Hepatitis E; An Emerging Killer
Hepatitis E, caused by the Hepatitis E virus, is a highly contagious disease that poses a global health risk. It is often underestimated and misdiagnosed, despite affecting billions worldwide. HEV has emerged as a global pathogen, with cases reported in both developing and advanced countries. Outbreaks arise when individuals consume water that is contaminated in regions lacking adequate sanitation measures.Factors like population density and limited access to clean water contribute to these outbreaks. Hepatitis E prevalence varies by region, with Africa having the highest rates. Underdeveloped countries have emerging cases of HEV-1 and HEV-2, while developed countries face HEV-3 and HEV-4. In Pakistan, people with weak immune defense systemshave a maximum chance of being affected by HEV. However, the chances of HEV infection in immune people are minimal. The acceptance of contagious food, close contact with infected animals, and blood transfusions are also reasons for HEV transmission. Identification of infected individuals can be challenging due to asymptomatic cases. Treatment mainly involves supportive measures, although severe cases may require ribavirin. A natural recovery without treatment is also possible.
Introduction
In recent times, the emergence of contagious diseases has become a significant risk to the overall safety of public health worldwide [1]. Regrettably, the majority of newly appearing infectious diseases stem from RNA viruses [2]. HEV is an RNA virus that causes hepatitis E, a disease characterized by inflammation of the liver. It is worth noting that hepatitis E has a significant global impact, with an estimated occurrence in approximately 2.3 billion individuals based on seroprevalence information [3]. In Pakistan, HEV primarily affects immunocompromised people, with pregnant women being the most vulnerable. Every year, 10 million pregnancies in Pakistan are recorded as being at risk from HEV. Significantly, a quarter of pregnant women who contract HEV during the third trimester face a fatal outcome [4, 5]. The Hepatitis E virus is acknowledged as the fifth member in the family of hepatitis viruses, following A, B, C, and D. While HEV is recognized as the emerging factor behind the global prevalence of acute viral hepatitis, demonstrating its widespread prevalence [6, 7]. It has been uncovered that an estimated number exceeding 20 million individuals in nine different regions worldwide have experienced hepatitis E. Notably, East and South Asia contribute to the majority, comprising over 61% of all reported cases [8]. In a separate report from the Southeast Asia Regional Office of the World Trade Organization, it is stated that there are approximately 6.5 million symptomatic cases of this disease. The annual mortality rate for diagnosed cases is estimated at 160,000, and Asia alone has reported over 2,700 cases of stillbirth [9].
Nevertheless, despite the concerning statistics mentioned above, hepatitis E remains significantly underestimated. Physicians generally lack sufficient awareness about this disease, resulting in infrequent routine screenings in hospitals worldwide. Hepatitis E is thus frequently misdiagnosed or never diagnosed. Additionally, there is a dearth of knowledge on the disease’s mode of transmission, particularly in wealthy nations. This information gap results from specialists’ original assumption that hepatitis E mostly affects underdeveloped nations.
HEV has gained widespread recognition as an emerging pathogen that presents a grave risk to public health worldwide [10]. Instances of HEV infection were indeed documented exclusively in developing regions such as Africa, Asia, and Mexico. Nonetheless, isolated cases can also be observed in both developing and advanced countries [11]. While the prevalence of the disease is mainly concentrated in certain regions of Asia and Africa, recent research findings have indicated occasional cases of locally transmitted infections and significant rates of antibody presence in developed countries [12, 13]. Hepatitis E has undergone a significant transformation, transitioning from a self- limiting gastrointestinal illness to a complex, multifaceted, and chronic disease. The transition from being a regional affliction to emerging as a worldwide health issue has broadened its impact significantly [14].
Virology
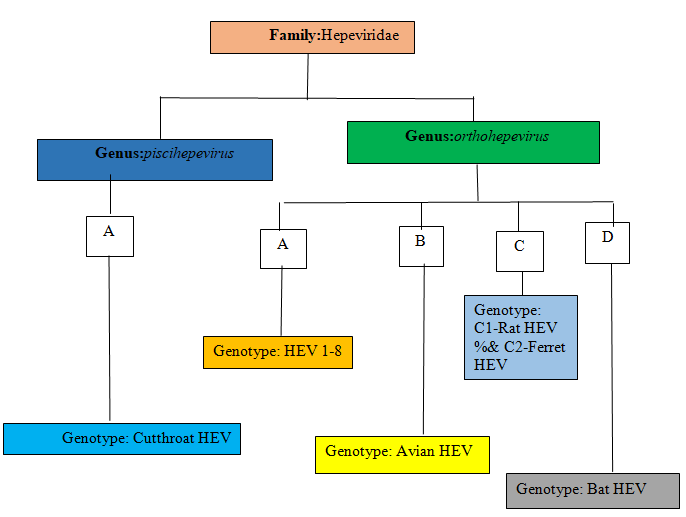
HEV is a type of virus that belongs to a group called orthohepeviruses. This group is part of a larger family called Hepeviridae. Orthohepevirushas four different types called species A, B, C, and D. The strains of species A are the ones that can cause diseases in humans. Within species A, there are eight different variations called genotypes [15, 16]. Two of these cause diseases only in humans (HEV1 and HEV2), while two can infect animals and then spread to humans (HEV3 and HEV4). The other types of the virus seem to mainly affect wild boars (HEV5 and HEV6) and camels (HEV7 and HEV8), but there has been one documented case of a person getting infected with HEV7 [17].
HEV is a virus with a specific shape and genetic material called RNA. Its genome is about 7.2 kilobases long and contains three sections called open reading frames (ORFs). These ORFs provide instructions for making different proteins. One protein is responsible for copying the virus’s RNA (ORF1), another forms the protective outer shell of the virus (ORF2), and the third helps release the virus from infected cells (ORF3). Although ORF2 has been extensively studied because it triggers an immune response, the role of the less understood ORF3 protein is believed to be important in how the virus interacts with the immune system of the infected host [18].
The complete mechanism responsible for the encapsulation of HEV particles remains unclear, although the involvement of ORF3 appears to be of significant importance [19]. Experts have proposed that bile, a substance produced in our bodies, might have the ability to break down the protective covering of HEV viruses. This could be the reason why we observe virus particles without their outer covering in bile and feces [20].
The special type of HEV viruses, called quasi-enveloped virions, doesn’t have certain proteins on their outer surfaces. Because of this, antibodies that are designed to neutralize these viruses by targeting those specific proteins (called anti- ORF2 antibodies) cannot work against them [19]. By using quasi-enveloped forms, HEV can avoid the immune response of its current host and increase its ability to infect new hosts.
Pathogenesis
The exact mechanisms underlying the development of hepatitis E are not yet fully comprehended. How the virus particles reach the liver, given that transmission occurs through the fecal-oral route, is still uncertain. However, recent findings have shed some light on this matter. Studies have demonstrated that HEV1 and HEV3 replication can occur in primary cultures of intestinal cells. Furthermore, in a patient suffering from a persistent infection, researchers have detected HEV RNA and ORF2 antigen specifically in the intestinal crypts. These findings offer significant knowledge regarding the precise distribution and plausible replication locations of the virus within the human body [21].
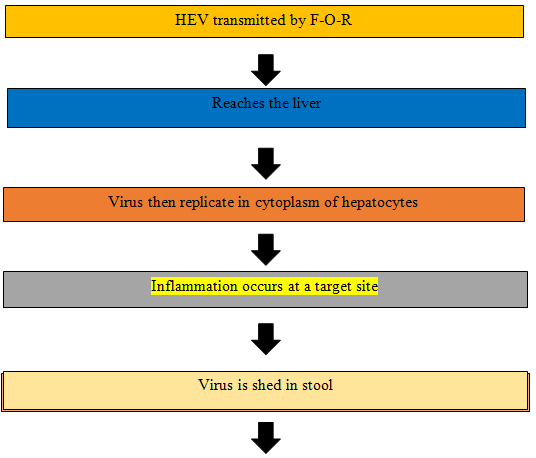
Based on the research findings, it is suggested that HEV undergoes an initial replication process within the gastrointestinal tract. Following this, it enters the liver via the bloodstream while being enclosed in a quasi-enveloped form. Once inside hepatocytes, HEV can replicate within the cytoplasm and then be released into the bloodstream and bile as particles associated with lipids. Capelli N, et al. [22] conducted a study using polarized hepatocytes in a controlled laboratory environment, revealing that the majority of HEV particles are discharged from the apical membrane, which corresponds to the side facing the bile [22]. Bile salts play a vital role in eliminating fats from the virus expelled through feces. The liver cells are not directly harmed by the HEV itself; instead, an HEV infection may induce liver damage through the immune response facilitated by cytotoxic T cells and natural killer cells [23].
Outbreaks
The primary cause of outbreaks stems from the consumption and utilization of polluted water in environments characterized by inadequate sanitary and hygienic conditions [24]. The initial recorded instance of a verified HEV outbreak was documented in Delhi in 1955. After that, several outbreaks have been documented in countries with warm temperatures, including tropical and subtropical regions. These outbreaks have predominantly occurred in countries across Asia and Africa. Among the most significant outbreaks were the ones in Kanpur, India, between 1990 and 1991, which affected around 79,000 individuals, and the outbreak in China between 1986 and 1988, which affected approximately 119,000 people [25, 26]. A new study has used modeling techniques to identify the best areas for HEV viruses to thrive in nature. They found that the Ganges Valley in India and Pakistan is one of the most suitable places for these viruses to exist [27]. Several key factors have a significant role in causing outbreaks of HEV that are related to water. These factors include how many people live in a particular area, the economic and social conditions of the population, the quality of sanitation practices, and the availability of safe drinking water [24, 27]. To stop HEV outbreaks, we can prevent them by making sure places have good hygiene and people can easily get clean drinking water. See Table 1-5 for outbreaks in India, Pakistan, Bangladesh, Uganda, and the Central African Republic, respectively, that occur most frequently in India and have different modes of transmission, as well as different modes of transmission in Pakistan, that affect thousands of people annually.
| Mode of Transmission | Year | References | |
|---|---|---|---|
| 82 | Waterborne | 1998 | [28] |
| 185 | Contaminated water | 2002 | [29] |
| 538 | Drinking untreated raw river water | 2004 | [30] |
| 429 | Contaminated drinking water | 2005 | [31] |
| 64 | Fecal contamination of water resources | 2007-2008 | [32] |
| 23915 | Sewage contamination of the river | 2008 | [33] |
| 442 | Waterborne | 2005-2010 | [34] |
| 102 | Waterborne | 2010 | [35] |
| 180 | Fecal contamination of drinking water | 2012 | [36] |
| 240 | Sewage contamination of drinking water | 2013 | [37] |
| 17 | Waterborne | 2014-2016 | [38] |
| Reported Cases | Mode of Transmission | Year | References |
| 3827 | Waterborne | 1993-1994 | [39] |
| 104 | Fecal contamination—water system | 1998 | [40] |
| 300 | Waterborne | 2019 | [41] |
| 14 | Parental to child | 2022 | [42] |
Table 1: Outbreak in India.
| Mode of Transmission | Year | References | |
|---|---|---|---|
| 4751 | Sewage contamination—municipal water | 2009-2012 | [43] |
| 200 | Waterborne | 2010 | [44] |
| 103 | Waterborne | 2014-2015 | [45] |
| 661 | Waterborne | 2014-2017 | [46] |
Table 2: Outbreak in Bangladesh.
| Mode of Transmission | Year | References | |
|---|---|---|---|
| 146 | Waterborne | 2007-2009 | [47] |
| >10,000 | Substantialperson-to-person | 2008 | [48-50] |
| 987 | Contaminated water | 2009-2012 | [51] |
Table 3: Outbreak in Uganda.
| Reported Cases | Mode of Transmission | Year | References |
|---|---|---|---|
| 213 | Rainy season | 2004 | [52] |
| 745 | Waterborne | 2008-2012 | [53] |
| 149 | Waterborne | 2018 | [54] |
Table 4: Outbreak in the Central African Republic.
Epidemiology
Developing nations exhibit a higher prevalence of HEV antibodies in their populations in contrast to developed countries [55]. Africa has the highest rate of people who have antibodies against HEV, with about 21.76% of the population testing positive. Asia follows with 15.80%, Europe with 9.31%, North America with 8.05%, South America with 7.28%, and Oceania with 5.99%. When considering IgM antibodies, the prevalence is comparatively reduced.In Africa, about 3.09% of the population has IgM antibodies against HEV. In Asia, it’s 1.86%; in Europe, it’s 0.79%; in North America, it’s 0.22%; and in South America, it’s 2.43% [56]. Four main types of genotypes can make people sick, and two of them, called HEV-1 and HEV-2, are mostly present in underdeveloped countries. These genotypes are usually spread through water that has been contaminated with feces, but sometimes they can also be passed from one person to another or from a mother to her baby [57]. In Table 6, the strains of HEV that are of the A (HEV 1-8) genotype have global epidemiology.
Hepatitis E is a type of liver inflammation that usually happens in outbreaks or isolated cases.Teenagers and young adults tend to experience this occurrence more frequently. When we look at different age groups, the estimated rate of hepatitis E infection is around 0.5% to 1.0% for children aged 0 to 15 years. The rates increase to about 1.0% to 1.4% for those aged 15 to 20 years but then drop quickly to a lower rate of 0.2% or less for people older than 30 years [8]. HEV-3 is the main cause of local infections in developed countries, while HEV-4 is mostly found in Asia and occasionally in Europe [58, 59]. These viruses often spread when we eat contaminated food, come into close contact with infected animals, or receive a blood transfusion from someone with the virus in their blood [60].
| Transmission Route | Genotype | Host | |
|---|---|---|---|
| India, Pakistan, Bangladesh, Myanmar, China, | F-O-R | HEV-1 | Human, primates |
| Mexico, Nigeria | F-O-R | HEV-2 | Human, primates |
| Industrialized countries | Zoonotic transmission contaminated blood | HEV-3 | Human, pig, wild boar, rabbit. |
| Asian countries | Zoonotic transmission / contaminated blood | HEV-4 | Human, pig, wild boar, cow, Rhesus monkey |
| UAE | Zoonotic | HEV-7 | Human dromedary camel |
Table 5: The following table is Orthohepevirus Genotype A epidemiology in Global [61].
Transmission
HEV is mainly transmitted through the fecal-oral pathway. In less developed areas, HEV genotypes 1 and 2 often propagate through the contamination of water sources, leading to significant outbreaks and epidemics. On the other hand, in industrialized or developed regions where HEV genotypes 3 and 4 are more common, transmission to humans is primarily associated with consuming animal products that are contaminated, such as raw meat or liver. It’s important to mention that, apart from the fecal-oral route, new transmission routes have been discovered in recent times [62]. HEV particles and the capsid protein linked to HEV were detected in the urine of rhesus macaques infected with the virus as well as in individuals who have compromised immune systems. An experiment of significance demonstrated the successful transmission of HEV to monkeys by injecting them with urine from a monkey infected with HEV. This experiment underscored the potential for HEV to be transmitted orally through urine [63, 34].
The global incidence of HEV infection transmitted through blood has garnered significant international concern. Numerous instances of HEV infection resulting from transfusions have been extensively documented, particularly among immunosuppressed individuals, potentially leading to the development of chronic hepatitis E. Vertical transmission of HEV can take place and is mainly attributed to genotype 1 HEV. Additionally, HEV genotypes 3 and 4 have demonstrated the potential for vertical transmission in animal models, including rabbits and rhesus macaques [65, 66].
The transmission of HEV from mother to child can result in newborns developing jaundice shortly after birth. Generally, this leads to a mild and temporary illness for infants, without any long-lasting effects. However, in some cases, it can be fatal within 48 hours due to severe complications such as hypothermia, hypoglycemia, or rapid liver failure. Researchers also have identified HEV RNA in semen samples of individuals with chronic HEV infection, suggesting a potential for sexual transmission of the virus [67].
Diagnosis
There are various techniques accessible for identifying HEV, both through direct and indirect means. These techniques encompass IEM, fluorescent antibody blocking assay, EIA, immunoblot (IB), immune chromatography, and RT-PCR [68]. Following exposure and subsequent infection with HEV, there is an incubation period ranging from 15 to 60 days. Roughly three weeks following infection, the detection of HEV RNA is possible in both fecal and blood specimens [69]. HEV RNA becomes detectable just before the onset of clinical symptoms, and after four weeks after infection, Immunoglobulin M (IgM) antibodies start to emerge, followed by the appearance of IgG antibodies a few days later [70]. The presence of the virus in the bloodstream can persist for a period of three to six weeks, while the excretion of the virus in feces can continue for four to six weeks [71, 72]. IgM antibodies can typically be detected in the body for a period of three to four months following the initial infection with HEV. On the other hand, IgG antibodies remain present in the system for an extended duration, lasting for years after the primary HEV infection [73].
The detection of HEV RNA through molecular testing involves the utilization of NAAT-based assays. These assays employ the reverse transcription PCR method to detect and amplify RNA [74, 75]. Traditional testing methods focus on identifying highly conserved regions of ORF2 and ORF3 to detect all four genotypes of HEV [76]. Polymorphisms have led to misleading negative outcomes, but incorporating a minor modification in minor groove binding alleviates this issue by improving sensitivity [77]. Molecular tests are used to identify HEV RNA in blood or stool, indicating an active HEV infection. Persistent HEV RNA for at least three months confirms chronic hepatitis E. Molecular tests are preferred over antibody tests for screening immunocompromised patients due to the potential undetectability of antibodies. Thus, detecting HEV RNA is the most effective diagnostic approach in such cases.
Diagnosing Acute HEV infection involves detecting anti-HEV antibodies. IgM antibodies appear shortly after symptoms or approximately four weeks after exposure, followed by IgG antibodies in a few days, persisting for years. Serologic testing combines enzyme immunoassays with HEV NAAT to detect antibodies. Anti-HEV IgM and IgA testing increase diagnostic sensitivity. In a study of 60 HEV patients with positive IgM and IgA tests, all also tested positive for HEV RNA [78].
There are specific limitations to this approach that need to be acknowledged. Firstly, it may not be suitable for individuals who are unable to produce antibodies, thereby rendering it ineffective for such patients. Secondly, individuals who are undergoing long-term immunosuppressive therapy are not optimal candidates for this particular testing method [56]. Additionally, there probably exists a considerable chance of cross-reactivity between EBV (Epstein-Barr virus) and CMV (Cytomegalovirus) in antibody tests. More specifically, in samples that tested positive for HEV (Hepatitis E virus) IgM antibodies, approximately 33.3% of them were also detected as positive for EBV, whereas 24.2% showed positivity for CMV [79].
Enzyme immunoassays are a dependable method for detecting HEV antigens, which prove useful in diagnosing both acute and chronic cases of the infection. However, it is important to note that these tests have shown lower positivity rates in comparison to RT-PCR tests. Specifically, the positivity rates for sera and stool samples were observed to be 55% and 76%, respectively. It is worth mentioning that enzyme immunoassays can still show elevated results in stool samples even after the HEV RNA becomes negative, indicating that the presence of HEV antigens does not necessarily correlate with the presence of infectious HEV virions [80].
The utilization of immunochemistry in the examination of the HEV ORF2 protein has been valuable for hepatitis E diagnosis. The presence of open reading frames 1 and 3 in cells has been observed, although at times their traceability or detectability has been uncertain and inconclusive [81].
Treatment
The majority of individuals diagnosed with acute hepatitis E tend to recover naturally without the requirement for any specific treatment, apart from supportive measures aimed at alleviating symptoms. In rare documented cases, patients suffering from severe AHE have received ribavirin as a treatment option, resulting in positive changes in laboratory indicators and a reduction in HEV RNA levels [82, 83]. However, without implementing any measures to regulate the situation, it is not feasible to attribute this enhancement solely to the medication, leaving room for the possibility that the recovery occurred naturally.
Patients diagnosed with chronic hepatitis E have two potential therapeutic approaches based on available observational data. The first approach involves restoring the patient’s immune status by either reducing the dosage or discontinuing the use of immunosuppressant drugs. Additionally, in HIV-positive individuals, antiretroviral therapy may be administered to achieve the same goal. The second approach involves the administration of either ribavirin or PEGylated interferon. It is worth noting that the first approach has been linked to HEV clearance in approximately one-third of the patients [84]. Although there is a possibility of the transplanted organ being rejected, it is still recommended as the preferred method whenever feasible. In cases where this method is not an option or proves ineffective in eliminating HEV infection, oral ribavirin seems to be the most suitable medication.
Ribavirin treatment has proven to be effective in managing chronic HEV infection in individuals with weakened immune systems, such as those who have received solid organ or bone marrow transplants.The use of ribavirin in solid-organ graft patients with persistent hepatitis E was investigated in a retrospective, multi-center investigation. The patients received a median dose of approximately 8.1 mg/kg of ribavirin for 3 months. Results showed that 78% of the 59 patients achieved a sustained virological response, meaning that their serum HEV RNA levels remained undetectable six months after discontinuing ribavirin. The most commonly reported adverse event was anemia, which often required adjustments in ribavirin dosage, administration of erythropoietin, or blood transfusions [85]. The existing information does not provide precise guidelines regarding the specific dosage and duration of ribavirin treatment.
The complete understanding of how ribavirin works in treating HEV infection remains unclear. However, it seems to hinder HEV replication by reducing the available supply of guanosine triphosphate within the cells [86]. Alternative suggestions have been put forth, involving various mechanisms such as the modulation of the immune system, enhanced activation of interferon-stimulated genes, induction of viral mutagenesis, and the thwarting of viral replicative processes [87]. The dynamics of viral replication while undergoing ribavirin treatment could serve as an indicator of the prognosis of chronic HEV infection. According to a published study, a reduction of 0.5 log10 copies/mL or more in HEV RNA levels after 7 days of ribavirin therapy appeared to be a reliable predictor of a sustained virological response [88].
A G1634R mutation in the polymerase region of the HEV RNA was discovered in two individuals who had ongoing HEV infections and did not respond to ribavirin therapy. The mutation was observed to enhance viral replication in an in vitro system, but there was no evidence of it causing drug resistance [89].
Prevention
In areas where waterborne infections are prevalent, the key approach to preventing such diseases revolves around enhancing sanitation measures and access to safe drinking water [90, 91]. Research has demonstrated a clear link between the lack of intervention in sterilizing drinking water during epidemics and the subsequent occurrence of more widespread outbreaks [25]. In regions where zoonotic transmission is prevalent, it is crucial to take appropriate measures in the preparation of food items to prevent infections. Vulnerable individuals, including women who are expecting, those with liver issues, and others with weakened immune systems, need to exercise caution and refrain from consuming raw meat, To ensure safety, it is advised for individuals involved in the handling of pigs, wild boar, and related products to minimize direct interaction and employ protective gear [92]. China has made a highly efficient vaccine accessible to the public for nearly six years [93]. The purpose of developing this vaccine is to provide extended safeguarding against all variants of HEV. However, the approval for worldwide implementation is still pending, as additional phase IV trials are necessary to evaluate its safety in specific groups, such as children, the elderly, individuals with weakened immune systems, and those with pre-existing liver conditions [94, 95].
Conclusion
Hepatitis E virus (HEV) affects people globally and is an emerging killer, particularly in underdeveloped countries due to poor sanitation systems. Another big reason in underdeveloped countries is the high annual pregnancy rate, which is a leading factor for immunocompromization. Hepatitis E has become prevalent in immunocompromised people and leads to death. It is needed to emphasize awareness and increase public health care, as well as understanding the virology, pathogenesis, and outbreak it, which are crucial factors for prevention and control strategies to mitigate the infection of that emerging killer. Underdeveloped countries need to take steps like developed countries to overcome its futuristic dangerous effect on their precious people’s lives.
References
-
Parvez MK, Arabia S (2013) Emerging and reemerging viral diseases risks and controls. Microbial pathogens and strategies for combating them science technology and education, pp: 1619-1626.
-
Nichol ST, Arikawa J, Kawaoka Y (2000) Emerging viral diseases. Proceedings of the National Academy of Sciences 97(23): 12411-12412.
-
Guerra JA, Kampa KC, Morsoletto DG, Junior AP, Ivantes CA (2017) Hepatitis E: A Literature Review. J Clin Transl Hepatol 5(4): 376-383.
-
Aparna S, Rubina H, Zeba S, Sabahat H, Emma P, et al. (2023) Adding It Up Costs and Benefits Of Meeting the Contraceptive and Maternal and Newborn Health Needs of Women in Pakistan. Reproductive health, pp: 24.
-
Chaudhry SA, Verma N, Koren G (2015) Hepatitis E infection during pregnancy. Can Fam Physician 61(7): 607-608.
-
Melgaço JG, Gardinali NR, Leal M, De Mello VM, Pinto MA, et al. (2018) Hepatitis E: Update on Prevention and Control. BioMed Research International 2018: 5769201.
-
Teshale EH, Hu DJ (2011) Hepatitis E Epidemiology and prevention. World J Hepatol 3(12): 285-291.
-
Rein DB, Stevens GA, Theaker J, Wittenborn JS, Wiersma ST, et al. (2012) The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology 55(4): 988-997.
-
Hudu SA, Niazlin MT, Nordin SA, Harmal NS, Tan SS, et al. (2018) Hepatitis E virus isolated from chronic hepatitis B patients in Malaysia Sequences analysis and genetic diversity suggest zoonotic origin. Alexandria Journal of Medicine 54(4): 487-494.
-
Webb GW, Dalton HR (2019) Hepatitis E: an underestimated emerging threat. Ther Adv Infect Dis 6: 2049936119837162.
-
Aggarwal R (2011) Hepatitis E Historical contemporary and future perspectives. Journal of Gastroenterology and Hepatology 26: 72-82.
-
Lewis HC, Wichmann O, Duizer E (2010) Transmission routes and risk factors for autochthonous hepatitis E virus infection in Europe: a systematic review. Epidemiol Infect 138(2): 145-166.
-
Capai L, Falchi A, Charrel R (2019) Meta-Analysis of Human IgG anti-HEV Seroprevalence in Industrialized Countries and a Review of Literature. Viruses 11(1): 84.
-
Harrison LC, Di CE (2018) Hepatitis E Virus An Emerging Foodborne Pathogen. Frontiers in Sustainable Food Systems 2.
-
Purdy MA, Harrison TJ, Jameel S, Meng XJ, Okamoto H, et al. (2017) ICTV Virus Taxonomy Profile Hepeviridae. J Gen Virol 98(11): 2645-2646.
-
Smith DB, Simmonds P, Jameel S, Emerson SU, Harrison TJ, et al. (2014) Consensus proposals for classification of the family Hepeviridae. J Gen Virol 95(10): 2223-2232.
-
Lee GH, Tan BH, Teo EC, Lim SG, Dan YY, et al. (2016) Chronic Infection with Camelid Hepatitis E Virus in a Liver Transplant Recipient Who Regularly Consumes Camel Meat and Milk. Gastroenterology 150(2): 355- 357.
-
Debing Y, Moradpour D, Neyts J, Gouttenoire J (2016) Update on hepatitis E virology Implications for clinical practice. J Hepatol 65(1): 200-212.
-
Takahashi M, Tanaka T, Takahashi H, Hoshino Y, Nagashima S, et al. (2010) Hepatitis E Virus HEV strains in serum samples can replicate efficiently in cultured cells despite the coexistence of HEV antibodies characterization of HEV virions in blood circulation. J Clin Microbiol 48(4): 1112-1125.
-
Yin X, Li X, Feng Z (2016) Role of Envelopment in the HEV Life Cycle. Viruses 8(8): 229.
-
Marion O, Lhomme S, Nayrac M, Dubois M, Pucelle M, et al. (2020) Hepatitis E virus replication in human intestinal cells. Gut 69(5): 901-910.
-
Capelli N, Dubois M, Allart S, Lhomme S, Marion O, et al. (2019) Vectorial Release of Hepatitis E Virus in Polarized Human Hepatocytes. J Virol 93(4): e01207-e01218.
-
Fields BN, Knipe DM, Howley PM (2013) Fields Virology. 6th(Edn.), Lippincott Williams & Wilkins Philadelphia, PA, USA, pp: 2664.
-
Khuroo MS, Khuroo MS, Khuroo NS (2016) Transmission of Hepatitis E Virus in Developing Countries. Viruses 8(9): 253.
-
Naik SR, Aggarwal R, Salunke PN, Mehrotra NN (1992) A large waterborne viral hepatitis E epidemic in Kanpur, India. Bull World Health Organ 70(5): 597-604.
-
Bi SL, Purdy MA, Mccaustland KA, Margolis HS, Bradley DW, et al. (1993) The sequence of hepatitis E virus isolated directly from a single source during an outbreak in China. Virus Res 28(3): 233-247.
-
Carratalà A, Joost S (2019) Population density and water balance influence the global occurrence of hepatitis E epidemics. Sci Rep 9(1): 10042.
-
Aggarwal R, Kumar R, Pal R, Naik S, Semwal SN, et al. (2002) Role of travel as a risk factor for hepatitis E virus infection in a disease endemic area. Indian J Gastroenterol 21(1): 14-18.
-
Banerjee A, Sahni A, Rajiva, Nagendra A, Saiprasad G, et al. (2005) Outbreak of Viral Hepatitis E in a Regimental Training Centre. Med J Armed Forces India 61(4): 326- 329.
-
Swain SK, Baral P, Hutin YJ, Rao TV, Murhekar M, et al. (2010) A hepatitis E outbreak caused by a temporary interruption in a municipal water treatment system Baripada Orissa India 2004. Trans R Soc Trop Med Hyg 104(1): 66-69.
-
Sarguna P, Rao A, Ramana SKN (2007) Outbreak of acute viral hepatitis due to hepatitis E virus in Hyderabad. Indian J Med Microbiol 25(4): 378-382.
-
Khuroo MS, Khuroo MS (2010) Seroepidemiology of a second epidemic of hepatitis E in a population that had recorded the first epidemic 30 years before and has been under surveillance since then. Hepatol Int 4(2): 494-499.
-
Vivek R, Nihal L, Illiayaraja J, Reddy PK, Sarkar R, et al. (2010) Investigation of an epidemic of Hepatitis E in Nellore in south India. Trop Med Int Health 15(11): 1333-1339.
-
Karna R, Hazam RK, Borkakoti J, Kumar A, Kar P, et al. (2020) A 5 year Single Center Experience of Hepatitis E Virus Infection During Pregnancy. J Clin Exp Hepatol 10(2): 135-138.
-
Majumdar M, Singh MP, Pujhari SK, Bhatia D, Chawla Y, et al. (2013) Hepatitis E virus antigen detection as an early diagnostic marker report from India. J Med Virol 85(5): 823-827.
-
Tambe MP, Patil SP, Dravid M, Bhagwat VR (2015) Investigation of an Outbreak of Hepatitis E in a Rural Area of Dhule District in Maharashtra. JKIMSU 4(1): 109- 114.
-
Awsathi S, Rawat V, Rawat CMS, Semwal V, Bartwal SJ, et al. (2014) Epidemiological investigation of the jaundice outbreak in Lalkuan Nainital district Uttarakhand. Indian J Community Med 39(2): 94-97.
-
Goel A, Padmaprakash KV, Benjamin M, Katiyar H, Aggarwal R, et al. (2020) Temporal profile of HEV RNA concentration in blood and stool from patients with acute uncomplicated hepatitis E in a region with genotype 1 predominance. J Viral Hepat 27(6): 631-637.
-
Rab MA, Bile MK, Mubarik MM, Asghar H, Sami Z, et al. (1997) Water borne hepatitis E virus epidemic in Islamabad, Pakistan a common source outbreak traced to the malfunction of a modern water treatment plant. Am J Trop Med Hyg 57(2): 151-171.
-
Bryan JP, Iqbal M, Tsarev S, Malik IA, Duncan JF, et al. (2002) Epidemic of hepatitis E in a military unit in Abbottabad Pakistan. Am J Trop Med Hyg 67(6): 662- 668.
-
Salman M, Mustafa ZUL, Asif N (2019) Hepatitis E outbreak in the province of Punjab Pakistan a call for action. Infect Dis Lond 51(8): 633-634.
-
Khan SA, Khan Z, Alam Z, Sana H, Ali M, et al. (2022) Hepatitis E virus seroprevalence among pregnant women in Khyber Pakhtunkhwa Pakistan. Clinical Immunology Communications 2: 79-82.
-
Gurley ES, Hossain JM, Paul RC, Sazzad HMS, Islam MS, et al. (2014) Outbreak of hepatitis E in urban Bangladesh resulting in maternal and perinatal mortality. Clin Infect Dis 59(5): 658-665.
-
Kayesh MEH, Kohara M, Kohara TK (2022) Epidemiology and Risk Factors for Acute Viral Hepatitis in Bangladesh An Overview. Microorganisms 10(11): 2266.
-
Khan AI, Salimuzzaman M, Islam T, Afrad MH, Shirin T, et al. (2020) Nationwide Hospital Based Seroprevalence of Hepatitis A and Hepatitis E Virus in Bangladesh. Ann Glob Health 86(1): 29.
-
Paul RC, Nazneen A, Banik KC, Sumon SA, Paul KK, et al. (2020) Hepatitis E as a cause of adult hospitalization in Bangladesh: Results from an acute jaundice surveillance study in six tertiary hospitals 2014-2017. Plos Neglected Tropical Diseases 14(1): e0007586.
-
Gerbi GB, Williams R, Bakamutumaho B, Liu S, Downing R, et al. (2015) Hepatitis E as a cause of acute jaundice syndrome in northern Uganda 2010-2012. Am J Trop Med Hyg 92(2): 411-414.
-
Teshale EH, Howard CM, Grytdal SP, Handzel TR, Barry V, et al. (2010) Hepatitis E epidemic Uganda. Emerg Infect Dis 16(1): 126-129.
-
Teshale EH, Grytdal SP, Howard C, Barry V, Kamili S, et al. (2010) Evidence of person to person transmission of hepatitis E virus during a large outbreak in Northern Uganda. Clin Infect Dis 50(7): 1006-1010.
-
Howard CM, Handzel T, Hill VR, Grytdal SP, Blanton C, et al. (2010) Novel risk factors associated with hepatitis E virus infection in a large outbreak in northern Uganda results from a case control study and environmental analysis. Am J Trop Med Hyg 83(5): 1170-1173.
-
Cummings MJ, Wamala JF, Komakech I, Lukwago L , Malimboet M, et al. (2014) Hepatitis E in Karamoja, Uganda, 2009-2012: Epidemiology and challenges to control in a setting of semi-nomadic pastoralism. Trans R Soc Trop Med Hyg 108(10): 648-655.
-
Goumba AI, X Konamna, Komas NP (2011) Clinical and epidemiological aspects of a hepatitis E outbreak in Bangui, Central African Republic. BMC Infectious Diseases 11(1): 93.
-
Tricou V, Bouscaillou J , Nguembe GLL , Bere A , Konamna X, et al. (2020) Hepatitis E virus outbreak associated with rainfall in the Central African Republic in 2008- 2009. BMC Infect Dis 20(1): 260.
-
Impouma B, Archer BN, Lukoya OC, Hamblion EL, Fal IS (2018) World Health Organization Regional Office for Africa Weekly Bulletin on Outbreaks and Other Emergencies. Emerg Infect Dis 24(7):1394-1395.
-
Kmush B, Wierzba T, Krain L, Nelson K, Labrique AB (2013) Epidemiology of hepatitis E in low- and middle- income countries of Asia and Africa. Semin Liver Dis 33(1):15-29.
-
Li P, Liu J, Li Y, Su J, Ma Z, et al. (2020) The global epidemiology of hepatitis E virus infection: A systematic review and meta-analysis. Liver Int 40(7):1516-1528.
-
Khuroo MS, Khuroo MS, Khuroo NS (2016) Hepatitis E: Discovery, global impact, control and cure. World J Gastroenterol 22(31): 7030-7045.
-
Honing RWH, Coillie EV, Antonis AFG, Poel WHM (2011) First isolation of hepatitis E virus genotype 4 in Europe through swine surveillance in the Netherlands and Belgium. PLoS One 6(8): e22673.
-
Garbuglia AR, Scognamiglio P, Petrosillo N, Mastroianni CM, Sordilloet P, et al. (2013) Hepatitis E virus genotype 4 outbreak, Italy, 2011. Emerg Infect Dis 19(1):110-114.
-
Goel A, Aggarwal R (2020) Hepatitis E: Epidemiology, Clinical Course, Prevention, and Treatment. Gastroenterol Clin North Am 49(2): 315-330.
-
Smith DB, Izopet J, Nicot F, Simmonds P, Jameel S et al. (2020) Update: proposed reference sequences for subtypes of hepatitis E virus (species Orthohepevirus A). J Gen Virol 101(7): 692-698.
-
Liang Z, Wang L, Wang L (2022) Updates on hepatitis E virus. Chin Med J (Engl) 135(10): 1231-1233.
-
Geng Y, Zhao C, Huang W, Harrison TJ, Zhang, H et al. (2016) Detection and assessment of infectivity of hepatitis E virus in urine. J Hepatol 64(1): 37-43.
-
Huang F, Yang C, Zhou X, Yu W, Pan Q, et al. (2016) Rhesus macaques persistently infected with hepatitis E shed virus into the urine. J Hepatol 64(6):1446-1447.
-
Yu W, Hao X, Li Y, Yang C, Li Y, et al. (2020) Vertical transmission of hepatitis E virus in pregnant rhesus macaques. Sci Rep 10(1):17517.
-
Xia J, Liu L, Wang L, Zhang Y, Zeng H, et al. (2015) Experimental infection of pregnant rabbits with hepatitis E virus demonstrating high mortality and vertical transmission. J Viral Hepat 22(10): 850-857.
-
Horvatits T, Wißmann JE, Johne R, Groschup MH, Gadicherla AK, et al. (2021) Hepatitis E virus persists in the ejaculate of chronically infected men. J Hepatol 75(1): 55-63.
-
Raji YE, Toung OP, Taib NM, Sekawi ZB (2022) Hepatitis E Virus: An emerging enigmatic and underestimated pathogen. Saudi J Biol Sci 29(1): 499-512.
-
Kamani L, Padhani ZA, Das JK (2021) Hepatitis E: Genotypes, strategies to prevent and manage, and the existing knowledge gaps. JGH Open 5(10):1127-1134.
-
Khuroo MS, Kamili S, Dar MY, Moecklii R, Jameel S, et al. (1993) Hepatitis E and long-term antibody status. Lancet 341(8856): 1355.
-
Takahashi M, Tanaka T, Azuma M, Kusano E, Aikawa T, et al. (2007) Prolonged fecal shedding of hepatitis E virus (HEV) during sporadic acute hepatitis E: evaluation of infectivity of HEV in fecal specimens in a cell culture system. J Clin Microbiol 45(11): 3671-3679.
-
Chandra NS, Sharma A, Malhotra B, Rai RR (2010) Dynamics of HEV viremia, fecal shedding and its relationship with transaminases and antibody response in patients with sporadic acute hepatitis E. Virol J 7: 213.
-
Dawson GJ, Mushahwar IK, Chau KH, Gitnick GL (1992) Detection of long-lasting antibody to hepatitis E virus in a US traveler to Pakistan. Lancet 340(8816): 426-427.
-
Jothikumar N, Cromeans TL, Robertson BH, Meng XJ, Hill VR, et al. (2006) A broadly reactive one-step real- time RT-PCR assay for rapid and sensitive detection of hepatitis E virus. J Virol Methods 131(1): 65-71.
-
Baylis SA, Hanschmann KM, Blümel J, Nübling CM (2011) Standardization of hepatitis E virus (HEV) nucleic acid amplification technique-based assays: an initial study to evaluate a panel of HEV strains and investigate laboratory performance. J Clin Microbiol 49(4): 1234-1239.
-
Baylis SA, Blümel J, Mizusawa S, Matsubayashi K, Sakata H, et al. (2013) World Health Organization International Standard to harmonize assays for detection of hepatitis E virus RNA. Emerg Infect Dis 19(5): 729-735.
-
Garson JA, Ferns RB, Grant PR, Ijaz S, Nastouli E, et al. (2012) Minor groove binder modification of widely used TaqMan probe for hepatitis E virus reduces the risk of false negative real-time PCR results. J Virol Methods 186(1-2): 157-160.
-
Zhao C, Geng Y, Harrison TJ, Huang W, Song A, et al. (2015) Evaluation of an antigen-capture EIA for the diagnosis of hepatitis E virus infection. J Viral Hepat 22(11): 957-963.
-
Hyams C, Mabayoje DA, Copping R, Maranao D, Patel M, et al. (2014) Serological cross-reactivity to CMV and EBV causes problems in the diagnosis of acute hepatitis E virus infection. J Med Virol 86(3): 478-483.
-
Montpellier C, Wychowski C, Sayed IM, Meunier JC, Saliou JM, et al. (2018) Hepatitis E Virus Lifecycle and Identification of 3 Forms of the ORF2 Capsid Protein. Gastroenterology 154(1): 211-223.
-
Lenggenhager D, Gouttenoire J, Malehmir M, Bawohl M, Honcharova-Biletska H, et al. (2017) Visualization of hepatitis E virus RNA and proteins in the human liver. J Hepatol 67(3): 471-479.
-
Gerolami R, Borentain P, Raissouni F, Motte A, Solas C, et al. (2011) Treatment of severe acute hepatitis E by ribavirin. J Clin Virol 52(1): 60-62.
-
Goyal R, Kumar A, Panda SK, Paul SB, Acharya SK, et al. (2012) Ribavirin therapy for hepatitis E virus-induced acute on chronic liver failure: a preliminary report. Antivir Ther 17(6): 1091-1096.
-
Kamar N, Garrouste C, Haagsma EB, Garrigue V, Pischke S, et al. (2011) Factors associated with chronic hepatitis in patients with hepatitis E virus infection who have received solid organ transplants. Gastroenterology 140(5): 1481-1489.
-
Kamar N, Izopet J, Tripon S, Bismuth M, Hillaire S, et al. (2014) Ribavirin for chronic hepatitis E virus infection in transplant recipients. N Engl J Med 370(12): 1111-1120.
-
Debing Y, Emerson SU, Wang Y, Pan Q, Balzarini J, et al. (2014) Ribavirin inhibits in vitro hepatitis E virus replication through depletion of cellular GTP pools and is moderately synergistic with alpha interferon. Antimicrob Agents Chemother 58(1): 267-273.
-
Paeshuyse J, Dallmeier K, Neyts J (2011) Ribavirin for the treatment of chronic hepatitis C virus infection: a review of the proposed mechanisms of action. Curr Opin Virol 1(6): 590-598.
-
Kamar N, Lhomme S, Abravanel F, Cointault O, Esposito L, et al. (2015) An Early Viral Response Predicts the Virological Response to Ribavirin in Hepatitis E Virus Organ Transplant Patients. Transplantation 99(10): 2124-2131.
-
Debing Y, Gisa A, Dallmeier K, Pischke S, Bremer B, et al. (2014) A mutation in the hepatitis E virus RNA polymerase promotes its replication and associates with ribavirin treatment failure in organ transplant recipients. Gastroenterology 147(5): 1008-1011.
-
Nelson KE, Kmush B, Labrique AB (2011) The epidemiology of hepatitis E virus infections in developed countries and among immunocompromised patients. Expert Rev Anti Infect Ther 9(12): 1133-1148.
-
Haque F, Banu SS, Ara K, Chowdhury IA, Chowdhury SA, et al. (2015) An outbreak of hepatitis E in an urban area of Bangladesh. J Viral Hepat 22(11): 948-956.
-
Schielke A, Ibrahim V, Czogiel I, Faber M, Schrader C, et al. (2015) Hepatitis E virus antibody prevalence in hunters from a district in Central Germany, 2013: a cross-sectional study providing evidence for the benefit of protective gloves during disemboweling of wild boars. BMC Infect Dis 15: 440.
-
Zhu FC, Zhang J, Zhang XF, Zhou C, Wang ZZ, et al. (2010) Efficacy and safety of a recombinant hepatitis E vaccine in healthy adults: a large-scale, randomized, double-blind placebo-controlled, phase 3 trial. Lancet 376(9744): 895-902.
-
Zhang J, Zhang XF, Huang SJ, Wu T, Hu YM, et al. (2015) Long-Term Efficacy of a Hepatitis E Vaccine. New England Journal of Medicine 372(10): 914-922.
-
(2014) Global Advisory Committee on Vaccine Safety, 11-12 June 2014. Wkly Epidemiol Rec 89(29): 325-335.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions