The Resurgence of African Viral Haemorrhagic Fevers (AVHFs) in Nigeria
AVHFs are a diverse group of animal and human illnesses that are caused by five distinct families of RNA viruses: the Arenaviridae, Bunyaviridae, Filoviridae, Flaviviridae and Togaviridae. Generally, VHFs are characterized by fever and bleeding disorders and all can progress to high fever, shock, haemorrhage and death in extreme cases. Infections with haemorrhagic fever viruses are an important cause of human illness and a public health problem of global dimension especially in the African continent. VHF agents are all highly infectious via the aerosol route, and most are quite stable as respirable aerosols. This means that they satisfy at least one criterion for being weaponized, and some clearly have the potential to be biological warfare threats. These viruses are found endemic in some areas of Africa, where they depend on animal, insect or natural reservoir for survival; they are usually restricted to the geographical area inhabited by their hosts and vectors. Currently, in Nigeria there are reports of the resurgence of these viral agents such as Lassa fever, Crimean-Congo haemorraghic fevers, Ebola and Rift Valley fever in some parts of the country.
Introduction
The African viral haemorrhagic fevers (AVHFs) are a diverse group of animal and human illnesses that are caused by five distinct families of RNA viruses: the Arenaviridae (Lassa, Lusaka-Johannesburg virus (LUJV) and Lusaka-Namwala (LUNA)-viruses first discovered in Zambia and South Africa) Bunyaviridae (Crimean-Congo, Rift Valley fever), Filoviridae (Ebola, Marburg), Flaviviridae (Dengue, Yellow fever) and Togaviridae (Chikungunya, O’Nyong-nyong) [1, 2]. All types of viral haemorrhagic fevers (VHFs) are characterized by fever and bleeding disorders and all can progress to high fever, shock, haemorrhage and death in extreme cases. The viruses cause significant outbreaks of diseases with person-to-person transmission. Some of the VHF agents cause relatively mild illnesses (Scandinavian Nephropathia epidemica), while others (African Ebola virus), can cause severe, life-threatening disease [3, 4]. Infections with haemorrhagic fever viruses are an important cause of human illness and a public health problem of global dimension especially in the African continent. These viruses are found endemic in some areas of Africa (Figure 1), since they depend on their animal, insect or natural reservoir for survival; they are usually restricted to the geographical area inhabited by their hosts and vectors [5].
![Figure 1: Map of Viral haemorrhagic fevers in Africa showing areas of known risk [6].](/fulltextimages/1423/fig_1.jpeg)
The viral haemorrhagic fevers prevalent in Africa (African Haemorrhagic Fevers, AHFs) comprise of
• The Arboviral (arthropod-borne) infections of Yellow
fever (YF), Rift Valley fever (RVF), Crimean-Congo haemorrhagic fever (CCHF); Chikungunya, O’Nyong- nyong and Nairobi Sheep disease virus.
- The Arenaviral (rodent-borne or robovirus) infection of Lassa fever (LASV)
- The Filoviral infections of Ebola (EBO) and Marburg virus disease (MARBV) haemorrhagic fevers. Each of these groups of VHFs has specific geographic patterns with vector and animal reservoirs (usually asymptomatic viraemic carriers). Although the individual disease pattern may differ for each virus, the VHFs may share many common features. They may be transmitted to humans through contact with infected animal, rodent or arthropod vectors [3, 4].
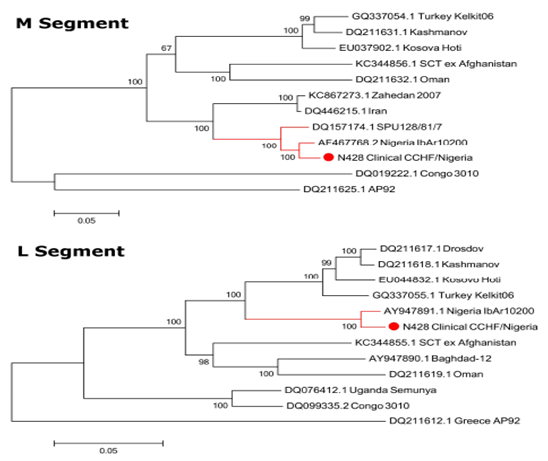
The distribution of the VHF viruses is generally limited and is endemic in certain areas of the world. Their geographical ranges may be highly circumscribed. Changing social, economic and climatic conditions such as the advent of jet travel resulting into increasing international travel, bioterrorism and ecological disruption coupled with human demographics increase the opportunity for humans to contact these infections and for introduction of VHF-associated viruses into new areas or increase the incidence in endemic areas [7, 8, 9]. The potential danger of transmission and importation of non-endemic VHFs has also been the focus of intense media attention and public concern [3]. The VHF agents are all highly infectious via the aerosol route, and most are quite stable as respirable aerosols. This means that they satisfy at least one criterion for being weaponized, and some clearly have the potential to be biological warfare threats. In Africa, AHFs usually do not cause major epidemics; however, localized outbreaks do occur and may have devastating effects on the local community and cause widespread concern. In addition to having high fatality rates, some also cause permanent disability, such as hearing loss following Lassa fever, or blindness after Rift Valley fever [10]. In Nigeria, there are reports from literature of serological and virological evidence of AHF virus activity in certain parts of the country among humans and animals [11, 12, 13, 14, 15, 16, 17, 18, 19, 20]. Previous virological and serological surveys in Nigeria have revealed the presence of human and animal infections by some of the viruses associated with haemorrhagic fevers [21]. These include YF Dengue 1 and 2 Congo of the Crimean-Congo haemorrhagic fever group RVFV LASV, Ebola and Marburg viruses [22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37]. Also since the first case of LF was reported in 1969, there have been reports of several outbreaks in many parts of the country [35, 36]. In 2017, between weeks 1 and 41, 569 suspected cases of Lassa fever with 120 Laboratory confirmed cases and 65 deaths (case-fatality rate, 11.4%) were reported from 86 Local Government Areas (LGAs) in 26 States compared with 87 Laboratory confirmed and 102 deaths (CFR,11.9%) from 138 LGAs of 28 States during the same period in 2016 [37]. Serologic and virological studies on some of the viral aetiologic agents of the AHFs indicate increasing prevalence and activities in recent years. RVFV antibodies have been found in sheep, goats, cattle, horses and camels in the northern States of Kaduna and Sokoto [38] and in the plateau area [15] suggesting that the virus may be enzootic in Nigeria. In addition, serological studies conducted on human sera have confirmed the existence of the disease in Nigeria [16, 19]. In one of these studies, conducted by Bukbuk et al. in 2014 among the human population in Borno Nigeria, RVFV antibodies (14.1%) were found to be more prevalent relative to antibodies against Lassa virus (7.4%) and CCHF virus (2.4%). The first report of CCHF in Nigeria occurred in 1970, when it was identified in various tick species, including Hyalomma spp. collected from market animals, and hedgehogs [19, 26]. However, very few cases of CCHF have been reported in Africa [39]; the majority are described from South Africa [40]. The risk of CCHF in several African countries is poorly defined and infection with the virus is often undiagnosed in these regions [41]. Of importance, CCHFV is a known to be a notorious cause of nosocomial infections especially when undiagnosed, and the virus presents a significant risk to health care workers [42, 43, 44, 45, 46]. However, despite several studies on the seroprevalence of antibodies against CCHFV from humans and animals in Nigeria, detailed investigation demonstrating the presence of IgG and IgM antibodies to the virus have not been reported until recently [20]. This study reported prevalence rates of IgG and IgM antibodies to be 10.6% and 3.5% respectively. This is also coupled with the fact that there have been no virological confirmations of human infection reported from Nigeria. The first virological or genomic analysis of CCHFV from sera of a 15-year-old female patient who presented with an undiagnosed febrile illness consistent with a case of VHF provided the first published evidence of a human case of CCHFV in Nigeria and its phylogenetic context [20]. CCHFV RNA obtained from this case (N428) was characterized by next generation sequencing (NGS) resulting in complete S.M. and L segment sequences. Phylogenetic analysis clustered the S segment in the Africa 3 phylogenetic group (Figure 2). The S segment open-reading frame showed close homology with a previous isolate of CCHFV from Nigeria (IbAr10200), as well as isolates from Mauritania (ArD39554) and South Africa (SPU415/85 and SPU128/61/7). The M and L clustered closely with the Sudan ABI-2009 isolate and the Nigeria IbAr10200 isolates (Figure 3).
![Figure 2: Maximum-Likelihood phylogenetic tree showing relationship distances obtained by comparing CCHFV S segment open-reading frames. Different CCHFV cladws are indicated by coloured lines [20].](/fulltextimages/1423/fig_2.jpeg)
References
-
Briese T, Paweska JT, McMullan LK, Hutchison SK, Street C, et al. (2009) Genetic detection and characterization of Lujo virus, a new haemorrhagic fever-associated Arenavirus from Southern Africa. PLOS Pathogens 5(5): 1000455.
-
Ishii A, Thomas Y, Moonga L, Nakamura I, Ohnuma A, et al. (2011) Novel Arenavirus, Zambia. Emerging Infectious Diseases 17(10): 1921-1924.
-
Jahrling PB, Zajtchuk R, Bellamy RF (1997) Textbook of Military Medicine: Medical aspects of chemical and biological warfare. Viral Hemorrhagic Fevers 591- 602.
-
Marty AM, Jahrling PB, Geisbert TW (2006) Viral Hemorrhagic Fevers. Clinical Laboratory Medicine 26(2): 345-386.
-
Public Health England (2014) Viral haemorrhagic fevers: epidemiology, characteristics, diagnosis and management.
-
https://www.gov.uk/government/uploads/system/u ploads/attachment_data/file/365845/VHF_Africa_96 0_640.png
-
Papa A, Benjiang M, Kouidou S, Tang Q, Hang C (2002) Genetic characterization of the M RNA segment of Crimean Congo Haemorrhagic Fever Virus strains, China. Emerging Infectious Diseases 8 (1): 50-53.
-
Sidwell RW, Smee DF (2003) Viruses of the Bunya- and Togaviridae families: potential as bioterrorism agents and means of control. Antiviral Res 57(1-2): 101-111.
-
Bakir M, Ugurlu M, Dokuzoguz B, Bodur H, Tasyaran MA, et al. (2005) Crimean-Congo haemorrhagic fever outbreak in Middle Anatolia: a multicentre study of clinical features and outcome measures. J Med Microbiol 54(4): 385-389.
-
WHO (1996) Rift Valley fever. Fact sheet N°207, Revised May 2010, World Health Organisation.
-
David-West TS, Cooke AR, David-West AS (1974) Sero-epidemiology of Congo virus (related to the virus of Crimean haemorrhagic fever) in Nigeria. Bulletin of the World Health Organisation 51(5): 543- 546.
-
Tomori O, Monath TP, O’Connor EH, Lee V, Cropp CB (1981) Arbovirus Infections among Laboratory personnel in Ibadan, Nigeria. Am J Trop Med Hyg 30(4): 855-861.
-
Umoh JU, Ezeokoli CD, Ogwu D (1983) Prevalence of antibodies to Crimean-Congo haemorrhagic virus in cattle in northern Nigeria. Int J Zoonoses 10(2): 151- 154.
-
Tomori O (1988) Lassa fever and other viral haemorrhagic disorders, UNESCO Serial article, Cat. No., 80828, series 150, pp: 115-128.
-
Olaleye OD, Tomori O, Schmitz H (1996a) Rift Valley fever in Nigeria: infections in domestic animals. Rev sci tech International Office of Epizootics 15(3): 937- 946.
-
Olaleye OD, Tomori O, Ladipo MA, Schmitz H (1996b) Rift Valley fever in Nigeria: infections in humans. Revue scientifique et technique International Office of Epizootics 15(3): 923-935.
-
Becker-Ziaja B, Folarin O, Phelan, Ehiane PE, Ifeh VE, et al. (2012) Molecular diagnostics for Lassa fever at Irrua Specialist Teaching Hospital, Nigeria: Lessons learnt from two years of laboratory operation. PLoS Negl Trop Dis 6(9): 1839.
-
Mylne AQ, Pigott DM, Longbottom, Joshua, Shearer F, et al. (2015) Mapping the zoonotic niche of Lassa fever in Africa. Trans R Soc Trop Med Hyg 109(8): 483-492.
-
Bukbuk DN, Fukushi S, Tani H, Yoshikawa T, Taniguchi S, et al. (2014) Development and validation of serological assays for viral hemorrhagic fevers and determination of the prevalence of Rift Valley fever in Borno State, Nigeria. Trans R Soc Trop Med Hyg 108(12): 768-773.
-
Bukbuk DN, Dowall SD, Lewandowski K, Bosworth A, Baba SS, et al. (2016) Serological and Virological Evidence of Crimean-Congo Haemorrhagic Fever Virus Circulation in the Human Population of Borno State, Northeastern Nigeria. PLoS Negl Trop Dis 10(12): 0005126.
-
Moore DL, Causey OR, Carey DE, Reddy S, Cooke AR, et al.(1975) Arthropod-borne viral infections of man in Nigeria, 1964-1970.Ann Trop Med Parasitol 69(1): 49-64
-
Monath TP, Mertens PE, Patton R, Moser CF, Baum JJ, et al. (1973) A hospital epidemic of Lassa fever in Zorzor, Liberia, March-April, 1972. Am J TroMed Hyg 22(6): 773-779.
-
Monath TP, Maher M, Casals J (1974) Lassa fever in eastern province of Sierra Leone. Am J Tro Med Hyg 23(6): 1140-1149.
-
Fagbami AH, Fabiyi A (1976) Epidemiology of Dengue infections in Nigeria: virus isolation and clinical observations, 1972-1975. J Trop Med Hyg 79(10): 226-228.
-
Fagbami AH, Monath TP, Fabiyi A (1977) Dengue virus infections in Nigeria: a survey for antibodies in monkeys and humans. Trans R Soc Trop MedHyg 71(1): 60-65.
-
Causey OR, Kemp GE, Madbouly MH, David-West TS (1970) Congo virus from domestic livestock, African hedgehogs, and arthropods in Nigeria. Am J Trop Med Hyg 19(5): 846-850.
-
Fagbami AH, Tomori O, Kemp GE (1973) Survey of Nigerian domestic and wild animals for serum neutralizing antibody to indigenous Rift Valley virus. Nigerian Veterinary Journal 2(2): 45-48.
-
Tomori O (1980) Rift valley fever virus infection in man in Nigeria. J Med Virol 5(4): 343-350.
-
Fisher-Hoch SP, Tomori O, Nasidi A, Perez-Oronoz GI, Fakile Y, et al. (1995) Review of cases of Nosocomial Lassa Fever in Nigeria: the high price of poor of medical practice. British Medical Journal 311(7009): 857-859.
-
Bajani MD, Tomori O, Rollin PE, Harry TO, Bukbuk ND, et al. (1997) A survey for antibodies to Lassa virus among health workers in Nigeria. Trans R Soc Trop Med Hyg 91(4): 379-381.
-
Omilabu SA, Badaru SO, Okokhere P, Asogun D, Drosten C, et al. (2005) Lassa fever, Nigeria, 2003 and 2004. Emerg Infect Dis 11: 1642-1644.
-
Fichet-Calvet E, Lecompte E, Koivogui L, Soropogui B, Dore A, et al. (2007) Fluctuation of abundance and Lassa virus prevalence in Mastomys natalensis in Guinea, West Africa. Vector Borne Zoonotic Dis 7(2): 119-128.
-
Ehichioya DU, Hass M, Ölschläger S, Becker-Ziaja B, Onyebuchi Chukwu CO, et al. (2010) Lassa fever, Nigeria, 2005–2008. Emerg Infect Dis 16(6): 1040- 1041.
-
Tomori O, Fabiyi A, Sorungbe A, Smith A, McCormick JB (1988) Viral hemorrhagic fever antibodies in Nigerian populations. Am J Trop Med Hyg 38(2): 407- 410.
-
http://www.promedmail.org 2007.
-
http://www.promedmail. 20150228.3199551.
-
http://www.ncdc.gov.ng/reports/weekly.
-
Ezeifeka GO, Umoh JU, Belino ED, Ezeokoli CD (1982) A serological survey for Rift Valley fever antibody in food animals in Kaduna and Sokoto States of Nigeria. Int J Zoonoses 9(2): 147-151.
-
Maltezou HC, Andonova L, Andraghetti R, Bouloy M, Ergonul O, et al. (2010) Crimean-Congo hemorrhagic fever in Europe: current situation calls for preparedness. Euro Surveill 15(10): 19504.
-
Swanepoel R, Struthers JK, Shepherd AJ, McGillivray GM, Nel MJ, et al. (1983) Crimean-congo hemorrhagic fever in South Africa. Am J Trop Med Hyg 32(6): 1407-1415.
-
Messina JP, Pigott DM, Golding N, Duda KA, Brownstein JS, et al. (2015) The global distribution of Crimean-Congo hemorrhagic fever. Trans R Soc Trop Med Hyg 109(8): 503-513.
-
Shepherd AJ, Swanepoel R, Shepherd SP, Leman PA, Blackburn NK, et al. (1985) A nosocomial outbreak of Crimean-Congo haemorrhagic fever at Tygerberg Hospital. Part V. Virological and serological observations. S Afr Med J 68(10): 733-736.
-
Conger NG, Paolino KM, Osborn EC, Rusnak JM, Gunther S, et al. (2015) Health care response to CCHF in US soldier and nosocomial transmission to health care providers. Emerg Infect Dis 21(1): 23-31.
-
Pshenichnaya NY, Nenadskaya SA (2015) Probable Crimean-Congo hemorrhagic fever virus transmission occurred after aerosol-generating medical procedures in Russia: nosocomial cluster. Int J Infect Dis 33: 120-122.
-
Naderi HR, Sheybani F, Bojdi A, Khosravi N, Mostafavi I (2013) Fatal nosocomial spread of Crimean-Congo hemorrhagic fever with very short incubation period. Am J Trop Med Hyg 88(3): 469-471.
-
Mardani M, Keshtkar-Jahromi M, Ataie B, Adibi P (2009) Crimean-Congo hemorrhagic fever virus as a nosocomial pathogen in Iran. Am J Trop Med Hyg 81(4): 675-678.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions