Use of the Multicriteria Decision Making Method in Establishing the Consequences of Breast Cancer Treatment
Objective: We present in this paper the results of multicriteria ranking of risk factors for depression, anxiety and stress in women with breast cancer. Method: The PROMETHEE/GAIA method was used for ranking purposes, with additional optimization of alternatives using the PROMETHEE method with inherent limitations. Results: Almost 50% of women with early breast cancer experienced depression, anxiety or both in the period of one year after the diagnosis; 25% in the second, third and fourth year; and 15% in the fifth year. Long-term depression and anxiety were associated with prior psychological treatment, absence of an intimate, confident relationship, younger age and severely stressful (non-cancer) events in life. A lack of intimate support in confidence also predicted prolonged episodes of depression and anxiety. Conclusion: Increased levels of depression, anxiety or both in the first year after the diagnosis of early breast cancer indicate the need for special support services during that period. Psychological intervention for women with breast cancer who no longer have the disease should take into account a broader social context of cancer occurrence, with a focus on the improvement of social support.
Introduction
Breast cancer is a global public health problem, not only due to its epidepic proportion, but also because its consequences affect all the segments in a society, from health care to psychosocial and socioeconomic ones. The epidemic wave of breast cancer hits hard both the developed and developing countries. The distribution, when the disease incidence is concerned, is almost equal, while the number of deaths in developing countries is higher by around 40% [1, 2].
In developed countries, more than 60% of the cases of breast cancer are detected in the stage of local disease, and less than 10% in more advanced stages [2]. Such a situation is directly reflected on the survival on the population level, which is 99% in the USA for localized disease; 84% for locoregional disease; and 23% for the stage with distant metastases [2]. For our country, there are no data of this kind. Numerous analyses have shown that five-year survival in breast cancer depends mostly on the economic development of a country in question [3].
In view of a high degree of probability of survival with breast cancer, the question of the quality of life of the survivors becomes very important. Quality of life assessment is an integral part of therapeutic pšrocedure and patient follow-up and makes possible the insight into therapeutic sequelae and other dysfunctions. In contrast, quality of life does not correlate often with objective clinical parameters, since it basically represents a subjective view of the patient.
The information about the impact of psychological factors on cancer prognosis are available. It appears that psychological status is a predictor of the length of survival in several types of cancer. Longer follow-ups show that a stronger fighting spirit does not offer any advantages in the sense of survival, while in patients who are disease-free after 5 years, their initial reaction of helplessness/hopelessness still has a significant effect on 5-(and up to 10)year disease- free survival rates [4]. The results of one eight-year follow-up study of 10.000 patients have demonstrated that coexistence of cancer and depression is associated with a higher risk of death [5]. Therefore, untreated depressive disorders can be associated with more rapid disease progression [6].
Methods
The study took place at the Day Hospital of the Clinic of Oncology, University Clinical Center Niš, involving the patients with the diagnosis of breast cancer treated in the period from 2014 to 2019. The control group consisted of 50 depressive women without breast cancer, treated at the Special Hosital for Psychiatric Diseases in Gornja Toponica.
For sample calculations, we used the literature data of average MADRS scores among breast cancer patients (13.4±10.3) and in controls (8.3±7.9) [7]. The calculated minimal sample size required to produce satisfactory statistical power was 140 patients (or aided by the calculator, where the sample for the Municipality was calculated to be 153 examinees) [8].
For the purpose of this study, two groups of examinees were formed. The first group of cases consisted of 160 patients with the diagnosis of breast cancer. Out of these,
120 consented to participate in the study (75%), while the other 40 did not give their consent due to lack of personal interest. Six patients died in the period of 6 months and were excluded from the analysis.
The testing of these patients took place at the Day Hospital of the Clinic of Oncology 6 months after their oncological therapy. The patients were aged 18 to 65 years [9, 10, 11].
The second, control group, comprised 50 women without breast cancer, aged 18 to 65 years, in whom depression was diagnosed. The sample (studied and control group) was approximately stratified by the age of examinees.
The patients were informed about all the aspects of the study using the information leaflet. The study involved 153 examinees – 103 (67.3%) women with breast cancer (studied group) and 50 (32.0%) women with depression and without breast cancer (as controls). The average age of the whole studied population was 49.2±11.2 years (age range, 26 to 65 years). Age structure of the examinees did not statistically significantly, i.e. the groups were homogenous (studied group: 49.4±10.8; control group: 48.76±12.21 years; t=0.329; p=0.734).
Results
Use of the PROMETHEE/GAIA (Preference Ranking Organisation Method for Enrichment Evaluation – Geometrical Analysis for Interactive Assistance) methodology in this paper was represented by the example of the effect of psychiatric problems in patients treated for breast cancer [12].
The choice of an appropriate psychiatric problem is performed through the following six phases:
- Social factors
- Disease-related factors (depression, anxiety and stress)
- Disease phase
- Type and histopathological type of the malignancy
- Possibility for an adequate therapy
- Possibility for rehabilitation The sum of measurable criteria for the assessment of suggested methods should involve the availability of patient medical records, availability of social, health care and educational services, as well as the safety aspects.
| Alternative | Criteria | |||||
|---|---|---|---|---|---|---|
| 95% CI | Cases of mental disorders | Age at mental disorder diagnosis (years) | Personality type | Personal beliefs regarding malignancy | Disease phase | |
| Depression (% of patients) | 0.091(max- 0.025 | 1.80% | 49.20±11,2 | 1 | 1 | 2 |
| Anxiety (% of patients) | 0.083 0.23 | 1.30% | 49.01(11,6) | 2 | 2 | 2 |
| Stress-related disorders (% of patients) | 0.079 0.022 | 0.80% | 47.7(10.5) | 2 | 3 | 1 |
Table 1: Characteristics of the process of psychiatric problems in breast cancer patients.
In order to perform calculations in this example, the Decision Lab software was used that can graphically represent the obtained results of alternative ranking. Figure 1 [13] presents the initial (tabulatory) data in that software.
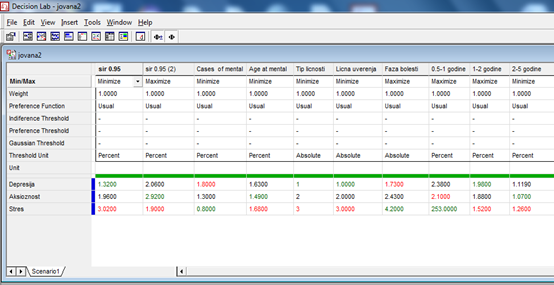
From the presented data, we had three alternatives to choose medical (psychic) problems, with six present criteria given in Table 1. The last two criteria were qualitative ones. In order to quantify the qualitative values of the location criteria we used a 5-cypher scale with the following meanings: 1 – very poor; 2 – poor; 3 – satisfying; 4 – good; 5 – very good. Some of the criteria needed to be minimized, while the rest needed to be maximized.
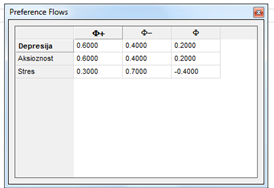
Based on the calculated positive (entry) and negative (exit) preference courses, Figure 2. we performed partial ranking by the PROMETHEE I method.
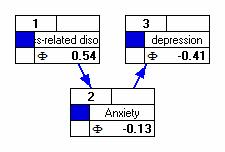
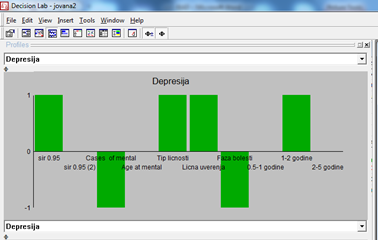
The Decision Lab program presented the results graphically (Figure 3). The obtained graph suggested that the alternative of depression predominates over all other alternatives. PROMETHEE I did not compare conflicting actions.
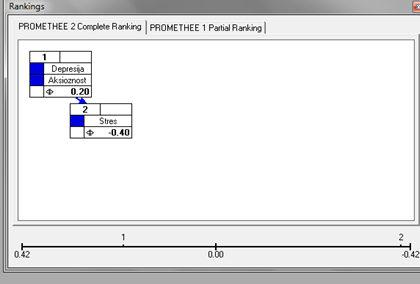
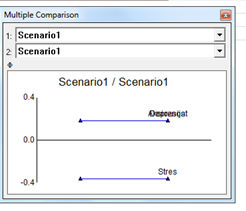
The PROMETHEE II method provides decision-makers with the opportunity to perform a complete alternative ranking, as depicted in the Figure 4. Based on this figure, a conclusion can be drawn that the order of alternatives is as follows: Depression → Stress → Anxiety. Both methods offer a strong support to decision-makers in the process of problem-solving.
It is quite obvious that PROMETHEE I and PROMETHEE II methods perform ranking based on the assigned weight coefficients. A special option of the software, termed „The walking weights“ enables modification of initial weights and observation of resulting modifications during ranking with the assistance of the PROMETHEE II method (Figure 5). A decision-maker is thus able to simply perform an analysis of the sensitivity of the obtained results.
A graphical analysis of the obtained results can be seen as well in Figure 6.
A specialized data processing software, D-sight, was used for the result analysis. The platform onto which the D-sight software is being developed is closely related to the PROMETHEE method. D-sight enables simplification of the PROMETHEE method analytical model through the following steps: entry of alternatives, entry of criteria, entry of weight coefficients for individual criteria, entry of alternatives weights and their normalization, determination of the criteria functions, and maximization or minimization of the criteria and reading of the results [5].
A graphical representation of results processing was obtained using the Global Visual Analysis (GVA) and was presented in Figure 7. The information related to the complex problem of decision-making containing k of the criteria, can be presented in a k-dimensional space. The GAIA plane represents a plane obtained after the projection of the whole information into two-dimensional space. In the GAIA plane, alternatives are presented as triangles, and criteria as squares. The red dot marks the approximative value of all criteria weights and visually presents an optimal point which the offered alternatives are trying to reach. Conflicting criteria characteristics are depicted in the diagram; conflicting criteria are oriented in the opposite direction, while the criteria with similar preferences are oriented in the same direction. As an addition in the representation of alternatives and criteria of the weight vector projections in the GAIA plane, there is a corresponding Pi vector, showing the direction of compromising results. A large number of offered criteria led to a crowded and unclear graphical representation of the obtained results in Figure 7. Regardless of that, however, it could be seen that the action 1, i.e. depression, was the one closest to the Pi plane.
Our reading of the solutions obtained by the application of the PROMETHEE method of multicriteria decision-making, with the support of the D-Sight software, confirmed that depression was most prevalent, followed by stress, and then anxiety (Figure 2).

Based on the position of alternatives and criteria, it could be seen that all the criteria were very conflicting with one another (different directions of the axes). The direction indicated that the first alternative was a best one. The method could further be applied to the other phases.
Discussion
Almost 50% of women with early breast cancer have had depression, anxiety or both in the year following the diagnosis of their disease; 25% in the second, third and fourth year; and 15% in the fifth year. The prevalence was 33% at diagnosis, dropping to 15% after a year. Out of those relapsing, 45% experienced depression, anxiety or both in the period of three months after the diagnosis.
The results of a large epidemiological study of Mehnert et al. have shown that as high as 42% of patients with breast cancer have a mental health problem [14]. At a special risk are the patients on chemotherapy (as a sole treatment modality), in whom anxiety and/or depression are more prevalent [15, 16, 17]. Similar results were obtained in a study which compared the presence of depression and anxiety in patients or chemotherapy and radiation therapy [18].
In this paper, we investigated the presence of depressivity, anxiety and stress symptoms in breast cancer patients after six months and after five years. Numerous studies in breast cancer patients have so far examined mostly their prevalence and intensity, using the classical statistical methods to correlate them with sociodemographic and clinical patient characteristics, feasibility of their clinical assessment and the effects of various approaches of psychosocial support [19, 20, 21, 22, 23, 24].
In this paper, we presented the theoretical postulates of the PROMETHEE method and the use of the approach illustrated on the example of effects of psychiatric problems in patients treated for breast cancer. Utilization of the methods is considerably facilitated by the use of Decision Lab software, which provides final results in a simple and quick way, assuring also a clear and descriptive graphical representation of the results [6]. However, although this is a high quality method, the success in the application of the PROMETHEE method largely depends on the following factors:
- ability and experience of the decision-maker in expressing one’s own preferences between the alternatives on an interval scale per each considered criterion;
- willingness of the decision-maker to take into account all the criteria relevant for decision-making, being aware that the obtained solution will in fact represent the best compromise between all the analyzed criteria;
If these prerequisites are fulfilled, the PROMETHEE I and II method can become a useful tool to a decision-maker, able to offer strong support in the process of resolving complex problems in multicriteria decision-making [4, 6, 7, 8, 9].
In this large registry-based study, we discovered that breast cancer patients had 60% higher risk for the development of depression, anxiety and stress-related disorders.
Although the risk of mental disorders was greatest immediately after the diagnosis of their disease, the incidence of all three mental disorders remained increased in the following 5 years. Younger age at diagnosis, comorbid conditions, higher histological grade, positive lymphonodal status and chemotherapy were all independently associated with the risk of depression and anxiety in breast cancer patients; histological grade and chemotherapy contributed only to short-term risk, while comorbid conditions were mostly related to late-onset events. Younger age at diagnosis was the only recognizable risk factor for stress-related disorders in breast cancer patients. We were not able to establish an overall increased risk of mental disorders in breast cancer patients, except for an increased risk of stress- related disorders in the 6 months after the diagnosis.
Conclusion
The results of this study contribute to the awareness that another approaches as well in the definition of a particular psychiatric problem have an important impact on the efficiency in establishing the symptoms of depressivity, anxiety and stress.
Due to its prevalence and a huge public health impact, breast cancer will be the topic of interest in scientific work in the University Clinical Center.
References
-
Mather A, Rodriguez C, Guthrie MF, McHarg AM, Reиd IC, et al. (2002) Effects of exercise on depressive symptoms in older adults with poorly responsive depressive disorder. The British Journal of Psychiatry 180: 411-415
-
Siegel R, Naishadham D, Jemal A (2012) Cancer Statistics, 2012. CA Cancer J Clin 62(1): 10-29.
-
Li CI (2010) Breat cancer epidemiology. Springer Scienec, New York.
-
Drummond FJ, Kinnear H, Donnelly C, O’Leary E, O’Brien K, et al. (2015) Establishing a population-based patient- reported outcomes study (PROMs) using national cancer registries across two jurisdictions: the Prostate Cancer Treatment, your experience (PICTure) study. BMJ Open 5(4): e006851.
-
Kav S, Schulmeister L, Nirenberg A, Barber L, Johnson J, et al. (2010) Development of the MASCC teaching tool for patient receiving oral agents for cancer. Support Care Cancer 18(5): 583-590.
-
Somers RM, Miller K, Berry DL (2012) Feasibility pilot on medication adherence and knowledge in ambulatory patients with gastrointestinal cancer. Oncol Nurs Forum 39(4): E373-E379.
-
Sajjad S, Ali A, Gul RB, Mateen A, Rozi S (2016) The effect of individualized patient education, along with emotional support, on the quality of life of breast cancer patientsa pilot study. Eur J Oncol Nurs 21: 75-82.
-
Park JH, Bae SH, Jung YS, Kim KS (2012) Quality of life and symptom experience in breast cancer survivors after participating in a psychoeducational support program: a pilot study. Cancer Nurs 35(1): E34-E41.
-
Cvetković J, Kovačevic SI, Cvetkovic M, Cvetković S (2020) Evaluation of the role of stress in patients with breast cancer and depression by paykel’s life event and adaptive neuro‐fuzzy approach. Brain and Behavior 10(4): e01570.
-
Cvetkovic J, Cvetkovic M (2019) Evaluation of UML diagrams for test cases generation:Case study on depression of internet addiction. Physica A: Statistical Mechanics and its Applications 525: 1351-1359.
-
Cvetkovic J (2018) Depression in patients with breast cancer (Meeting Abstract). European Psychiatry 48: S408-S408.
-
Brans JP, Mareschal B, Vincke P (1984) PROMETHEE: A new family of outranking methods in multicriteria analysis. Operational Research 3: 477-490.
-
Geldermann J, Zhang K (2001) Software review: Decision Lab 2000. WOL 10: 317-323.
-
Cvetković J, Nenadović M (2016) Depression in breast cancer patients. Psychiatry Research 240: 343-347.
-
Nikbakhsh N, Moudi S, Abbasian S, Khafri S (2014) Prevalence of depression and anxiety among cancer patients. aspian J Intern Med 5(3): 167-170.
-
Caruso R, Nanni MG, Riba MB, Sabato S, Mitchel AJ, et al. (2017) Depressive spectrum disorders in cancer: prevalence, risk factor and screening for depression: a critical review. Acta Oncol 56(2): 146-155.
-
Wdowiak A, Makara-Studzińska M, Raczkiewicz D, Cyranka K (2022) Reproductive problems and intensity of anxiety and depression in women treated for infertility. Psychiatr Pol 56(1): 153-170.
-
So WKW, Marsh G, Ling WM, Leung FY, Lo JCK, et al. (2010) Anxiety, depression and quality of life among Chinese breast cancer patients during adjuvant therapy. Eur J Oncol Nurs 14(1): 17-22.
-
Mehnert A, Brahler E, Faller H, Harter M, Keller M, et al. (2014) Four-week prevalence of mental disorders in patients with cancer across major tumor entities. J Clin Oncol 32(31): 3540-3546.
-
Roser M, Ritchie H, Spooner F (2019) Burden of Disease [Internet]. Our World in Data.
-
Krebber AMH, Buffart LM, Kleijn G, Riepma IC, deBree R, et al. (2014) Prevalence of depression in cancer patients: a meta-analysis of diagnostic interviews and self-report instruments. PsychoOncology 23(2): 121-130.
-
Tsaras K, Papathanasiou IV, Mitsi D, Veneti A, Kelesi M, еt al. (2018) Assessment of depression and anxiety in breast cancer patients: prevalence and associated factors. Asian Pacific Journal of Cancer Prevention 19(6): 1661-1669.
-
Jimenez-Fonseca P, Calderon C, Hernandez R, Cajal TRY, Mut M, at al. (2018) Factors associated with anxiety and depression in cancer patients prior to initiating adjuvant therapy. Clin Transl Oncol 20(11): 1408-1415.
-
Singer S, Danker H, Roick J, Einenkel J, Briest S, et al. (2017) Effects of stepped psychooncological care on referral to psychosocial services and emotional well- being in cancer patients: a cluster-randomized phase III trial. Psychooncology 26(10): 1675-1683.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions