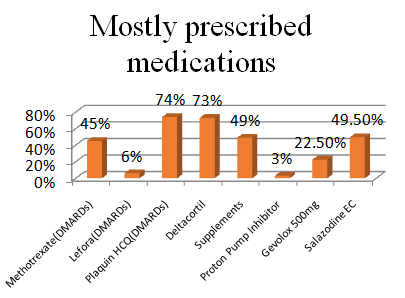
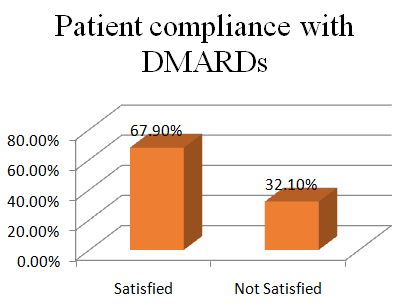
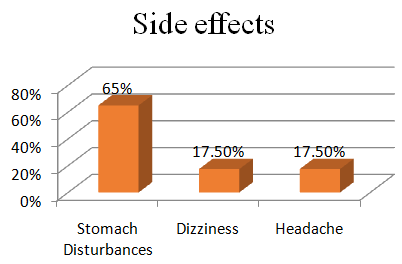
Figure 2: Mostly prescribed medications. Figure-3 showed that most patients were satisfied with DMARDs therapy as they found this therapy effective in their ailment as 67.9% patients had compliance with DMARD’s, but 32.1% patients had non-compliance due to reasons of financial, environmental, and medication side effects problems. Among side effects, 65% patients suffered from stomach disturbances 17.5% patients have dizziness and 17.5% headache as medication side effects (Figure 4).
Discussion
The study highlighted the higher incidence of RA in females than males in the ratio of 3:1. A study conducted in Rochester, Minnesota also demonstrated the same fact and found that the females were more prone to RA than males with the prevalence of 1.06% in women and 0.16% in men [17]. The hormonal variations and early onset of menopause are the contributing factors to the higher prevalence of RA in women [18]. The study showed that the treatment strategy adapted for the RA included DMARDs as drugs of choice. Other therapeutic classes were NSAIDs and supplements to prevent further joint destruction. Wolfe et al. has also shown the increased prescribing trend of DMARDs therapy from 1997 to 2007 in the treatment of RA [19]. The study focused on the effectiveness of DMARDs therapy in providing the symptomatic relief to RA patients. Wolfe et al. showed that DMARDs not only control the disease progression but also reduce the joint erosion and help to improve quality of life [20]. A study conducted in Malaysia has shown not only the effectiveness of DMARDs therapy but also highlighted that methotrexate and sulphasalazine were the drugs of choice in treating RA [21]. Another study conducted in USA also demonstrated the effectiveness of methotrexate and sulphasalazine in decreasing the disease activity and showed that these drugs were equally effective in treating RA [22]. The study showed that in addition to the medication use certain dietary precautions were also been advised to the patients to improve their health status and thus to enjoy quality life. A study conducted by Pattison and colleagues represented that the omega-3 fatty acid rich diet had an anti-inflammatory effect and thus beneficial in RA disorder [23]. A study by Shapiro, et al also reported the effectiveness of fish oil in preventing RA [24]. The study demonstrated that the RA patients were advised to adapt lifestyle modifications including weight loss and certain aerobic exercises to improve their joint mobility. Previous studies have also demonstrated the effectiveness of dynamic exercises to improve the muscle function and joint mobility in patients with active and inactive RA [25]. Significant benefits of intensive exercises were reported in RA patients [26]. The study also highlighted the satisfaction level and compliance of RA patients with DMARDs therapy as they found this therapy effective in retarding their disease progression. Darmawan and colleagues showed that discontinuing the therapy had worsened the disease [27]. A study conducted by Unk et al. has highlighted that certain educational and informative programs should be conducted in order to educate the patients about their disease and treatment that help them in improving their health and quality of life [28, 29].
Conclusion
Majority of the patients diagnosed with RA were females. DMARDs were still considered to be cornerstone in the treatment of RA. Patients were advised to adopt certain life style modifications to improve their joint mobility. There is no permanent cure of the RA and the goal of treatment is to reduce symptoms, reduce functional limitations, prevent joint deformity and decrease complication of the disease. Proper guidance regarding the disease is still lacking in the population. So, the role of health care professionals and pharmacists is very essential in helping the patients in managing their life and educating them about RA in order to lead them to healthier life.
Acknowledgement
We are extremely obliged to the staff of Sheikh Zayed Hospital Lahore, Jinnah Hospital Lahore, Shalimar Hospital Lahore and Services Institute of Medical Sciences, Lahore, who played a supporting role, and all patients who made this research possible.
References
-
Goldman L (2016) Ehlers-Danlos Syndrome Rheumatoid arthritis. Goldman Cecil Medicine 2(25): 1957-1978.
-
Birch JT Jr, Bhattacharya S (2010) Emerging trends in diagnosis and treatment of rheumatoid arthritis. Primary Care 37(4): 779-792.
-
Heidari B (2010) The associated factors of progressive disease and treatment decision in undifferentiated arthritis. Caspian Journal of Internal Medicine 1: 79-88.
-
Turesson C, Jacobsson L, Bergström U (1999) Extra- articular rheumatoid arthritis: prevalence and mortality. Rheumatology 38(7): 668-674.
-
Farooqi A, Gibson T (1998) Prevalence of the major rheumatic disorders in the adults’ population of North Pakistan. British Journal 37(5): 491-495.
-
Alam SM, Kidwai AA, Jafri SR, Qureshi BM, Sami A, et al. (2011) Epidemiology of Rheumatoid Arthritis in a tertiary care unit. Journal of Pakistan Medical Association 61(2): 123-126.
-
Pascual M, Nieto A, Lopez-Nevot MA, Ramal L, Mataran L, et al. (2001) Rheumatoid arthritis in southern Spain: toward elucidation of a unifying role of the HLA class II region in disease predisposition. Arthritis Rheumatology 44(2): 307-314.
-
Cojocaru M, Cojocaru IM, Silosi I, Vrabie CD, Tanasescu R (2010) Extra articular manifestations in rheumatoid arthritis. Maedica Journal 5(4): 286-291.
-
Arthritis Foundation (2017) Causes and Symptoms of Rheumatoid Arthritis.
-
Nishimura K, Sugiyama D, Kogata Y, Tsuji G, Nakazawa T, et al. (2007) Diagnostic accuracy of anti- cyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis. Annals of Internal Medicine 146(11): 797-808.
-
Finch A, Liang MH (2007) Anti-cyclic citrullinated peptide antibodies in the diagnosis of rheumatoid arthritis. Annals of Internal Medicine 146-816.
-
Luime JJ, Colin EM, Hazes JM, Lubberts E (2010) Does anti-mutated citrullinated vimentin have additional value as a serological marker in the diagnostic and prognostic investigation of patients with rheumatoid arthritis?. Annals of Rheumatic Disease 69(2): 337- 344.
-
Birch JT Jr, Bhattacharya S (2010) Emerging trends in diagnosis and treatment of rheumatoid arthritis. Primary Care 37(4): 779-792.
-
Sizova L (2008) Approaches to the treatment of early rheumatoid arthritis with disease-modifying antirheumatic drugs. British Journal of Clinical Pharmacology 66(2): 173-178.
-
Friestein GS (2012) Kelley’s Textbook of Rheumatology 9-1070.
-
Myasoedova E, Crowson CS, Kremers HM, Therneau TM, Gabriel SE (2010) IS the incidence of rheumatoid arthritis rising?. Arthritis Rheumatology 62(6): 1576- 1582.
-
Gibofsky A (2012) Overview of epidemiology, pathophysiology and diagnosis of Rheumatoid arthritis. American Journal of Managed Care 18(13): S295-302.
-
Ebringer A, Wilson C (1996) The use of low starch diet in the treatment of patients suffering from ankylosing spondylitis. Clinical Rheumatology 15(1): 62-66.
-
Wolfe F, Hawley DJ, Cathey MA (1990) Termination of slow acting antirheumatic therapy in rheumatoid arthritis: a 14-year prospective evaluation of 1017 consecutive starts. Journal of Rheumatology 17(8): 994-1002.
-
Chot HK, Hernan MA, Seeger JD, Robins JM, Wolfe F (2002) Methotrexate and mortality in patients with rheumatoid arthritis. Lancet 359(9313): 1173-1177.
-
Raza K, Filter A (2015) The therapeutic window of opportunity in rheumatoid arthritis. Annals of Rheumatology 74(5): 793-794.
-
Lard LR, Visser H, Spryer I, Vander Horst-Bruinsma IE, Zwinderman AH, et al (2001) Early versus delayed treatment in patients with recent onset of rheumatoid arthritis: comparison of two cohorts who received different treatment strategies. American journal of Medicine 111(6): 446-451.
-
Kris-Etherton PM, Harris WS, Apper IJ (2002) Fish consumption, fish-oil and omega-3 Fatty acids and cardiovascular disease. Circulation 106(21): 2747- 2757.
-
Linos A, Kaklamani VG, Kaklamani E, Koumantaki Y, Giziaki E, et al. (1999) Dietary factors in relation to rheumatoid arthritis: a role for olive oil and cooked vegetables. American Journal of Clinical Nutrition 70(6): 1077-1082.
-
Van den Ende CH, Hazes JM, Cessie SL, Mulder WJ, Belfor DG, et al. (2000) Comparison of high and low intensity training in well controlled rheumatoid arthritis. Annals of the Rheumatic Diseases 55(11): 798-805.
-
Vander Ende CH, Vliet Vlieland TP, Munneke M, Hazes JM (1998) Dynamic exercises in rheumatoid arthritis. British Journal of Rheumatology 37(6): 677-687.
-
Darmawan J, Raker HJ, Nuralim H (2003) Reduced burden of disease and improved outcome of Patients with rheumatoid arthritis. The Journal of Rheumatology 30(67): 50-53.
-
Carli C, Ehlin AGC, Klareskog L, Lindblad S (2006) Trends in disease modifying anti rheumatic drug prescription in early rheumatoid arthritis. Annals of Rheumatology 65(8): 1102-1105.
-
Carissa Flick, Jessica Farrell (2013) Issue of the Rheumatologist.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions