Monitoring of Immune Response Following Covid-19 Vaccination
Introduction: SARS-CoV-2 is an infectious, viral, and contagious disease in which most patients present a mild respiratory condition whose recovery is autonomous and guided by the immune system itself. Objectives: The objectives of this research were to evaluate the immune system, the vaccination doses administered to the inhabitants of the parish of El Recreo, located in the Duran Canton of the Province of Guayas (Ecuador), according to age groups and gender, the vaccination coverage and the incidence of new diseases in the population under study. Material and Methods: This was a descriptive, non-experimental, prospective, cross-sectional, field study. It was carried out during the period from November 2021 to March 2022, during the pandemic of the "Omicron" variant. Results: the predominant age group corresponded to the range of 50-59 years (26.83% and 42; 29.79%) for both genders. We found (90.10%) of the population vaccinated. Another group (3.31%) did not receive the biologic and (6.59%) indicated that they were reluctant to receive the product. The second dose was administered to (83.5%) people in the community, while (14.28%) indicated having received the third dose. (3.04%) became ill after receiving the first doses; (2.63%) the second doses and none of those who received the third doses. It is necessary to alert the population of the need to benefit from the application of the vaccine since it seems to confer a certain degree of protection to the inhabitants and thus, the viral spread, hospitalization and death.
Introduction
SARS-CoV-2 is an infectious, viral, and contagious disease in which most patients present a mild respiratory condition whose recovery is autonomous guided by the immune system itself [1]; however, there are severe cases where immediate medical intervention is required [2].
In 2019, the coronavirus disease (COVID-19) affected public health worldwide, becoming a pandemic that has generated a major crisis in several areas of life, without discriminating against any social stratum [3]. This global emergency began in the city of Wuhan (China) at the end of December 2019 and spread to several countries until the World Health Organization (WHO) declared a global pandemic [4]. This virus in the period 2019-2022, has had several lethal and highly contagious mutations, causing several outbreaks throughout several countries, both developed and underdeveloped [5].
In Latin America, the first confirmed infection of a person with COVID-19 was in February 2020, in Brazil. Subsequently, nearby countries, such as Peru and Colombia, were acquiring infections until reaching an unprecedented increase in cases and deaths [6].
In Ecuador, preventive measures were taken to respond to the first reported case on February 29, 2020 [7], which triggered chaos in both institutions and citizens. The disease caused the collapse of health systems, which showed how unprepared the country was to face a pandemic of such magnitude [8]. The Ecuadorian territory was immersed in difficult months with affectation in all socio-cultural spheres, for which the country’s perspective was in dilemma and uncertainty.
Strenuous research by scientists led to the development of the first vaccines against COVID-19, in order to stop the wave of contagions [9]. The course of the vaccination process was a challenge to overcome, but today, more than 80% of the population over 5 years of age has the complete immunization schedule against COVID-19, providing an apparent protection against this pathogen and avoiding complications of the disease [10]. As time went by, the vaccine doses were doubled, since the immunity created by the first doses was decreasing, and new infections were observed in people who had already suffered from the disease [11, 12].
Several communications issued by the Atlanta Center for Disease Control (CDC) demonstrated the effectiveness of a third dose as a booster, indicating the prevention of severe disease and hospitalization due to a new Omicron variant, the fifth variant discovered, the first four being alpha, beta, gamma and delta, respectively. These findings demonstrated the possible benefit of the third booster dose, which protects against delta and Omicron variant, avoiding hospitalization in most cases [13].
Several experts have concluded from studies that the antibodies generated by the vaccines decrease with the passage of time, approximately 6 months after the application of the second dose, in which a decay of the values is observed [14]. Given this circumstance, these antibodies were no longer sufficient to neutralize the new variant, and a discussion was opened about including a third booster dose to help increase the serum levels of antibodies against the virus in question, thus contributing to a decrease in the number of infections [15]. Therefore, it is necessary to know scientific evidence to elucidate the problem, and in turn, to prove the reduction of the morbidity and mortality rate by COVID-19 in the province of Guayas.
In Ecuador, the issue of herd immunity was of great help, since a large part of the population acquired an immune response through collective contagion, probably due to the lack of social responsibility. After some time, when preliminary results of the vaccines were being observed, the wave of the Omicron variant was added [16]. This strain is more contagious but less lethal; from this moment on, a new discussion on the effectiveness of vaccines began [17].
On the other hand, there is the problem of managing pre-existing health conditions that affect the severity of COVID-19. The pandemic disproportionately exposes people of limited economic resources to make difficult choices, where due to the multiple deprivations that must be faced, they must choose between food and the purchase of medication to improve their health status. In this environment, an improvement in the acquisition and distribution of free medication to the population with underlying chronic diseases should be considered, as well as the possibility of expanding primary care services, both in the diagnosis and follow-up of risk factors among the population. In addition, little is known about the effectiveness of COVID-19 vaccines of different commercial brands such as Sputnik V, Sinovac and Sinopharm and their impact in the locality. Even less, if once exposed to the virus and immunized, it confers partial or total protection against acquiring new infections against other new strains. This information is essential for decision making and to generate concrete health actions in the face of the uncertainty of the population to continue to be immunized against a new variant.
The objectives of this research were to evaluate the effectiveness of vaccination of the inhabitants of the parish of El Recreo, located in the Daule Canton of the Province of Guayas (Ecuador), according to age and gender groups, vaccination coverage and incidence of new diseases in the population under study.
Materials and Methods
This was a descriptive, non-experimental, prospective, cross-sectional, field study. It was carried out from November 2021 to March 2022. Executed in the Province of Guayas, Canton Duran, parish of El Recreo, Ecuador. Carried out during the pandemic of the “Omicron” variant, which corresponded to December 14, 2022, date on which the first case of this variant was announced.
For the realization of this study, the research was structured in phases. For this, previous meetings were held with local health managers such as the Ministry of Public Health of Ecuador (MSP), the Autonomous Centralized Municipal Government (GAD) and other active forces of the canton, who took an active part in the study. Afterwards, meetings
Study Area
were held with community leaders of the Recreo parish to review the location of the houses and corroborate data such as number of houses, houses by blocks, uninhabited houses, among others. All this information was provided by the District Epidemiology Coordination, who participated in this preliminary reconnaissance. With the help of the sketches provided by this agency, we proceeded to select the dwellings by means of cluster sampling in a single block.
The homes were approached under strict biosecurity measures (Figure 1). The approach was carried out by a group made up of two nursing assistants, a laboratory assistant, two project researchers and the community leader corresponding to each block, together with two security personnel from the canton. Following informed consent, the information was recorded on an instrument designed for this purpose. For the application of both instruments in the community, the Bioethics Committee of the Health Intelligence Directorate (DIS), belonging to the Ministry of Public Health of Ecuador, approved the handling and processing of biological samples. The head or person responsible for the family nucleus was interviewed in each home. In addition, the following were established as inclusion criteria: 1) all heads of household regardless of age and gender 2) regardless of any marital status and occupation 3) being a resident of the study area for more than three years and exclusion criteria: being a resident of another canton or province of the country.
The following data were recorded in each household: weight, height, abdominal and brachial circumference, and the number of children who voluntarily decided to participate in the study. Samples were then taken for the determination of IgG and IgM antibodies to SARS - CoV2. 2019-nCOV/COVID-19. It was the Rapid IgG/IgM test device Hangzhou Realy Tech CO. LTD. The 2019-nCOV/COVID-19 IgG/IgM rapid test is a chromatographic immunoassay that allows the qualitative detection of IgG/IgM antibodies to coronavirus disease 2019, in human whole blood, serum or plasma as an aid in the diagnosis of COVID-19 infection. This test shows a Relative Sensitivity and Specificity of the IgG test of: 96% and 100% respectively. The Relative Sensitivity and Relative Specificity of the IgM test is 92% and 100%, respectively.
These determinations were carried out in the laboratory that operates in the Type C Orasmas Gonzalez Health Center. Then, a nasal swab was taken from those patients with a temperature increase above 38.5 ºC in order to perform the RT-PCR determination. Once a case was detected, epidemiological notification was made to fill out the form established by the Epidemiology Coordination and the samples were duly transported and processed at the Public
Results
Health Research Institute “Dr. Leopoldo Izquieta Pérez”, located in Guayaquil.
For the statistical analysis of the information, a format was designed in the program (Excel-Microsoft Office ®) that allowed obtaining and compiling the variables contained in the objectives of the study. Once the absolute frequencies were recorded, the relative frequencies were obtained and the mean of the population was calculated, it was related to the vaccination coverage with the presence of the new variant. All this information was represented in tables for subsequent analysis.
| Sex | ||||
|---|---|---|---|---|
| Age Group (Years) | Male | Female | ||
| Fa | Fr | Fa | Fr | |
| 18-29 | 3 | 7,32 | 20 | 14,18 |
| 30-39 | 3 | 7,32 | 18 | 12,77 |
| 40-49 | 5 | 12,20 | 30 | 21,28 |
| 50-59 | 11 | 26,83 | 42 | 29,79 |
| 60-69 | 10 | 24.39 | 19 | 13,48 |
| 70-79 | 8 | 19,51 | 9 | 6,38 |
| >80 | 1 | 2,44 | 3 | 2,13 |
| Total | 41 | 100,00 | 141 | 100,00 |
Table 1: Distribution of the population according to age groups and gender SOURCE: Study data The predominant age group in the st
Table 1: Distribution of the population according to age groups and gender SOURCE: Study data The predominant age group in the study area corresponded to the range of 50-59 years (n= 11; 26.83% and n= 42; 29.79%) for both genders. In second place, the 60-69 years age group (n=10; 24.39%) for the male sex and the 40-49 years age group (n=30; 21.28%) for the female sex. In third place, the categories of 70-79 years (n=8; 19.51%) for men and for women, the 60-69 years group (13.48%) (Table 1).
| Population | Fa (n) | Fr (%) |
|---|---|---|
| Vaccinated | 164 | 90,10 |
| Not vaccinated | 6 | 3,31 |
| Reluctant | 12 | 6,59 |
| Total | 182 | 100 |
Table 2: Total vaccinated and unvaccinated population. SOURCE: Study data Table 2 shows the distribution of the population interv
Table 2: Total vaccinated and unvaccinated population. SOURCE: Study data Table 2 shows the distribution of the population interviewed, which was classified as vaccinated, unvaccinated and reluctant. It was found that (n=164; 90.10%) were vaccinated. Another group (n=6; 3.31%) did not receive the biologic. Likewise, (n=12; 6.59%) indicated that they were reluctant to receive the product.
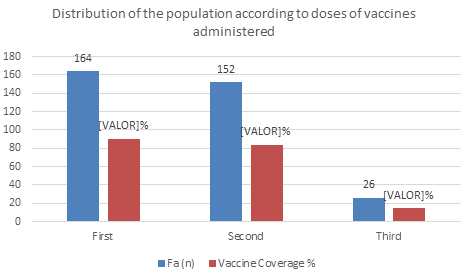
It was found that (n=164; 90.1%) of the population interviewed received the first dose of the vaccine. The second dose was administered to (n=152; 83.5%) people in the community. Meanwhile, (n=26; 14.28%) received the third dose (Figure 2).
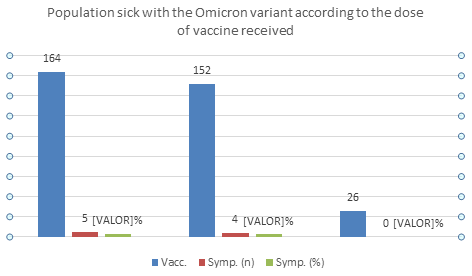
When the population that fell ill after the application of the respective doses was inspected, it was found that the individuals who received the first doses of 164 fell ill 5 (3.04%). When the second doses were applied, 4 became ill after having received 152 (2.63%). As for the third doses, 26 subjects who had received them reported that they had not reacquired another variant (Figure 3).
Discussion
The present work studied 182 people and analyzed the relationship between the doses of vaccine applied against SARS-CoV-2 and the development of COVID-19 disease in an urban parish whose demographic characteristics, such as population density, housing characteristics and lifestyles greatly favor the presence of the disease in the community. This research found that the most predominant age group was 50-59 years for both genders (26.83% and 29.79%). This result agrees with those obtained in a study of similar characteristics whose objective was to determine the effectiveness of vaccination against SARS-CoV-2 in preventing the development of disease and death due to COVID-19 in Córdoba, Argentina, in the period January-June 2021, in which the median (Md) age was 56 years (interquartile range [IQR], 40 to 69 years, since the interviewed groups were located between these age ranges [19]. Likewise, when evaluating the sample, it was found that the male gender predominated. These results are consistent with Herrera-Añazco, et al. [20] who have observed a lower intention to vaccinate among females. On the other hand, it differs from a study carried out in the state of Guerrero (Mexico) in a surveyed population (296 persons) in which the female gender predominated (65.20%) and in which the mean age plus standard deviation was 31.12 ±15.36 years [21].
In reference to the distribution of the vaccinated, non- vaccinated and reluctant population, it was evidenced that the majority of the population applied the vaccine against COVID (90.1%), while a minimum percentage did not receive the vaccine (3.31%) for various reasons, among which the population highlighted the harmful effects that these could cause and on the other hand the uncertainty, whether or not these actually granted total protection against the various variants of the disease. For this reason, they indicated that they refused to receive them. Similar results were obtained in a study carried out in several countries in 2021, among which, in a considerable number of national surveys [20], the aversion to the anticipated vaccine against COVID-19 varied in different countries: low in China (2 - 6 %) to very high in the Czech Republic and Turkey (43 % vs 44 %) respectively. They indicate that in most countries it was higher than usual. The reluctance to vaccinate, the authors point out, varies between countries such as Egypt and Russia (3%;55%) respectively [16]. They refer, among the reasons for reluctance to the application of the vaccine against COVID-19, the lack of knowledge and the fact that they accept them due to the uncertainty of getting sick, because of the limited information and refusing even if it is available because of the doubt about its effectiveness and safety.
Ecuador was one of the countries that stood out for being a pioneer in immunizing the population, since most of the population had a complete initial vaccination schedule when the Omicron variant appeared. Comparing figures in Ecuadorian territory, 83.36% of the population received the complete vaccination schedule against COVID 19, ranking fifth among 38 countries in Latin America and the Caribbean, while Chile ranked first with 88.47%, followed by Cuba, Uruguay, Argentina and Ecuador [10]. According to an article written by Moghadas, et al. [22] carried out in the United States, it explains that there was an increase in the application of doses after the first dose; either to complete the immunization scheme, infections, hospitalizations and deaths were avoided. We consider that good vaccination coverage was obtained in the parish under study, given that if in the community under study, 90.1% was reached with the application of the first dose and later, when receiving the second dose of the biologic, the figure of 83.5% was reached, similar to that obtained initially for the country, it could suggest that the population was sensitized and with it, the prevention of hospitalizations and deaths, due to the subsequent variant. On the other hand, the characteristics of the population studied, which is closely linked to lifestyles characteristic of a coastal locality in high growth, greatly favored the immunity initially acquired with the administration of the first dose in containing the spread of the virus [23].
Evidence shows that subsequent vaccines given against COVID provide the individual with superior immunity, thus preventing infection by a new variant, reinfection by a previously acquired variant or the presentation of more exacerbated symptoms. Studies support this theory, since, in a research conducted in the United States, there is evidence that booster doses applied to individuals provide excellent protection against the Omicron and Delta variants [24].
The initial doses of the vaccination scheme against COVID 19 contributed to the decrease in infections and the appearance of the disease, but in contrast with the appearance of the Omicron variant, a new window of discussion was opened on the effectiveness of the vaccine against other variants. In this regard, a study carried out by the United Kingdom Health Safety Agency (UKHSA) showed that most of the cases of Omicron in England coincidentally correspond to people who have received their complete vaccination schedule, also due to the different mass public events in various localities, causing new variants to be transmitted in the community [25]. In this sense, as in the present study carried out in the parish of El Recreo, in Guayaquil, Ecuador, it could be seen that the booster dose contributed greatly to immunity against this variant. Likewise, in an article published in The Lancet Infectious Diseases, entitled: Heterologous antibody response after vaccination with inactivated virus (BBIBP- CorV) in the elderly indicates that a third dose creates neutralizing antibodies against the Omicron variant, fighting this variant and thus decreasing the percentage of cases [26]. In this regard, bibliographic references on the effectiveness of third dose against the Omicron variant, a report published by the CDC, reveals that the booster dose has a 90% effectiveness in preventing hospitalization and death by Omicron [27]. This third dose is more beneficial because it provides greater immunity against COVID than the initial two doses alone [28].
In relation to the efficacy of the vaccines in the vaccinated population, a discrete number of people became ill again due to COVID (3.04% first dose) and (2.63% second dose) respectively. Clinical trials on the vaccines used have shown that they significantly reduce COVID-19 in vaccinated individuals with respect to unvaccinated control groups. In this regard, a study conducted by Scruzzim, et al. in 2021 reveals the effectiveness of vaccination against SARS-CoV-2 in preventing the development of disease and death from COVID-19 in Córdoba, Argentina, in the period January-June 2021, shows similarities with respect to our work; given that they report that of the total population vaccinated with one dose, 1.2% (n=7,829) contracted COVID-19; of the total number of people vaccinated with two doses, only 0.75% (n=1,245) developed the disease [19]. On the other hand, the European Medicines Agency, based on the COV002 studies conducted in the United Kingdom and COV003 in Brazil, stated that the efficacy of vaccination with ChAdOx1nCoV-19 (vaccine developed by the University of Oxford and AstraZeneca) reduced by 59.5% the number of people infected with SARS-CoV-2, with no hospitalizations recorded in people vaccinated with one or two doses, 22 days after its application [29].
As for the serological determinations carried out on the population, it was found that all the individuals who decided to participate voluntarily in the study showed a positive IgG determination (182/182) as opposed to negative IgM (170/182). It should be noted that confidentially 12 of the subjects were positive for both tests (IgG and IGM). The review also identified that 9 of these subjects had received one dose, 8 had received two doses and 3 had received three booster doses. The remaining three subjects received only two of the three booster doses. On the other hand, no case with temperature elevation above 38.5ºC was found during the approach.
It has been found that there are significant variations according to: number of people exposed to the virus, occupation, pre-existing disease and type of response obtained after the application of the biologic (first, second and third doses), but not according to the comorbidities present in the population. Thus, Azzolini, et al. [30], in dialyzed patients observed a reduction in the antibody response after months of the 2nd dose compared to healthy subjects (p<0.0001), but, however, the levels of neutralizing antibodies increased equally after the 3rd dose in participants with rheumatologic diseases and on dialysis. On the other hand, Pareja Cruz, et al. [31] in a study carried out in Peru, indicate that it seems that the vaccine, where most of the health professionals were male, 17.05% were 66 years old or older and 16.60% reported having had COVID-19 before being vaccinated with Sinopharm or Pfizer, allowed reinforcing the neutralizing antibody response in individuals previously diagnosed with COVID-19. In the present investigation carried out in the selected parish, in which they were vaccinated with Sinopharm, Pfizer or AstraZeneca, although a reduced number of the surveyed population indicated having received the third booster doses, the response of the informants indicated not having become ill with the Omicron variant, which could suggest that these doses achieved the desired immune response to avoid new infections by other variants of the virus.
In conclusion, the results obtained in the Parish of El Recreo, in Guayaquil, indicated that having received the vaccine, regardless of the type, decreased the probability of contracting the new variant, as well as decreasing the cases of severity and its complications, in addition, the protection was greater with the application of the second dose.
Acknowledgment
The authors wish to thank the inhabitants of the Recreo parish, especially Mrs. Rosa Zúñiga, leader of the community, for her permanent support, attitude and constancy, always present, which allowed us to achieve the objectives set for the realization of this study.
Conflict of Interest
The authors of this article declare that they have no conflicts of interest.
References
-
WHO (2020) Organización Mundial de la Salud. Coronavirus.
-
Alarcon R (2020) Perspectivas éticas en el manejo de la pandemia. Rev Neuropsiquiatr 83(2): 97-103.
-
Maguiña Vargas C, Gastelo Acosta R, Tequen Bernilla A (2020) El nuevo Coronavirus y la pandemia del Covid-19. Revista Medica Herediana 31(2): 125-131.
-
Orozco-Muñoz J, Tascón-Hernández J, Serrato-Yunda D, Alvear-Muñoz M (2022) Consideraciones especiales acerca de las intervenciones quirúrgicas durante la COVID-19. MEDISAN 26(3).
-
Hernández Fernández J (2021) La variante delta del COVID-19: ¿qué podemos esperar? Revista Mutis 11(2): 5-7.
-
Forero-Peña DA, Carrión-Nessi FS, Camejo-Ávila NA, Forero-Peña MJ (2020) COVID-19 en Latinoamérica: una revisión sistemática de la literatura y análisis bibliométrico. Revista de Salud Pública 22(2): 1-7.
-
(2020) Servicio Nacional de Gestión de Riesgos y Emergencias. SITUACIÓN NACIONAL POR COVID-19 (CORONAVIRUS).
-
Briones-Claudett KH, Murillo Vásconez RA, Rivera Salas C del R, Briones-Zamora KH, Briones-Márquez DC, et al. (2021) Management of COVID-19 at the pandemic’s first wave in Ecuador. SAGE Open Med Case Rep 9: 2050313X2110452.
-
Sardiña M (2020) EEUU prueba en humanos la primera vacuna experimental contra el Covid-19. France 24.
-
(2022) Ecuador ocupa el quinto puesto de vacunación COVID-19 entre 38 países de América y el Caribe. Ministerio de Salud.
-
Luzuriaga JP, Marsico F, Garcia E, González V, Kreplak N, et al. (2021) Impact of vaccines against COVID-19 on the incidence of new SARS-COV2 infections in health care workers of the Province of Buenos Aires. SciELO Preprints.
-
OMS (2022) Declaración para los profesionales de la salud: cómo se regulan las vacunas contra la COVID-19 para garantizar que son seguras y eficaces.
-
Thompson MG, Natarajan K, Irving SA, Rowley EA, Griggs EP, et al. (2022) Effectiveness of a Third Dose of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance - VISION Network, 10 States, August 2021–January 2022. MMWR Morb Mortal Wkly Rep 71(4): 139-145.
-
Gaus D (2021) COVID-19 Actualizacion Nueva variante, nuevas terapias, vacunas para niños. Práctica Familiar Rural 6(3).
-
Staneloni MI, Barcán LA (2021) Is a third dose of vaccine necessary for COVID-19? Revista del Hospital Italiano de Buenos Aires 41(4):196-198.
-
Fajardo P, Navarrete J, Marcillo S, García A (2022) Sars- Cov-2 variants: genomic characteristics. Ciencia Latina Revista Científica Multidisciplinar 6(1): 1744-1763.
-
Sánchez-Varela N, Cinza-Sanjurjo S, Portela-Romero M (2022) Reinfection by the Omicron variant in patients previously infected with the Delta variant of the SARS- CoV-2 coronavirus: an increasingly frequent reality in primary care. Family medicine Semergen 48(5): e35-e36.
-
Mapcarta (2022) Duran Municipality.
-
Scruzzi GF, Aballay LR, Carreño P, Díaz Rousseau GA, Franchini CG, et al. (2022) Vacunación contra SARS- CoV-2 y su relación con enfermedad y muerte por COVID-19 en Argentina. Revista Panamericana de Salud Pública 46: e39.
-
Herrera-Añazco P, Uyen-Cateriano A, Urrunaga-Pastor D, Bendezu-Quispe G, Toro-Huamanchumo C, et al. Prevalence and factors associated with the intention of vaccination against COVID-19 in Peru. SciELO Preprints.
-
Alcocer-Carranza J, Gonzalez-Carlo AL, Reyna-Avila L, Peña-Marcial E, Pérez-Cabañas R (2022) Attitude towards the vaccine against COVID-19 of the inhabitants of the state of Guerrero, Mexico. University and Health 24(2): 108-116.
-
Moghadas SM, Vilches TN, Zhang K, Nourbakhsh S, Sah P, et al. (2021) Evaluation of COVID-19 vaccination strategies with a delayed second dose. PLoS Biol 19(4): e3001211.
-
Thompson MG, Burgess JL, Naleway AL, Tyner HL, Yoon SK, et al. (2021) Interim Estimates of Vaccine Effectiveness of BNT162b2 and mRNA-1273 COVID-19 Vaccines in Preventing SARS-CoV-2 Infection Among Health Care Personnel, First Responders, and Other Essential and Frontline Workers — Eight U.S. Locations, December 2020–March 2021. MMWR Morb Mortal Wkly Rep 70(13): 495-500.
-
Accorsi EK, Britton A, Fleming-Dutra KE, Smith ZR, Shang N, et al. Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants. JAMA 327(7):639-651
-
Gregory A (202) More than half Omicron cases in England are in the double jabbed. The Guardian.
-
Rouco SO, Rodriguez PE, Miglietta EA, Rall P, Ledesma MMGL, et al. (2022) Heterologous booster response after inactivated virus BBIBP-CorV vaccination in older people. Lancet Infect Dis 22(8): 1118-1119.
-
(2023) Stay up-to-date with COVID-19 vaccinations, including booster doses. Centros para el Control y Prevención de Enfermedades.
-
Spitzer A, Angel Y, Marudi O, Zeltser D, Saiag E, et al. (2022) Association of a Third Dose of BNT162b2 Vaccine With Incidence of SARS-CoV-2 Infection Among Health Care Workers in Israel. JAMA 327(4): 341-349.
-
Picazo J (2021) Vacuna frente al COVID-19. Sociedad Espanola de Quimioterapia: infection y vacunas.
-
Azzolini E, Pozzi C, Germagnoli L, Oresta B, Carriglio N, et al. (2022) mRNA COVID-19 vaccine booster fosters B- and T-cell responses in immunocompromised patients. Life science alliance 5(6): e202201381.
-
Arturo PC, Julio César LE, Pedro Javier NM, Delgado Joel DL, Jesús Demóstenes GM (2022) Respuesta inmune humoral a cuatro vacunas contra el SARS-CoV-2 en profesionales de la salud. Horiz Med 22(2): e1937.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions