Should Mumps be Bumped up the Public Health Agenda in India?
Objectives: Mumps is a public health problem on a global scale. An effective vaccination exists, which is incorporated into routine immunisation schedules in over 100 countries, usually in the form of MMR for measles mumps and rubella. This is not the case in India, as mumps is not viewed as a significant enough public health problem by the government to warrant such intervention. This paper aims to add to the body of literature supporting routine immunisation with the mumps vaccine, positing that mumps is a significant enough public health problem to warrant such. Study Design: This paper presents a data set pertaining to mumps outbreaks in Kashmir, compiled by the Integrated Disease Surveillance Programme (IDSP). Methods: The number of mumps outbreaks was recorded, with cases diagnosed based on clinical signs and symptoms. Door to door visits occurred in the affected villages and schools, examining for signs and symptoms. Additionally, the living conditions and surroundings of the inhabitants were examined. The current rate of cases was compared to the background rate, and the outbreak described with respect to time, place and person. Results: From July 2017 to September 2017, there were 15 outbreaks and 260 cases of mumps recorded in the Kashmir region. Conclusions: We recommend that the MMR vaccination is included in the Universal Immunisation Programme (UIP). This would result in clinical and economic benefits, by reducing outbreaks and associated morbidity of mumps, concurrently tackling the recognised morbidity and mortality of rubella and measles.
Introduction
The Universal Immunisation Programme (UIP) of India does not include the MMR vaccination. It currently vaccinates against measles, however not rubella or mumps [1]. By presenting data collected from the Kashmir Region of India, this paper aims to add to the body of literature supporting inclusion of the mumps vaccination in the UIP on the basis that it is a significant public health problem. We posit that it would be worthwhile ensuring routine MMR vaccination, thereby ensuring robust immunisation against measles and rubella also, tackling associated morbidity, mortality and economic sequelae. Mumps is a viral infection caused by a paramyxovirus. The virus spreads through direct contact with respiratory secretions, saliva or through fomites. It replicates in the upper respiratory tract and the average incubation period is 16 to 18 days. Mumps primarily affects the salivary glands, causing pain, tenderness and swelling in one or both parotid glands. Prodromal symptoms may precede parotitis by several days, consisting of low grade fever, myalgia, anorexia, malaise and headache. Parotitis typically lasts for at least 2 days. Spread is enhanced by longer and closer contact with an infected individual. Therefore it is advised that an infected individual should avoid contact with others from the time of diagnosis until 5 days post-onset of parotitis [2]. Vaccination is recognised as the best way to prevent mumps. The first vaccine against mumps was licensed in the United States in 1967- it is a live attenuated vaccine, given as a simple subcutaneous dose, usually in MMR which is a combination of Measles, Mumps and Rubella. According to the UK Centers for Disease Control, two doses of mumps vaccine are 88% effective at preventing the disease, and one dose is 78% effective. Vaccinated cases are less likely to present severe symptoms or complications than under- or unvaccinated cases [3]. The World Health Organisation and Indian Association of Paediatrics (IAP) recognise the vaccine as a highly effective way of preventing infection- the IAP includes it on its vaccination schedule [4].
Indian Perspective
The Integrated Disease Surveillance Programme (IDSP) of India aims to strengthen and maintain decentralized laboratory based disease surveillance systems for epidemic prone diseases to monitor disease trends and to detect and respond to outbreaks promptly through trained Rapid Response Teams (RRTs) [5]. The Kashmir IDSP Division collected data for mumps outbreaks in Kashmir from January 2017 to September 2017, which is presented in this paper. The Universal Immunisation Programme (UIP) began in India in 1985. It was an extension to the Expanded Programme for Immunisation (EPI), which endeavoured to provide recommended vaccines against tuberculosis, polio and other diseases for all Indian children. The national policy of immunisation of all children during the first year of life with DPT, OPV and BCG- with the series of primary vaccination to be completed prior to the age of one- was adopted in 1978 with the launching of the EPI to increase the Immunisation coverage in infancy to 80%.The Ministry of Health and Family Welfare was responsible for the programme, with significant support from the international community. The UIP is one of the largest in the world in terms of quantities of vaccine used, the number of beneficiaries, the number of immunisation sessions organised, the geographical spread and the diversity of areas covered [6]. Advances in immunisation coverage have occurred, however not without management challenges. The Programme has not met the target of coverage for all children [7].
| Vaccination | Timing | ||||
| Bacillus Calmette Guerin | 1 Dose at birth (upto one year if not given earlier) | ||||
| Diphtheria, Pertussis, Tetanus Toxoid | 5 doses; Three primary doses at 6,10,14 weeks and two booster doses at 16-24 months and 5 Years of age | ||||
| Oral Polio Vaccine | 5 doses; 0 dose at birth, three primary doses at 6,10 and 14 weeks and one booster dose at 16-24 months of age | ||||
| Hepatitis B vaccine | 4 doses; 0 dose within 24 hours of birth and three doses at 6,10 and 14 weeks of age. | ||||
| Measles | 2 doses; first dose at 9-12 months and second dose at 16-24 months of age | ||||
| Tetanus Toxoid | 2 doses at 10 years and 16 years of age |
| The Current Vaccination Schedule Under the UIP is At present, the vaccination schedule (figure 1) does not include mumps.(6)Reasoning behind this is that it is not a significant enough public health problem. Despite being a widely prevalent disease in the country, it is considered | 000 cases, permanent sequelae occur in about 25% of | |
| encephalitis cases. Mumps is a leading cause of acquired | ||
| sensorineural deafness among children, affecting | ||
| approximately 5/100 000 mumps patients. Additionally, | ||
| mumps infection during the first 12 weeks of pregnancy is | ||
| associated with a 25% incidence of spontaneous abortion | ||
| [12,13]. |
Global Perspective
Studies have shown that 2 dose MMR coverage reduces disease severity and transmission alongside a reduction in complications and hospitalisation [9, 10]. Vaccination against mumps has been mandatory in Poland since 2003, ensuring 2 dose MMR coverage. Systematic execution of ensuring mumps vaccination resulted in a significant decrease in the number cases and further decline is expected [11]. By 2002 the mumps vaccination was included in the routine immunization schedule of 121 countries/territories. In countries where vaccination was introduced and high coverage was sustained the incidence of the disease has dropped tremendously and circulation has stopped. In countries where vaccination was not introduced the incidence of mumps remains high, mostly affecting children aged 5-9 years [12, 13]. Mumps has recognised associated complications. According to the WHO, although the case-fatality rate of mumps encephalitis is low and overall mortality is 1/10
Methods
The IDSP has been recording outbreaks of diseases including mumps. The epidemiological methods employed in this instance involved collecting the number of outbreaks and diagnosing cases based on clinical signs and symptoms. The WHO recommended clinical case definition is: ‘acute onset of unilateral or bilateral tender, self-limited swelling of the parotid or other salivary gland, lasting two or more days and without other apparent cause [12].’ Door to door visits occurred for patients in the affected villages and schools, examining for signs and symptoms. Additionally the living conditions and surroundings of the inhabitants were examined. The current rate of cases was compared to the background rate, and the outbreak described with respect to time place and person.
Results
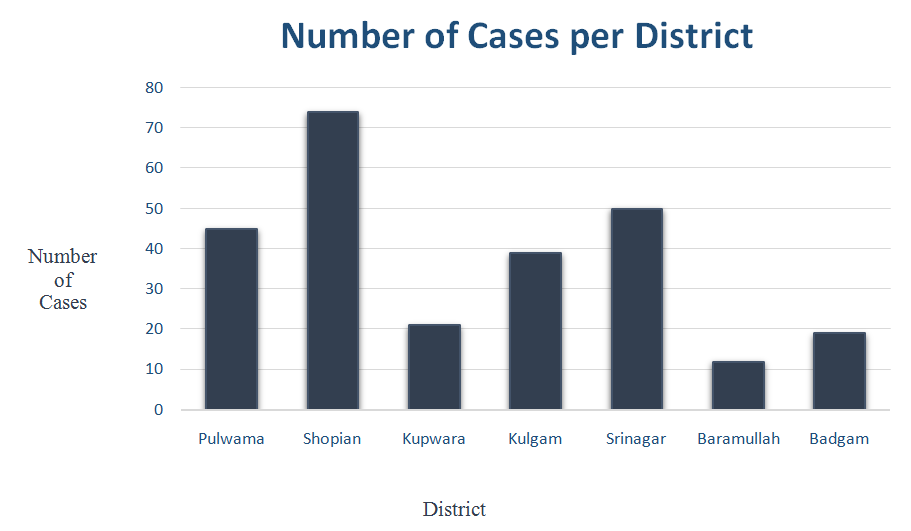
From July 2017- September 2017 15 outbreaks were recorded in the Kashmir region by the IDSP, totalling 260 cases (Figure 2). The outbreaks were across 7 districts in 15 villages. The minimum number of cases in an outbreak was 7 and the maximum 50, averaging 17 patients per outbreak.
| Outbreak Number | Date of Occurrence | District | Village Affected | Number of Cases |
| 1 | 17/07/2017 | Pulwama | Lasidaban | 10 |
| 2 | 24/07/2017 | Shopian | Naserpora | 25 |
| 3 | 27/07/2017 | Shopian | Tukroo | 11 |
| 4 | 15/08/2017 | Shopian | Pinjoora | 20 |
| S | 21/08/2017 | Kupwara | Bowan Zachaldar | 21 |
| 6 | 22/08/2017 | Pulwama | Abhama | 20 |
| 7 | 25/08/2017 | Kulgam | Lirrow | 7 |
| 8 | 26/08/2017 | Pulwama | Dogripora | 7 |
| 9 | 27/08/2017 | Pulwama | Wahipora | 8 |
| 10 | 28/08/2017 | Shopian | Harman Nildoora | 8 |
| 11 | 28/08/2017 | Srinagar | Govt Middle School, Khawja Bagh Maloora | 50 |
| 12 | 7/9/2017 | Baramullah | Sheeri Najibhat | 12 |
| 13 | 15/09/2017 | Shopian | Batpora | 10 |
| 14 | 16/09/2017 | Kulgam | Yaripora | 32 |
| 15 | 16/09/2017 | Badgam | Babapora | 19 |
Figure 2: Kashmir Mumps Outbreak Data. The largest outbreak was in an educational institution, in keeping with findings from existing literature which indicates that group settings associated with educational institutions are at increased risk of outbreaks, be they small or large [16]. The majority of outbreaks were recorded in the Shopian District, totalling 5 outbreaks with 74 cases overall (Figure 3).
Case Study: Intervention in Shopian District
To provide more context, an outbreak in Shopian District that was detected on the 15th August 2017 will be looked at in detail. Twenty cases were identified- the first case was reported on 14th August 2017 and clustering of cases occurred on 15th August 2017. The current rate of infection- 36.36%- was compared to background rate- 0%- by reviewing weekly IDSP data for the years 2016 and 2017. Interventions made due to the outbreak took the form of an info graphic and door to door surveys relaying education about transmission and prevention of the disease. Advice comprised:
- Keep affected children isolated from gathering
- Wash hands thoroughly with soap
- Keep affected children at home for 5 days and avoid close contact with others in house Additionally, health advisory pamphlets were distributed and pasted to public place walls (figure 4), a team of doctors was deployed to the area to identify and treat patients, schools were advised to avoid overcrowding, and field staffs were instructed to follow up affected children regularly until they were fully recovered. This outbreak only affected children, resulted in no hospitalisations or deaths, and no children developed major long-term sequelae.
![Figure 2: Kashmir Mumps Outbreak Data. The largest outbreak was in an educational institution, in keeping with findings from existing literature which indicates that group settings associated with educational institutions are at increased risk of outbreaks, be they small or large [16]. The majority of outbreaks were recorded in the Shopian District, totalling 5 outbreaks with 74 cases overall (Figure 3).](/fulltextimages/1794/fig_2.jpeg)
Discussion
Mumps vaccination is a proven way of preventing infection with the virus, reducing severity of disease if contracted, and reducing transmission.Two doses of the vaccine are 88% effective at protecting against mumps and one dose is 78% effective [3]. Waning immunity is a recognised issue, however on balance with the benefits of vaccination, this paper argues that this is not reason enough to choose not to routinely vaccinate. During mumps outbreaks in highly vaccinated communities, the proportion of cases that occur amongst the vaccinated population may be high. However this should not result in defaulting to the belief that the vaccine is not effective. The effectiveness of the vaccine is assessed by comparing the rate of infection in the vaccinated cohort to the rate of infection in the non- vaccinated cohort. In outbreaks in highly vaccinated populations, the non-vaccinated cohort tends to have a greater infection rate than the vaccinated cohort [3]. Given the existence of the MMR vaccination which is used in many countries globally, we suggest that the benefits of ensuring vaccination against mumps in addition to rubella and measles would be a logical public health intervention that would have highly significant clinical and economic benefits. It would ensure vaccination against mumps in addition to greater immunization rates against measles and rubella.
Conclusion
The Indian Government proposes that mumps is not a significant enough public health problem to warrant routine immunisation, however the data presented from Kashmir suggests otherwise. Environmental methods alone are clearly not preventing outbreaks. Whilst the case study of Shopian District did not have any hospitalisations or deaths, there is still recognised morbidity associated with mumps infection and potential lifelong sequelae for infected individuals, which is a public health concern. Whilst this paper acknowledges that there are other communicable diseases with greater associated morbidity and mortality, it proposes that given the existence of the MMR vaccination, mumps is a virus that could easily be vaccinated against in combination with measles and rubella, joining over 100 countries worldwide who routinely vaccinate against the virus. This paper should be taken into account alongside other literature within the body of evidence that proposes mumps as a significant enough public health problem to warrant investment in prevention through vaccination.
Acknowledgements
State Surveillance Officer (SSO) Kashmir wishes to thank Director Health Services Kashmir, Mission Director NHM and Deputy Director Schemes for their continuous support and motivation. My thanks to Chief Medical officers (CMOs), Medical Superintendents and District Health officers (DHOs) of all the districts of Kashmir Division for their support. Thanks to staff at District Surveillance Units (DSUs) in all the districts. Special thanks are extended to Staff at State Surveillance Unit, namely Ms. Irfana Bhat (DEO), for compilation of data.
Author Statements
We declare that this manuscript is original, has not been published before and is not currently being considered for publication elsewhere. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for- profit sectors. We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome. Ethical approval was not required for this paper as we present and analyze a data set obtained from other researchers that is properly anonymised. Informed consent was obtained at the time of original data collection. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
References
-
Universal Immunization Programme (UIP) (2017) National Health Portal of India.
-
Mumps (2017) Signs and Symptoms.
-
Mumps Vaccination (2017) CDC.
-
Indian Academy of Pediatrics (IAP).
-
India M. About IDSP: Integrated Disease Surveillance Programme (IDSP).
-
Universal Immunization Programme (UIP).
-
The Universal Immunisation Programme in India (2017) Centre for Public Impact.
-
Vashishtha V, Yadav S, Dabas A, Bansal C, Agarwal R, et al. (2015) IAP position paper on burden of mumps in India and vaccination strategies. Indian Pediatr 52(6): 505-514.
-
Levine H, Zarka S, Ankol O, Rozhavski V, Davidovitch N, et al. (2015) Seroprevalence of measles, mumps and rubella among young adults, after 20 years of universal 2-dose MMR vaccination in Israel. Hum Vaccin Immunother 11(6): 1400-1405.
-
Aasheim E, Inns T, Trindall A, Emmett L, Brown K, et al. (2014) Outbreak of mumps in a school setting, United Kingdom, 2013. Hum Vaccin Immunother 10(8): 2446-2449.
-
Janaszek Seydlitz W, Bucholc B, Gorska P, Slusarczyk J (2005) Mumps in Poland since 1990 to 2003; epidemiology and antibody prevalence. Vaccine 23(21): 2711-2716.
-
WHO (2017) WHO recommended surveillance standard of mumps.
-
Mumps (2017) World Health Organization.
-
Zamir C, Schroeder H, Shoob H, Abramson N, Zentner G (2015) Characteristics of a large mumps outbreak: Clinical severity, complications and association with vaccination status of mumps outbreak cases. Hum Vaccin Immunother 11(6): 1413-1417.
-
Vygen S, Fischer A, Meurice L, Mounchetrou Njoya I, Gregoris M, et al. (2016) Waning immunity against mumps in vaccinated young adults, France 2013. Euro Surveill 21(10): 30156.
-
Quinlisk M (2010) Mumps Control Today. The Journal of Infectious Diseases 202(5): 655-656.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions