Nasopharyngeal Carcinoma (NPC) in Russia and Epstein - Barr Virus Types: Analysis of the Influence of Gender, Ethnic and Age Factors on the Virus Types Spread in NPC Patients
Introduction: The discovery of two molecular types of Epstein-Barr virus, EBV-1 and EBV-2, with different biological properties, stimulated the search for new neoplasms associated with each type of the virus. Objective: The aim of this study was to analyze the prevalence of EBV-1 and EBV-2 in NPC patients from different climatic and geographical regions of Russia, representatives of different gender, ethnic and age groups of patients. Materials and Methods: Using nested PCR EBV types were determined in blood plasma of NPC and other non-EBV-associated tumors of the oral cavity (OTOC/EBV-) patients from the North Caucasus (NCFD) and the Central (CFD) Federal Districts of Russia. IgG and IgA antibody titers to viral capsid antigen (VCA) were determined by indirect immunofluorescence. Results: The studies carried out have shown that NPC and OTOC/EBV- patients were infected with both EBV types in roughly the same ratio. There were also no statistically significant differences in serological activities of NPC patients infected with EBV-1 or EBV-2. The prevalence of EBV-2 types 1 and 2 was not influenced by gender or ethno-geographic affiliation of NPC patients. The only difference was EBV-2 predominance in NPC patients under 60, and EBV-1 predominance in those over 60 years old. Conclusion: The absence of a predominance of one of the EBV types in NPC patients indicates that neither EBV-1 nor EBV-2 is strictly NPC-associated in Russia, and that different ethnic and climatic-geographical factors in the spread of virus types in NPC patients are not playing an essential role.
Introduction
It is known that the Epstein-Barr virus (EBV) permanently infects over 95% of the adult population worldwide. In most cases, EBV infection is asymptomatic, and the virus typically persists in a latent state in memory B-cells [1]. However, there is substantial evidence that the virus is involved in the development of malignant neoplasms of lymphoid and epithelial origin. Based on this evidence, the International Agency for Research on Cancer (IARC) has classified EBV as a Group 1 carcinogen, meaning it has direct carcinogenic effects on humans [2].
Among the epithelial neoplasms associated with EBV, nasopharyngeal carcinoma (NPC) occupies a special place, being one of the most common cancers in the southern provinces of China and Southeast Asian countries (25-30 cases per 100,000 people per year). NPC is less common among Arabs in North Africa, indigenous peoples of Greenland, Alaska, and relatively rare in most European countries and the United States [3]. In Russia, the incidence rate of NPC is 0.1-0.2% of the overall cancer morbidity, with rates of 0.55 for males and 0.29 for females per 100,000 population [3]. Established risk factors for NPC, apart from early childhood infection, include host genotype, male gender, and a family history of NPC. Risk factors also include high consumption of preserved foods (such as salted fish in China and Russia), as well as the presence of specific human leukocyte antigen (HLA) class I alleles in the infected individual [4, 5]. It is also important to note that the histological variant of the tumor associated with EBV is predominantly non-keratinizing and undifferentiated.
The mechanism of carcinogenesis in EBV-associated NPC is largely determined by the functional characteristics of the virus itself, which require further investigation. It has been shown that EBV exhibits dual tropism, infecting both B-lymphocytes and epithelial cells. Infection of both cell types in the nasopharyngeal tonsils is an important step in establishing viral persistence in the body [6, 7]. The lytic phase of infection in epithelial cells promotes viral replication and progeny spread, while latent infection of these same cells allows the virus to evade detection and immune system-mediated destruction, potentially leading to tumor development. Importantly, the expression of latent EBV genes is only possible in immortalized epithelial cells with altered activity in specific cellular genes (such as cyclin-D and p16), which contribute to overcoming cell cycle arrest. Moreover, the expression of latent genes also occurs in the presence of local inflammation and the inflammatory cytokine TGF-1 [8, 9]. These findings suggest that the malignant transformation of EBV-infected epithelium requires not only a specific host genotype but also the acquisition of genomic and epigenetic changes by the epithelial cells.
The arising tumor cells of epithelial origin often undergo lysis with release of viral progeny because of reactivation of the virus within them [10]. This is evident from high concentrations of EBV DNA in the blood plasma and elevated levels of IgG and IgA antibodies to viral antigens [11]. The process of EBV reactivation in tumor cells also contributes to the progression of NPC. This is due to the release of viral proteins that cause cellular genome instability, integration of the virus into areas of the cellular genome located near tumor-suppressor and inflammation-related genes, as well as the activation of vascular endothelial growth factor (VEGF) production, and so on [12, 13, 14]. Thus, while the latent genes of the virus ensure the survival of NPC tumor cells, the lytic phase of infection promotes tumor progression through genome instability and angiogenesis.
The encoded by the virus nuclear protein EBNA1 plays an important role in EBV-associated carcinogenesis. It has recently been discovered that in cells latently infected with EBV, EBNA1 binds to EBV-like sequences on fragile site 11 of the human chromosome, and increased levels of EBNA1 on this chromosome lead to its destruction. The consequence of this event became evident after whole-genome sequencing of 2439 malignant neoplasms belonging to 38 nosological forms. It was found that tumors associated with EBV demonstrate higher levels of chromosome 11 abnormalities, and these abnormalities are found in 100% of patients with NPC [15].
The discovery of two types of Epstein-Barr virus (EBV-1 and EBV-2 or types A and B) based on genetic differences in the genes encoding nuclear proteins EBNA-2, EBNA-3a, and EBNA-3c prompted a series of studies aimed at elucidating the biological properties of these virus types [16, 17, 18, 19]. In particular, it has been shown that EBV-1, unlike EBV-2, has the ability to transform B lymphocytes in vitro, while EBV- 2 is characterized by a unique cell tropism for T cells [20]. It was also found that EBV-2 easily infects mature CD3 T cells of humans in vitro, remaining in a latent state in these cells [21]. Moreover, the consistent detection of EBV-2 in T cells of patients with Burkitt lymphoma in Kenya and New Guinea, as well as its infection rate of over 20% in healthy Kenyan infants, indicates that EBV-2 infection of T cells is a natural part of the life cycle of this virus type. It may also be a necessary condition for realizing the oncogenic potential of this type of virus. [22]. These observations led to the hypothesis that each of the viral types, EBV-1 and EBV-2, uses alternative approaches to establish its latency - a stage preceding the development of malignant neoplasms - in the in vivo situation. Support for this hypothesis is provided by the fact that EBV-2 infection in humanized mice, previously vaccinated with human umbilical cord blood CD34 stem cells, led to the development of B-cell lymphoma resembling human diffuse large B-cell lymphoma in the majority of them [23]. The above-described and other data served as a basis for studies trying to establish the connection between each of the two viral types and specific EBV-associated neoplasms, and the ability to establish a more aggressive malignant phenotype in one of them [24].
According to literary data, EBV-1 infects the majority of EBV-positive Burkitt lymphomas in Brazil, dominates among patients with NPC in China, nasal and peripheral T-cell lymphomas in Taiwan, and predominates among EBV- positive cases of Hodgkin lymphoma in England, etc [25, 26, 27]. At the same time, EBV-2 is more frequently detected in patients with immune suppression of various origins [28]. Despite existing data on the preferential persistence of one type of EBV in a specific pathology, the contribution of each type to the carcinogenesis process remains largely understudied.
Since both EBV types and NPC incidence are characterized by geographic and ethnic variability, determining the contribution of each virus type to NPC development in genetically distinct populations from different geographic regions is an important task [29]. Based on the above, the aim of this study was to investigate the nature of the association between EBV-1 and EBV-2 with NPC in patients from the Central and North Caucasus federal districts of Russia, located in geographically and climatically different regions of the country with diverse ethnic composition of the population. In addition, it was important to determine the gender and age characteristics of the association with virus types, serological response to them in NPC patients.
Materials and Methods
Study Subjects
Study Material
The objects of the study were samples of blood plasma from patients with non-keratinizing undifferentiated histological variant of nasopharyngeal carcinoma (NPC) associated with Epstein-Barr virus (EBV) from the North Caucasus (NCFD) and Central (CFD) Federal Districts of the country (26 and 31 cases, respectively). As controls, 50 samples of blood plasma from patients with oral cavity tumors not associated with EBV (non-EBV-associated oral cavity tumors, OTOC/EBV-) were studied. These included neoplasms of the oral cavity mucosa, tongue, palate, sublingual tonsil, and cases of NPC with keratinizing differentiated histological variant of tumor not associated with EBV from the same Federal districts (27 and 23 cases, respectively). All patients were treated at the N.N. Blokhin National Medical Research Center of Oncology of the Ministry of Health of Russia. Blood sampling from patients was conducted with their consent and was approved by the Ethics Committee of the N.N. Blokhin National Medical Research Center of Oncology of the Ministry of Health of Russia.
EBNA-2 Genotyping by Nested PCR
EBNA-2 genotyping for EBV-1 and EBV-2 types in the samples of patients’ blood plasma was performed using a “nested” PCR, following the previously described method with minor modifications [30]. The primers used demonstrated high specificity of testing and absence of cross-reactivity with the human genome and other viruses or microorganisms [31].
Serological Test for EBV Antibodies
Titers of IgG and IgA antibodies to EBV capsid antigen (VCA) were determined in the plasma of patients using the indirect immunofluorescence method (the so-called “gold standard”), the conditions of which and the measurement of the obtained results were described earlier [32]. The antibody titers are presented as their mean geometric values (MGV).
Statistical Analysis
The number of EBV-1 and EBV-2 sequences in the studied blood plasma samples of NPC and OTOC/EBV-patients was assessed with the Mann-Whitney U-test. Using Fisher’s exact test, the P value was calculated by comparing the values of the percentage of EBV-1 and EBV-2 genotypes for the studied groups of patients; the differences were considered statistically significant at P≤ 0.05. Calculations were performed using statistical packages “Statistica for Windows, 10.0”.
Results
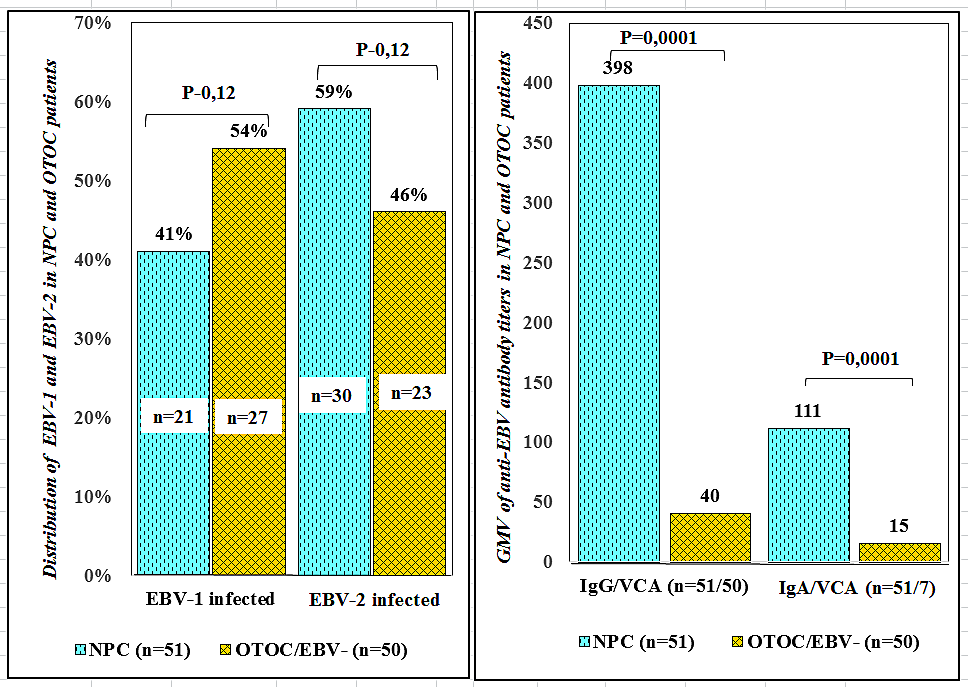
In order to determine the association of NPC with EBV types in Russia, plasma samples from NPC and OTOC/EBV- patients, representatives of the North Caucasus (NCFD) and Central (CFD) Russian Federal Districts, were tested for the presence of EBV-1 and EBV-2 copies. In addition, titers of IgG and IgA antibodies to viral capsid antigen (VCA) of EBV were determined in plasma samples from above patients. The obtained data are shown in Figure 1, which shows that the prevalence of EBV-1 was higher in OTOC/EBV- patients (54%; 27/51 compared to 41%; 21/51 in NPC patients). In contrast, EBV-2 was more dominant in NPC patients (60%; 30/50 compared to 46%; 23/50 in OTOC/EBV- patients). However, the differences between the percentage of the number of EBV-1 and EBV-2 copies in patients with NPC and OTOC/EBV- turned out to be statistically insignificant (P=0.12). Figure 1 also shows that the titers of IgG and IgA antibodies to VCA were significantly higher in NPC patients compared to OTOC/EBV- patients (P<0.0001 and P<0.0001, respectively). These findings indicate that NPC patients do not have a preferential association with either type of EBV, at the same time confirming the strong NPC association with EBV.
To analyze the biological activity of each EBV type, the serologic response was studied in two groups of NPC patients infected with either EBV-1 or EBV-2. As shown in Figure 2, higher titers of IgG and IgA antibodies to VCA were detected in NPC patients infected with EBV-2 compared to those infected with EBV-1 (383 and 102 compared to 312 and 80, respectively). The differences in the corresponding values
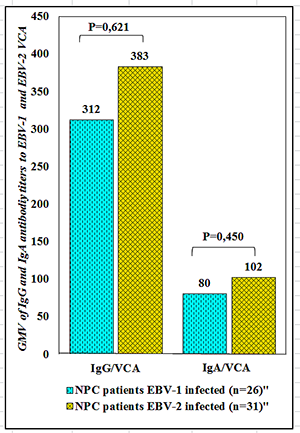
between the two groups of NPC patients were statistically insignificant, although there was a tendency towards higher activity of EBV-2 compared to EBV-1. Further investigation of additional properties of EBV-1 and EBV-2 using a larger sample size may provide a more accurate determination of the biological activity of each of these types of viruses.
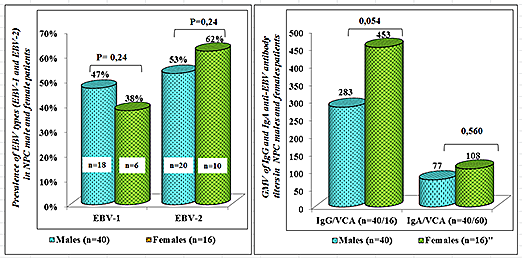
Taking into account the peculiarities of physiological and metabolic processes in men and women, it seemed important to find out whether a preferential association with one of the EBV types there is in representatives of the two genders of NPC patients. The data presented in Figure 3 indicate that men are slightly more frequently infected with EBV type 1 (47% versus 38% in women), while women are more frequently infected with EBV type 2 (62% versus 53% in men), but the differences in the percentage of EBV-1 and EBV-2 in the male and female groups were statistically insignificant (P=0.24). Despite higher VCA IgG and IgA antibody titers in women (453 and 108 versus 283 and 77 in men), the differences in these comparable indicators were also statistically insignificant (0.054 and 0.560, respectively). These findings suggest that gender differences do not influence the susceptibility of NPC patients to specific EBV types.
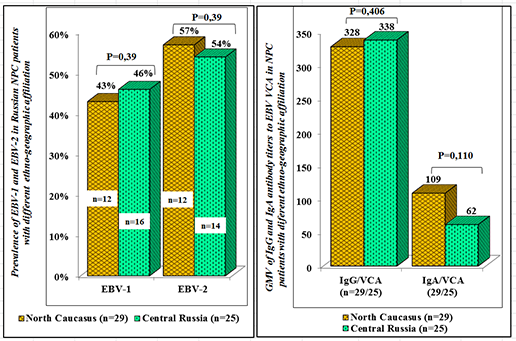
The influence of genetic factors and environmental triggers on the pattern of EBV-1 and EBV-2 infection was studied in NPC patients from North Caucasian (NCFD) and Central (CFD) Federal Districts of Russia. As mentioned above, these Federal Districts are located in different climatic and geographical regions of the country and are populated by genetically distinct populations - mainly numerous Caucasian and Slavic ethnic groups, respectively. The analysis conducted (Figure 4) showed that the prevalence of EBV infection in NPC patients from both Federal Districts was higher for EBV-2 compared to EBV-1 (55% and 54% versus
45% and 46%, respectively), although the differences in the prevalence of EBV-1 and EBV-2 among the two ethnic groups were statistically insignificant (P=0.39). The geometrical mean titers of VCA IgG and IgA antibodies to EBV in NPC patients from the NCFD and CFD were also statistically insignificant (P=0.406 and P=0.110, respectively). These findings suggest that the genetic characteristics of NPC patients and environmental factors do not significantly influence the distribution of EBV types and the serological response to them in NPC patients.
It is known that the human immune system functions at its maximum capacity from 16-18 to 55-60 years old, and its activity gradually declines in later years. This decline can be accompanied by the activation of EBV replication, which is a risk factor for the development of EBV-associated malignancies such as Kaposi’s sarcoma, Castleman’s disease, and various lymphomas including Hodgkin’s and non- Hodgkin’s lymphomas. To elucidate the features of the EBV-1 and EBV-2 distribution, as well as the serological activity of both viral types in the host organism depending on age, two groups of NPC patients aged up to 60 (n=11; mean age 44.1 years) and older than 60 were studied (n=31; mean age 71.5 years). The analysis showed (Figure 5) that patients over 60 years old were significantly more often infected with EBV-1 (55% vs 48% type 2; P=0.01), while patients under 60 years old were significantly more often infected with EBV-2 (52% vs 45% type 1; P=0.01). It was also found that the levels of IgG and IgA antibodies to viral capsid antigen (VCA) were higher in the group of patients under 60 years old (320 and 99 vs 265 and 58, respectively), but the differences between these levels were not statistically significant (P=0.310 and P=0.242, respectively).
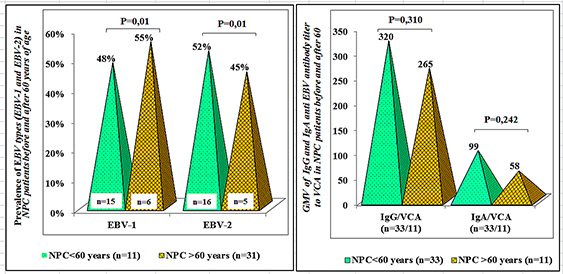
Figure 5: EBV types and serological markers in NPC patients before and after 60 years of age. Discussion The conducted research allowed identifying a practically indistinguishable pattern of association between EBV- 1 and EBV-2 in NPC and OTOC/EBV- patients as well as in NPC patients of two genetically different populations from different geographical and climatic regions of Russia. There were no gender differences in the distribution of virus types among NPC patients. In addition, in NPC patients mono- infected with EBV-1 and EBV-2, approximately the same serological activity of the virus against VCA was detected. There was also no dominance of any virus type in NPC patients with different sizes of primary tumor, tumor- involved lymph nodes, and disease stages (data not shown). The only difference found was a higher prevalence of EBV-1 in NPC patients over 60 years of age and EBV-2 in patients under 60 years, an observation that appears to need further study with more patients in each age group to confirm or refutation of the data obtained.
The obtained data overall suggest the absence of a dominant role of any EBV type in the development of NPC in Russia. The differences in the gene sequences of EBNA- 2, EBNA-3A, and EBNA-3C, which provide some functional characteristics to the type 1 and type 2 viruses, are not associated with the acquisition of NPC -specific properties by either of them, nor with the loss of oncogenic potential The predominantly observed infection with type 1 viruses in most EBV-positive Burkitt’s lymphomas in Brazil, Hodgkin’s lymphomas in England, and non-Hodgkin’s lymphomas in China, as well as the regular detection of type 2 viruses in T-cells of Burkitt’s lymphomas in Kenya and New Guinea, is likely not related to tumor-specific properties of the local virus types [22, 25, 26, 27]. It is more likely the result of dominant persistence of one virus type in the corresponding populations of specific geographical regions. Testing healthy individuals in these regions for EBV-1 and EBV-2 could clarify this issue.
Attempts to detect the existence of EBV variants specifically associated with specific human tumors have been made by many researchers, but so far have been unsuccessful. However, it is not possible to completely exclude the existence of EBV strains etiologically associated with the development of certain neoplasms. An example of this is the recently isolated EBV strain M-81 from a Chinese NPC patient, which is characterized by a high affinity for epithelium [33]. This viral property increases the likelihood of infection of the nasopharyngeal epithelium and the development of cancer in this anatomical area. In this regard, the search for EBV variants specific to certain types of tumors in endemic regions among different ethnic groups is justified. The complexity of the task, however, lies in the fact that the identification of high-risk EBV strains, similar to human papillomaviruses (HPV-16, HPV-18), is difficult due to the heterogeneity of its viral genes, the joint functioning of which likely leads to the acquisition of oncogenic potential by the virus.
Conclusion
The varying prevalence of EBV types (EBV-1 and EBV-2) worldwide is determined by many factors, including genetic characteristics of populations. Factors influencing the selection of EBV types in vivo include immune surveillance by the host organism and the major histocompatibility complex (MHC) type. Since predominant MHC types differ between ethnic groups and populations from different geographic regions, these factors may play a significant role in determining structural modifications of EBV and its types [34, 35, 36].
The absence of dominance of one the EBV types in the NPC patients we studied suggests that the type of the virus does not play a fundamentally important role in the development of NPC in Russia. It is likely that each of these types, EBV-1 or EBV-2, is capable of manifesting its oncogenic potential but only under the necessary conditions. However, the search for oncogenic tumor-specific variants of EBV in Russia remains a relevant task, as the detection of a virus with specific organ tropism would contribute to the development of an effective vaccine for successful management of corresponding neoplasms.
Funding
The study was supported by a grant from the Russian Science Foundation (project no. 23-25-00435).
Acknowledgments
The authors express their deep and sincere gratitude to Evgeny Matyakin, Mikhail Kropotov, and Ali Mudunov, professors of the Department of Head and Neck Tumors at the N.N. Blokhin National Medical Research Center of Oncology, Ministry of Health of Russia, for their comprehensive clinical support for this study.
Conflict of Interest: The authors declare no conflict of interest.
Ethical Approval: The study protocol was approved by the Ethics Committee of the N.N. Blokhin National Medical Research Center of Oncology, Ministry of Health of Russia (Protocol No. 532 of 14.04.2022).
References
-
Higgins CD, Swerdlow AJ, Macsween KF, Harrison N, Williams H, et al. (2007) A study of risk factors for acquisition of Epstein-Barr virus and its subtypes. J Infect Dis 195(4): 474-482.
-
Chen CJ, You SL, Hsu WL, Yang HI, Lee MH, et al. (2021) Epidemiology of Virus Infection and Human Cancer. Recent Results Cancer Res 217: 13-45.
-
Yu MC, Yuan JM (2002) Epidemiology of nasopharyngeal carcinoma. Semin Cancer Biol 12(6): 421-429.
-
Lo KW, To KF, Huang DP (2004) Focus on nasopharyngeal carcinoma. Cancer Cell 5(5): 423-428.
-
Wei WI, Kwong DLW (2010) Current management strategy of nasopharyngeal carcinoma. Clin Exp Otorhinolaryngol 3(1): 1-12.
-
Borza CM, Hutt-Fletcher LM (2002) Alternate replication in B cells and epithelial cells switches tropism of Epstein- Barr virus. Nat Med 8(6): 594-599.
-
Hutt-Fletcher LM (2007) Epstein-Barr virus entry. J Virol 81(15): 7825-7832.
-
Tsang CM, Zhang G, Seto E, Takada K, Deng W, et al. (2010) Epstein-Barr virus infection in immortalized nasopharyngeal epithelial cells: regulation of infection and phenotypic characterization. Int J Cancer 127(7): 1570-1583.
-
Tsang CM, Yip YL, Lo KW, Deng W, To KF, et al. (2012) Cyclin D1 overexpression supports stable EBV infection in nasopharyngeal epithelial cells. Proc Natl Acad Sci USA 109(50): E3473-E3482.
-
Yip YL, Lin W, Deng W, Jia L, Lo KW, et al. (2018) Establishment of a nasopharyngeal carcinoma cell line capable of undergoing lytic Epstein-Barr virus reactivation. Lab Invest 98(8): 1093-1104.
-
Twu CW, Wang WY, Liang WM, Jan JS, Jiang RS, et al. (2007) Comparison of the prognostic impact of serum anti-EBV antibody and plasma EBV DNA assays in nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys 67(1): 130-137.
-
Chiu SH, Wu CC, Fang CY, Yu SL, Hsu HY, et al. (2014) Epstein-Barr virus BALF3 mediates genomic instability and progressive malignancy in nasopharyngeal carcinoma. Oncotarget 5(18): 8583-8601.
-
Xu M, Zhang WL, Zhu Q, Zhang S, Yao YY, et al. (2019) Genome-wide profiling of Epstein-Barr virus integration by targeted sequencing in Epstein-Barr virus associated malignancies. Theranostics 9(4): 1115-1124.
-
Hong GK, Kumar P, Wang L, Damania B, Gulley ML, et al. (2005) Epstein-Barr virus lytic infection is required for efficient production of the angiogenesis factor vascular endothelial growth factor in lymphoblastoid cell lines. J Virol 79(22): 13984-13992.
-
Li JSZ, Abbasi A, Kim DH, Lippman SM, Alexandrov LB, et al. (2023) Chromosomal fragile site breakage by EBV- encoded EBNA1 at clustered repeats. Nature 616(7957): 504-509.
-
Rowe M, Young LS, Cadwallader K, Petti L, Kieff E, et al. (1989) Distinction between Epstein-Barr virus type A (EBNA 2A) and type B (EBNA 2B) isolates extends to the EBNA 3 family of nuclear proteins. J Virol 63(3): 1031- 1039.
-
Sample J, Young L, Martin B, Chatman T, Kieff E, et al. (1990) Epstein-Barr virus types 1 and 2 differ in their EBNA-3A, EBNA-3B, and EBNA-3C genes. J Virol 64(9): 4084-4092.
-
Feederle R, Klinke O, Kutikhin A, Poirey R, Tsai MH, et al. (2015) Epstein-Barr Virus: From the Detection of Sequence Polymorphisms to the Recognition of Viral Types. Curr Top Microbiol Immunol 390(Pt 1): 119-148.
-
Palser AL, Grayson NE, White RE, Corton C, Correia S, et al. (2015) Genome diversity of Epstein-Barr virus from multiple tumor types and normal infection. J Virol 89(10): 5222-5237.
-
Rickinson AB, Young LS, Rowe M (1987) Influence of the Epstein-Barr virus nuclear antigen EBNA 2 on the growth phenotype of virus-transformed B cells. J Virol 61(5): 1310-1317.
-
Coleman CB, Wohlford EM, Smith NA, King CA, Ritchie JA, et al. (2015) Epstein-Barr virus type 2 latently infects T cells, inducing an atypical activation characterized by expression of lymphotactic cytokines. J Virol 89(4): 2301-2312.
-
Young LS, Yao QY, Rooney CM, Sculley TB, Moss DJ, et al. (1987) New type B isolates of Epstein-Barr virus from Burkitt’s lymphoma and from normal individuals in endemic areas. J Gen Virol 68(Pt 11): 2853-2862.
-
Coleman CB, Lang J, Sweet LA, Smith NA, Freed BM, et al. (2018) Epstein-Barr Virus Type 2 Infects T Cells and Induces B Cell Lymphomagenesis in Humanized Mice. J Virol 92(21): e00813- e00818.
-
Neves M, Marinho-Dias J, Ribeiro J, Sousa H (2017) Epstein-Barr virus strains and variations: Geographic or disease-specific variants?. J Med Virol 89(3): 373-387.
-
Klumb CE, Hassan R, De Oliveira DE, De Resende LMM, Carrico MK, et al. (2004) Geographic variation in Epstein- Barr virus-associated Burkitt’s lymphoma in children from Brazil. Int J Cancer 108(1): 66-70.
-
Wu SJ, Lay JD, Chen CL, Chen JY, Liu MY, et al. (1996) Genomic analysis of Epstein-Barr virus in nasal and peripheral T-cell lymphoma: a comparison with nasopharyngeal carcinoma in an endemic area. J Med Virol 50(4): 314-321.
-
Gledhill S, Gallagher A, Jones DB, Krajewski AS, Alexander FE, et al. (1991) Viral involvement in Hodgkin’s disease: detection of clonal type A Epstein-Barr virus genomes in tumour samples. Br J Cancer 64(2): 227-232.
-
Boyle MJ, Sewell WA, Sculley TB, Apolloni A, Turner JJ, et al. (1991) Subtypes of Epstein-Barr virus in human immunodeficiency virus-associated non-Hodgkin lymphoma. Blood 78(11): 3004-3011.
-
Chang CM, Yu KJ, Mbulaiteye SM, Hildesheim A, Bhatia K (2009) The extent of genetic diversity of Epstein-Barr virus and its geographic and disease patterns: a need for reappraisal. Virus Res 143(2): 209-221.
-
Hassan R, White LR, Stefanoff CG, De Oliveira DE, Felisbino FE, et al. (2006) Epstein-Barr virus (EBV) detection and typing by PCR: a contribution to diagnostic screening of EBV-positive Burkitt’s lymphoma. Diagn Pathol 1: 17.
-
Salahuddin S, Khan J, Azhar J, Whitehurst CB, Qadri I, et al. (2018) Prevalence of Epstein-Barr Virus Genotypes in Pakistani Lymphoma Patients. Asian Pac J Cancer Prev 19(11): 3153-3159.
-
Gurtsevitch V, Ruiz R, Stepina V, Plachov I, Le Riverend E, et al. (1986) Epstein-Barr viral serology in nasopharyngeal carcinoma patients in the USSR and Cuba, and its value for differential diagnosis of the disease. Int J Cance 37(3): 375-381.
-
Tsai MH, Raykova A, Klinke O, Bernhardt K, Gartner K, et al. (2013) Spontaneous lytic replication and epitheliotropism define an Epstein-Barr virus strain found in carcinomas. Cell Rep 5(2): 458-470.
-
Burrows JM, Bromham L, Woolfit M, Piganeau G, Tellam J, et al. (2004) Selection pressure-driven evolution of the Epstein-Barr virus-encoded oncogene LMP1 in virus isolates from Southeast Asia. J Virol 78(13): 7131-7137.
-
Lin HJ, Cherng JM, Hung MS, Sayion Y, Lin JC (2005) Functional assays of HLA A2-restricted epitope variant of latent membrane protein 1 (LMP-1) of Epstein-Barr virus in nasopharyngeal carcinoma of Southern China and Taiwan. J Biomed Sci 12(6): 925-936.
-
Gurtsevitch VE, Senyuta NB, Ignatova AV, Lomaya MV, Kondratova VN, et al. (2017) Epstein-Barr virus biomarkers for nasopharyngeal carcinoma in non- endemic regions. J Gen Virol 98(8): 2118-2127.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions